
In the next ten minutes, get ready to:
- Grasp the intricacies of introducing the Hybrid Closed Loop Technology Appraisal within NHS Diabetes services.
- Realise the importance of adopting a fresh perspective.
- Witness the remarkable achievement of Birmingham Children’s Hospital, which has tripled its onboarding speed by focusing on Hybrid Closed Loop Therapy.
- Access a suite of ready-to-use Hybrid Closed Loop tools at your fingertips.
The undeniable benefits of hybrid closed therapy (HCL) are firmly established. Recent data from both UK paediatric and adult pilots further emphasises this, allowing HCL to meet the rigorous cost-effectiveness standards for a technology appraisal (TA).
What’s particularly noteworthy about this appraisal process is that local funding bodies, specifically Integrated Care Boards (ICBs), are legally required to allocate necessary funds within 90 days of an appraisal’s release, but have five years to implement the the TA fully. This means funds are available from April 2024!
This swift action will pave the way for over 100,000 individuals with type 1 diabetes to access HCL. There is a five-year implementation plan where ICB’s must provide funds in this priority order; Children, Young People, Pregnancy, Adults using a pump, Adults new to pump.
This is the most exciting time to be involved in type 1 diabetes care, but first, each service MUST support their ICB in understanding the funds are mandatory. If the ICB says there are no extra funds available, there are. The NHSE is funding up to 75% of the cost initially if accurate numbers on HCL Systems are submitted via the NPDA and NDA audit. Furthermore, even if there are no extra funds, it does not matter. The ICB’s are legally mandated over the next five years to pay for HCL therapy for those who meet the criteria. This means they need to follow this simple process, which you can explain to support them.
- Identify all their medical device and high-cost drug spending.
- Order them in priority of (1) Therapies with a NICE Technology Appraisal, such as NICE TA 943 for HCL Systems (2) Therapies with NICE Guidance (3) Therapies with an International Consensus Guidance (4) Therapies with an Individual Funding Request (IFR).
- Assign available monies in line with the the above priorities.
This is simple, but not necessarily easy.
This would mean funding HCL Systems and decommissioning other therapies. Remember, having a NICE TA means the therapy in question is cost-effective. Therefore, HCL Systems are the best use of the limited funds the ICBs have.
What about therapies that get funding removed?
It puts the ball in their court to build a robust evidence base and push for a NICE TA. We have been waiting for this moment for years in Diabetes Care. Let’s make it count for people with type 1 diabetes and the taxpayer.
However, this presents a tangible challenge for the NHS workforce. We now have the monumental task of integrating all these patients into the new system. Moreover, the TA’s cost analysis doesn’t account for additional staffing, so this massive undertaking has to be managed within the existing thin on-the-ground human resources.
For a clearer picture:
- In 2008, the NICE TA 151 for pump therapy was introduced. Yet, by 2023, only 45,000 patients have adopted insulin pumps. This equates to around 3,000 new users each year.
- Continuing at this pace, it will take a substantial 30 years to accommodate over 100,000 patients—a duration that’s simply unacceptable.
- Adult centres will cater to between 500-1500 qualifying individuals. Given the current onboarding rate of about 50 patients per year, this translates to a 10-30 year wait time for each facility.
- For paediatric centres, with 100-400 eligible patients, the current onboarding rate is approximately 20-60 patients annually, leading to a 5-10 year wait.
If the NHS rolls out the HCL TA at the 2008 TA 151 pump therapy’s rate, countless patients will be left waiting for this transformative therapy.
A novel approach is essential.
In Birmingham Children’s Hospital, our facility has been privileged to access both pump and CGM funding. This allowed us to transition to HCL with relative ease. However, up until 2023, we too encountered challenges. Annually, we managed to onboard 30-40 patients (20 of whom were renewals). Between April 2021 and April 2023, we initiated only 75 patients on HCL. With around 300 patients, this rate suggested another 6-years until all those eligible are benefitting from a HCL system. Determined to change this, we revamped our approach in April 2023. From April 2023 to January 2024, we successfully onboarded another 120 children with type 1 diabetes onto an HCL system, averaging 13 per month, tripling our on-boarding cadence. We are ambitiously targeting to onboard nearly all patients eligible by the close of 2024.
You can download all our teaching and patient resources, AID presentations, videos, clinic tools, leaflets, etc from this Google Drive.
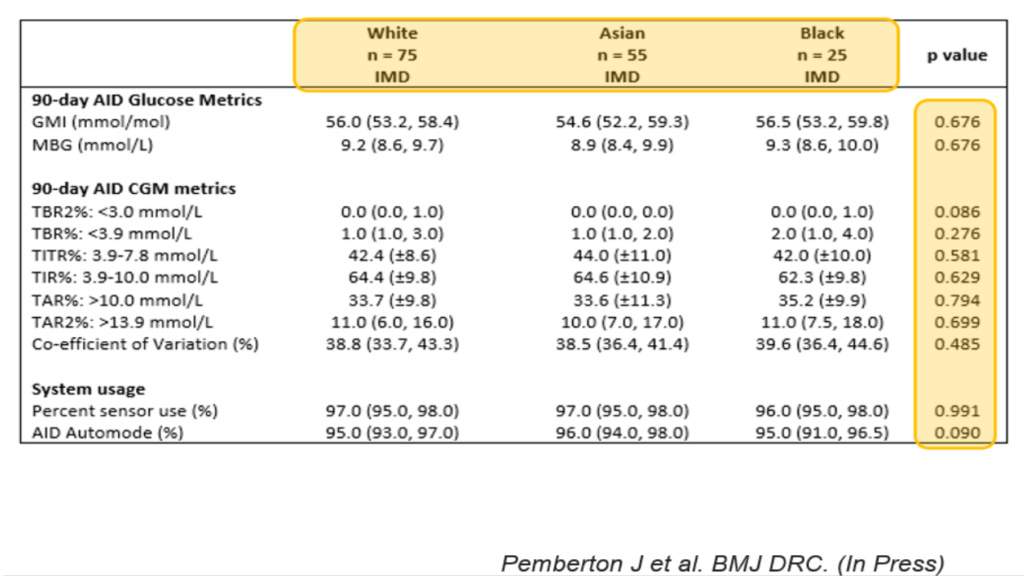
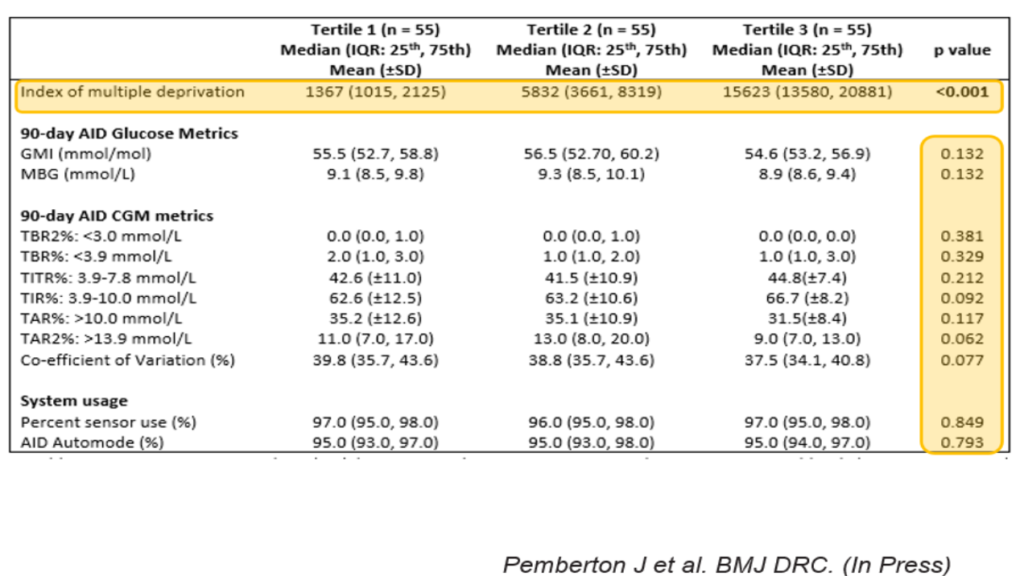
Our results highlight that HCL therapy is pivotal in bridging the gap in glucose control outcomes across ethnic groups and socioeconomic backgrounds. Furthermore, the published results from our virtual hybrid model has been shown to increase HCL access by the most deprived and ethnically diverse children and young people, whilst providing equal glucose control outcomes!
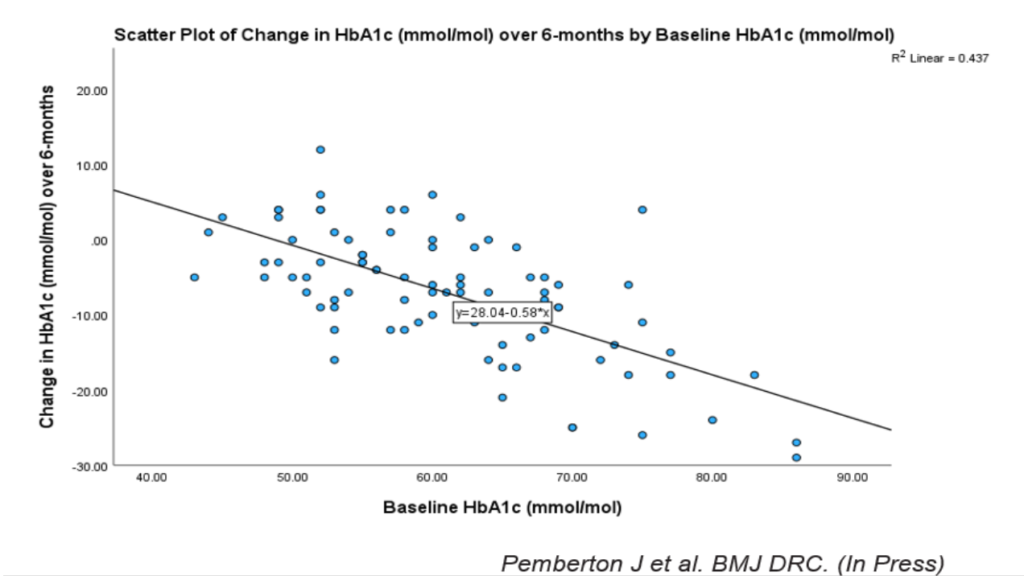
Furthermore, those who start with the highest HbA1c’s get the biggest reductions at 6-months, with no increased risk of DKA.
It’s very important to onboard equitably. Resist the urge to onboard those who demand it first. Look at your population demographics (ethnicity, socioeconomic status, interpreter requirement) and make sure your planned onboarding matches the population your service supports.
I’m excited to unfold our strategy that enabled equitable onboarding and offer valuable resources, aiming to foster innovative approaches and actions. The approach discussed, and the resources available are not perfect. Over four years, they have been crafted through relentless trial and error to meet our local needs. However, your team may be able to benefit from years of graft that may prevent unnecessary duplication.
What is needed first?
First and foremost, embrace HCL as a cohesive unit. It promises unparalleled stability in glucose levels and enhanced patient satisfaction—a sentiment echoed by Dr. Ali Lumb: “HCL provides a huge increase of Time in Happiness for people living with Type 1 Diabetes.”
After attending ISPAD 2022 and ATTD 2023, one message was crystal clear: HCL represents the zenith of type 1 diabetes care. We may never witness such a transformative leap forward again. Therefore, initiating as many people with Type 1 diabetes as possible, both swiftly and safely, is paramount.
Fortunately, we had a service improvement day close to the conferences. Our operations team collaborated closely, dedicating this day to:
- Highlighting the life-altering advantages of HCL,
- Prioritising HCL integration, and
- Implementing actionable plans with clear timelines and accountability measures to make this vision a reality. As the adage goes, and as I fondly recall from a cringeworthy interview, I observed, “Teamwork makes the dream work!”
The service improvement day was immensely successful, revealing three primary objectives:
- Capacity Creation: What can we phase out?
- Pathway Development & Material Creation: This ensures consistent and top-quality training.
- Delivery & Evaluation: Becoming independent of manufacturers and reporting back to the funders.
Here’s our detailed approach, alongside pertinent questions that might assist your service in navigating the road ahead.
Creating Capacity for HCL Onboarding
Here’s a straightforward question:
What activities are you currently engaged in that don’t deliver as much value as onboarding individuals onto HCL?
The reality, A LOT.
There were two primary areas of focus for us:
- Rethinking our high HbA1c clinics: We used to conduct high HbA1c clinics three times a week to offer added support for those with an HbA1c above 64mmol/moL. However, by introducing HCL, individuals can lower their HbA1c levels below 64mmol/mol, eliminating the need for frequent clinics. We’ve optimised by reducing these clinics to once a week, raising the threshold to 69mmol/moL, and reallocating those two sessions to HCL onboarding.
- Revamping our school education program: Traditionally, we invested significant time in educating schools about diabetes and carbohydrate counting. The pandemic taught us the power of online educational tools. Instead of reverting to face-to-face sessions, we’ve transitioned to video training and online competency tests. This award-winning program freed up precious time for our nurses and dietitians to focus on HCL onboarding. All the tools and how-to guides can be downloaded.
These combined efforts have effectively tripled our onboarding capacity, allowing us to grow from 3-5 individuals per month to 12-15.
Here are some pivotal questions to consider when creating capacity:
- How many people could two educators onboard onto HCL in just a week?
- Could some of the traditional DAFNE (or equivalent) sessions be replaced with HCL onboarding? While some may argue for the importance of education, isn’t it feasible to incorporate that education directly into HCL training, especially since HCL eliminates much of the need for extensive education on dose adjsutment?
- Is there a genuine need for specialised clinics focused on therapy adjustments, mealtime management, and detailed carbohydrate counting if HCL automatically handles many of these adjustments? Might these sessions be better utilised for HCL onboarding?
Many existing practices can be re-evaluated to prioritise HCL onboarding. It takes courage and honest reflection. As a dietitian with Type 1 diabetes, I’m a staunch advocate for education. While I’ve helped develop effective CGM programs, the outcomes from HCL far surpass those results. It’s not just about doing what we believe is effective; it’s about focusing on proven methods that offer the most significant impact. Furthermore, it’s best to package key lifestyle education as part of HCL onboarding, a BOGOF (Buy One Get One Free) approach.
Developing Pathways & Crafting Materials for HCL Onboarding
Both European and UK best practice guides offer detailed insights into safe and effective onboarding procedures. They’re crucial readings. However, they lack ready-to-use tools and resources. This might lead every service to “reinvent the wheel.”
To prevent countless hours of duplication, we offer valuable materials that could save you precious time. We’ve made them generic (minus logos and specific contact details) so you can use or adapt them (skin in the game style) to your local requirements. They are discussed briefly below. However, at the bottom of the page, there is a table with all the resources, the evidence base, and a link to download them. Enjoy!
Special note: Open the resources in Adobe Acrobat, not your web browser, as they have JavaScript code embedded.
Here’s a summary of what we’ve prepared (or you can send the people you support for a more in-depth AID guide):
- HCL System Selection: We’ve streamlined the process using a Google form detailing the pros and cons of each system, complete with key resource links. This lets users select a system and instantly notify you about their choice by completing the form. We discovered that 90% selected through this method, while the remaining 10% preferred a face-to-face consultation. This efficient method has spared hours of diabetes educator time. Check it out here, and feel free to replicate and customise it for your platform. Don’t know how to create a Google form?:
Which AID system is best? They are all Supercars! My choice is a Lamborghini, yours might be a Porsche, no bother, they are all amazing and will get fabulous results.

- Education Pathway and Resources:
- Session 1: Pre-pump/CGM education covering the essentials like highs, lows, and differences between injections and pumps.
- Session 2: onboarding onto the technology.
- Session 3: Review session emphasizing critical safety information – “Surviving”
- Session 4: Review session focusing on behavioral insights – “Thriving”
We believed that at least 70% of the users could self-educate session 1 using a Google form, aiming for a minimum score of 8/10 on the automated competency assessment. This assumption proved correct, saving significant time. Check out our pre-pump education forms for the 780G, Omnipod 5, and T-Slim X2 . The remaining 30% needed session 1 face-to-face, mainly due to educational and language barriers. Scotland is thinking much bigger (Go on, Fraser Gibb and team)! They have developed a national online pre-education module that the DTN and ACDC may replicate.
Our session 1 forms also collect current insulin doses, enabling our specialised starting dose calculator developed in collaboration with UCLH (thanks, Francesca and Becky). This ensures consistent dose calculations and seamless onboarding. Download the calculator if you like what you see in this video. The rules used and how they are adjusted can be found here.
We’ve successfully conducted Session 2 face-to-face with groups of 4-12. However, there’s potential to transition this to a virtual setting seamlessly. Sessions 3 and 4 are primarily held virtually, but we’ve adapted to in-person sessions when needed, such as when interpreters are involved or to address specific educational comprehension challenges.
- Teaching Workbook: This comprehensive guide covers all topics across the four sessions. Drawing from European and UK best practices, we ensured the content’s accuracy and clarity by reviewing it with manufacturers, diabetes patients, and medical professionals. Existing resources, like the Panther program and CARES methodology, further enriched the workbook. These workbooks serve as detailed, step-by-step guides, eliminating the need for manufacturer assistance during sessions.
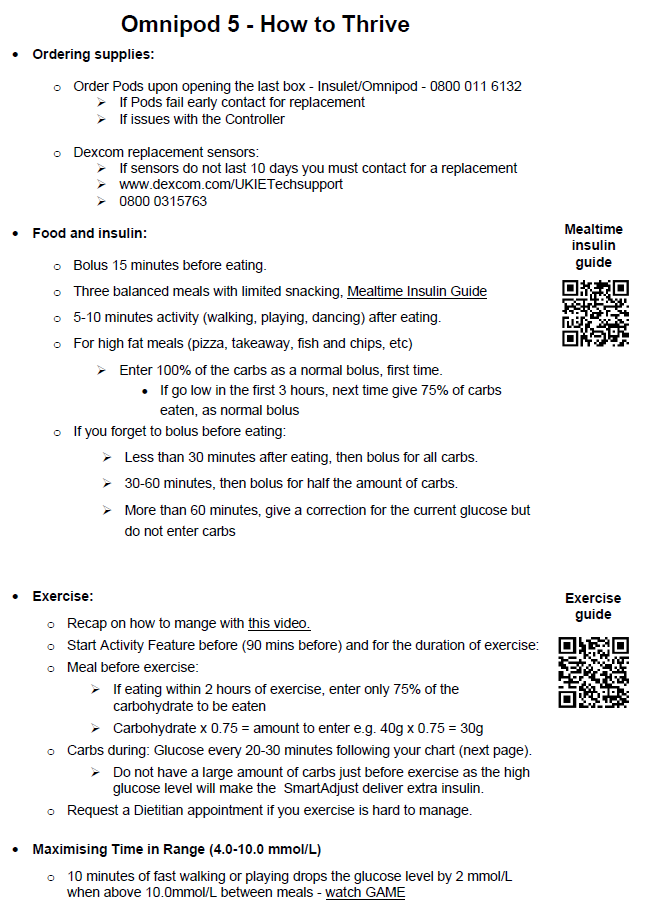
Interestingly, we found that after starting, most people with diabetes felt the bulk of the workbook was unnecessary. They wanted a concise summary spanning no more than two A4 pages, accompanied by QR-coded video links. It’s a perspective we hadn’t considered after dedicating two years to refining these workbooks. This underscores the crucial role of feedback from the most relevant audience. So, we distilled the essentials into a two-page “Survive and Thrive Guide” and gave QR code access to the full workbook. The Omnipod 5 Survive & Thrive is here.
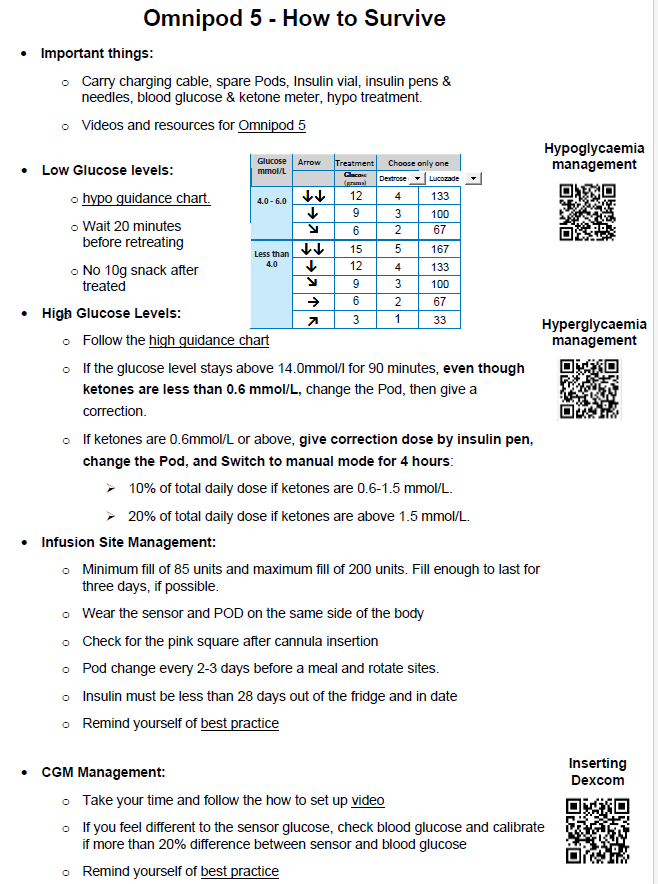
Find the Survive & Thrive guides for all four systems here:
We have also developed school careplans that save time teaching schools. All the how-to guides for implementing virtual school training by interactive PDF careplans can be downloaded. The HCL careplans can be found here:
- Review Process for Clinics: Every HCL system has unique settings. And while there isn’t an app (yet!) to simplify adjustments, we’ve developed a handy PDF tool. By entering details like daily insulin dosage, weight, and system type, the tool informs of which settings influence Automated mode and which need updating for Manual mode, whilst offering clinical and educational considerations. We’re actively using this in clinics, ensuring systems run seamlessly. The PDF also includes videos on how to use the tool and Survive & Thrive guides to assess 780G, T-Slim X2, and Omnipod 5 downloads. You can find the carb ratio, correction factor, and basal rate calculations used within the tool here,
By optimising our resources and leaning into efficient tools, we’ve streamlined the onboarding process. We invite you to benefit from our groundwork and further refine the journey for your patients.
Delivery & Evaluation
Based on our experience, there are some crucial requirements to enhance efficiency in your process:
- Administrative Excellence: Secure a diligent administrator who can manage the distribution and collection of Google/Teams forms. This ensures streamlined communication and organised feedback. Furthermore, this person must oversee “getting bums on seats” for the sessions. Pauline is our Trojan! Pauline tells me Accurx is THE best tool for fast and efficient communication.
- Project Management: Appoint a project manager responsible for overseeing the entire process. Accountability is key. Without it, achieving success becomes challenging. That’s my job!
- Adopt a Growth Mindset for Education: Dive into the educational sessions with a positive and resilient attitude. The provided workbooks are a safety net, ensuring you’re on the right track. Making mistakes or stumbling over words is natural, especially during the early stages. Remember, perfection isn’t the goal. Aim for safe and efficient onboarding. Start with sessions being “safe, though imperfect,” progress to “safe and decent,” then “safe and good,” and eventually achieve “safe and outstanding.” It’s meant to feel scary at the beginning; that’s what makes it exciting!
- Continuous Evaluation: Regularly audit your outcomes. This provides invaluable insights to share with your team, trust, and local ICBs. Our audit tool, complete with automatic calculations, is a handy resource, though you don’t need to get too detailed. As the saying goes, “what gets measured, gets managed.”
In conclusion, the path ahead is challenging, requiring a shift in the NHS mindset. Begin by embracing HCL as a united team and reflect honestly to create capacity. The materials provided here aim to guide the development of an effective pathway. Apply continual tinkering, ensuring you have skin in the game for successful local implementation. Conclude by sharing successes with both your immediate team and the broader community.
If you want more complete our AID Study Day (probably the best in the world).
If you found this guide valuable, please share it with others who might benefit, whether through email, social media, or other means.
Cheers
John Pemberton RD
Type 1 Diabetes Since 2008
Dad to Grace and Jude, whom The Glucose Never Lies is written for.
PS. Do you want to adapt the resources, Skin in the Game style, to local needs?
If so, purchase an Adobe Acrobat Pro license and see how easy it is to customise all the PDFs. Learn JavaScript coding and embed formulas if you want to get super fancy!.
Here are all the resources with the associated evidence-based base
| Resources | Description |
| Step-by-step teaching guides | The educational content was developed using methods outlined in the ATTD consensus on AID technologies (1) and the UK Diabetes Technology Network’s Best Practice Guidelines (2). These resources cover a range of topics including AID expectations, hypoglycaemia and hyperglycaemia management, infusion site care, nutrition advice, CGM management, and analysis of downloaded data. Exercise management advice was based on the ISPAD 2022 Exercise guidelines (3) and a detailed practical guide (4). The materials also encompass GAME-SET-MATCH strategies for optimising TIR (5–7) and a Mealtime Insulin Guide for T1D. To cater to different learning styles, we included manufacturers’ PowerPoint presentations, YouTube videos, and various explanatory tools. Additionally, we produced brief educational videos (5-10 minutes) to ensure clarity and consistency in messaging, which are accessible on www.screencast-o-matic.com at an annual cost of approximately £100. Each AID System (780G, CAMS, CIQ, and OP5) received a custom teaching guide, reviewed by the respective manufacturer’s education team. The Diabetes Team and CYP participating in the education sessions continually evaluated and enhanced these materials over a six-month period. Download links: 780G OP5 CIQ CAMS (Under construction) |
| Survive and Thrive guides | A crucial tool for CYP was the customised “Survive and Thrive” PDF guide, individually created for each AID system through JavaScript coding and Adobe Acrobat DC (annual cost of ~£180). This interactive guide generates a personalised hypoglycaemia treatment plan (5,6) and calculates carbohydrate needs for exercise based on the user’s name and weight, using ISPAD’s algorithms (3). It includes QR codes that link to essential short videos (5-10 minutes) covering key management techniques. The “Survive” section of the guide focuses on managing hypoglycaemia and hyperglycaemia, obtaining accurate CGM readings, infusion site management, and essential kit items to carry. The “Thrive” section details crucial nutritional and exercise management strategies, incorporating GAME-SET-MATCH approaches for optimising TIR (5,6) and a Mealtime Insulin Guide for Type 1 Diabetes (T1D). Each AID system, including 780G, CAMS, CIQ, and OP5, has a dedicated version of this guide, which has been reviewed by the education team of each system’s manufacturer. The Diabetes Team, along with the CYP participating in the education sessions, continuously reviewed and improved these materials over a period of six months. Download links: 780G OP5 CIQ CAMS |
| Interactive School Careplans | Similar to the “Survive and Thrive” guide, we transformed AID school care plans into interactive PDFs with embedded videos, requiring an 80% competency score for completion, thus reducing the need for direct teaching by healthcare professionals (8). Download links: 780G OP5 CIQ CAMS with Dana CAMS with Ypso |
| AID starting settings calculator | We adapted the Automated Insulin Delivery (AID) starting dose calculator originally created by the University College of London’s Diabetes Team. This calculator is grounded in the insulin setting guidelines proposed by the ISPAD 2022 guidelines (9) and incorporates research on paediatric bolus calculator settings (10). Our enhancements to the calculator were informed by the ATTD consensus recommendations, allowing it to produce tailored initial settings for various AID systems that support smooth onboarding. Download links: AID Starting Settings Calculator Algorithms behind the calculator |
| AID download assessment tool | This starting settings calculator led to the development of a download assessment clinical tool. We integrated the calculator’s algorithms with our understanding of factors influencing automated mode and manual mode adjustments in AID systems (1). This tool provides users with insights into which settings affect each mode of the AID system. It also offers tailored suggestions for optimising glucose control. These suggestions are based on several factors: current TIR, total daily insulin dose, desired percentage of basal insulin, and the specific AID system in use. The tool thus serves as an efficient guide for clinicians in supporting CYP make effective adjustments to their AID systems. Download links: Download Assessment PDF tool |
| Google Forms | We developed Google Forms for AID system selection and pre-initiation education, incorporating teaching guide materials, current insulin settings, setup guides, links to AID simulator applications, and an automated quiz with an 80% pass requirement for progression to onboarding. The forms also facilitated efficient organisation of onboarding sessions. Download links: AID System Selection Google Form Prototype, 780G Pre-AID Education Google Form Prototype OP5 Pre-AID Education Google Form Prototype CIQ Pre-AID Education Google Form Prototype CamAPS FX (under construction) |
References
1. Phillip M, Nimri R, Bergenstal RM, Barnard-Kelly K, Danne T, Hovorka R, et al. Consensus Recommendations for the Use of Automated Insulin Delivery (AID) Technologies in Clinical Practice. Endocr Rev. 2023 Sep 6;44(2):254–80.
2. Griffin TP, Gallen G, Hartnell S, Crabtree T, Holloway M, Gibb FW, et al. UK’s Association of British Clinical Diabetologist’s Diabetes Technology Network (ABCD-DTN): Best practice guide for hybrid closed-loop therapy. Diabet Med. 2023 Jul 1;40(7):e15078.
3. Adolfsson P, Taplin CE, Zaharieva DP, Pemberton J, Davis EA, Riddell MC, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Exercise in children and adolescents with diabetes. Pediatr Diabetes. 2022 Dec 1;23(8):1341–72.
4. Zaharieva DP, Morrison D, Paldus B, Lal RA, Buckingham BA, O’Neal DN. Practical Aspects and Exercise Safety Benefits of Automated Insulin Delivery Systems in Type 1 Diabetes. Diabetes Spectr. 2023 Mar 1;36(2):127–36.
5. Pemberton JS, Kershaw M, Dias R, Idkowiak J, Mohamed Z, Saraff V, et al. DYNAMIC: Dynamic glucose management strategies delivered through a structured education program improves time in range in a socioeconomically deprived cohort of children and young people with type 1 diabetes with a history of hypoglycemia. Pediatr Diabetes. 2021 Nov 17;22(2):249–60.
6. Pemberton JS, Barrett TG, Dias RP, Kershaw M, Krone R, Uday S. An effective and cost-saving structured education program teaching dynamic glucose management strategies to a socio-economically deprived cohort with type 1 diabetes in a VIRTUAL setting. Pediatr Diabetes. 2022 Jun 11;23(7):1045–56.
7. Pemberton JS, Gupta A, Lau GM, Dickinson I, Iyer PV, Uday S. Integrating Physical Activity Strategies to Lower Hyperglycaemia in Structured Education Programmes for Children and Young People with Type 1 Diabetes Improves Glycaemic Control without Augmenting the Risk of Hypoglycaemia. Smart CE, editor. Pediatr Diabetes. 2023 Jul 5;2023:1–8.
8. Pemberton JS, Collins L, Sands D. Oral Abstract 67: Virtual schools training package teaches 37% more staff and reduces the cost by 83% compared to face-to-face training during the COVID-19 pandemic. Pediatr Diabetes. 2022 Oct 1;23:3–43.
9. Sherr JL, Schoelwer M, Dos Santos TJ, Reddy L, Biester T, Galderisi A, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Diabetes technologies: Insulin delivery. Pediatr Diabetes. 2022 Dec 1;23(8):1406–31.
10. Hanas R, Adolfsson P. Bolus Calculator Settings in Well-Controlled Prepubertal Children Using Insulin Pumps Are Characterized by Low Insulin to Carbohydrate Ratios and Short Duration of Insulin Action Time. J Diabetes Sci Technol. 2017 Mar 1;11(2):247.
Click here to subscribe.