Mealtime Insulin Guide, Part 1 of 3
High-Carb Meals: Smashing the Spike
The bowl of cereal hits the table at seven, the school run is at eight, and the CGM trace from the last few mornings tells the same story: a fast climb past nine, a peak somewhere in the elevens, and a slow walk back down by mid-morning. The food finished digesting twenty minutes ago. The insulin is still arriving. This page is the part of the guide that names that gap, the mechanism behind it, and the moves that close it most reliably.
Ask Grace
Want to ask which pre-bolus window suits your insulin, or how a post-meal walk lands in your CGM trace? Ask Grace.
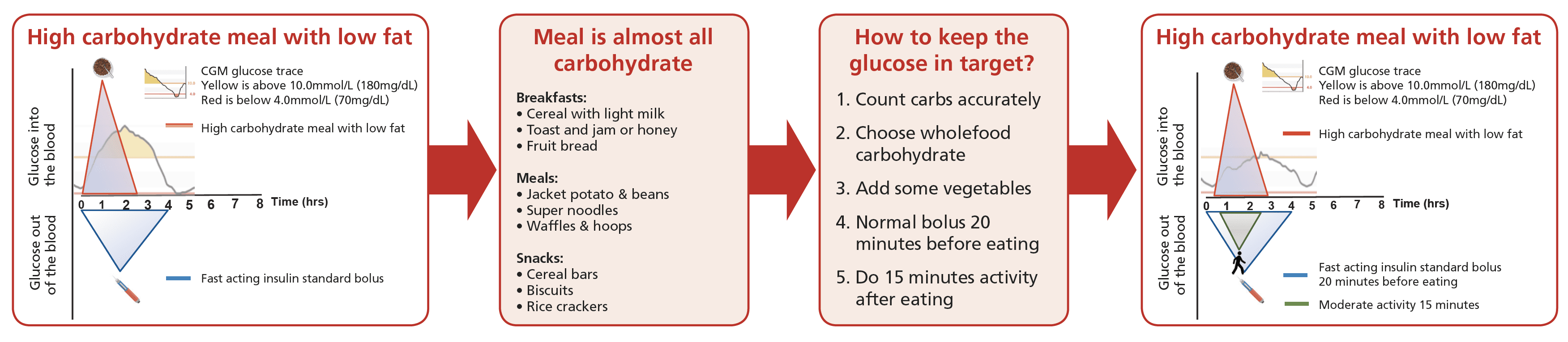
What kind of meal lands in this part of the guide
The breakfast cereal bowl is the textbook example. The jacket potato with baked beans, the toast and jam, the waffles with spaghetti hoops. As snacks: the cereal bar, the rice cracker, the biscuit at eleven. These are the meals where carbohydrate enters the bloodstream fast because digestion is fast, and the spike that follows is not a calculation error so much as the predictable result of giving carbohydrate a head start on injected insulin.
This page is not a defence of building a daily diet around these meals. The Mealtime Insulin hub names the mixed-meal pattern the carb ratio was tuned for, and most weeks should look like that. This page is for the mornings when high-carb is what is in front of you, and the trace from the previous high-carb morning is the reason you are reading.
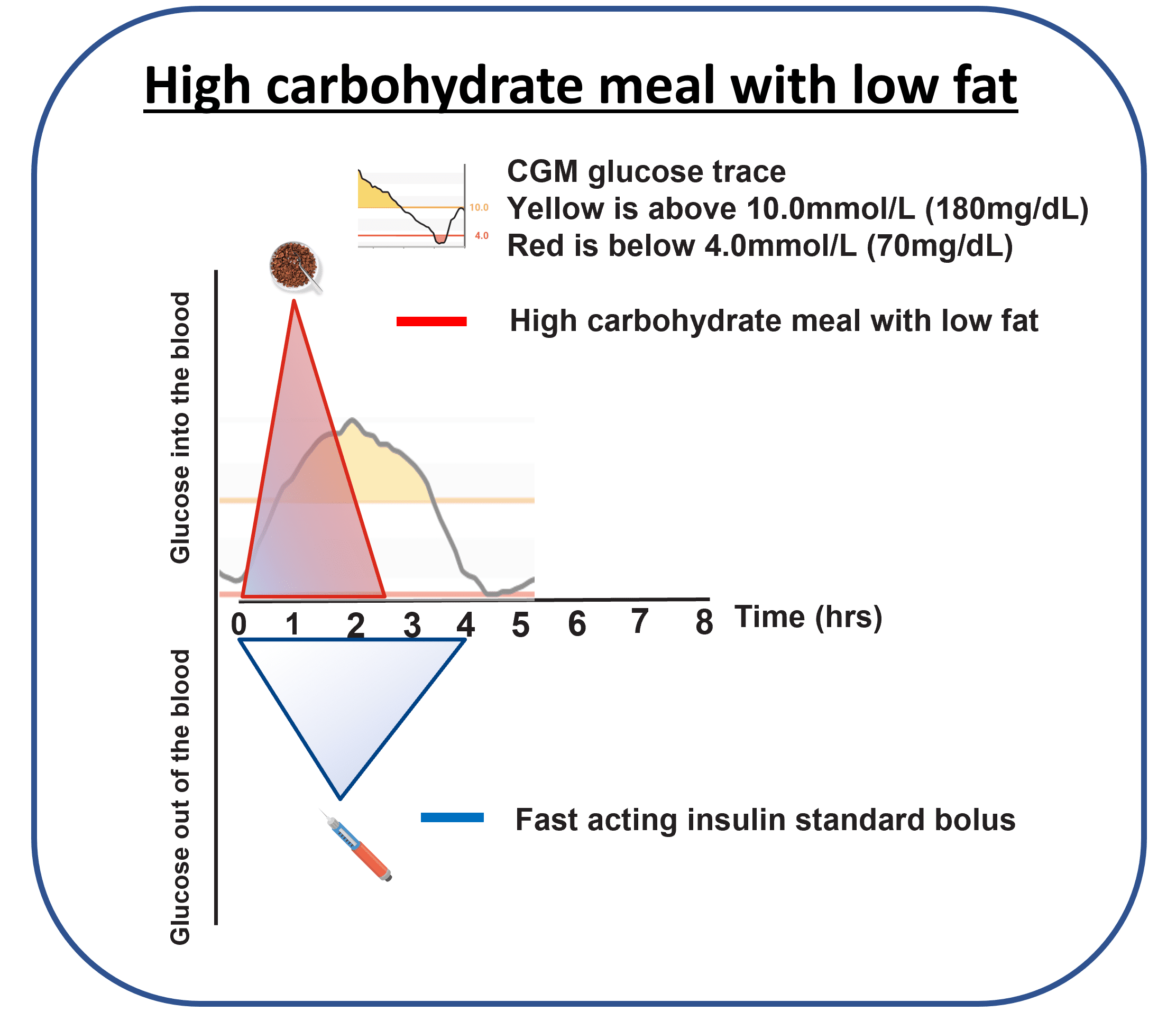
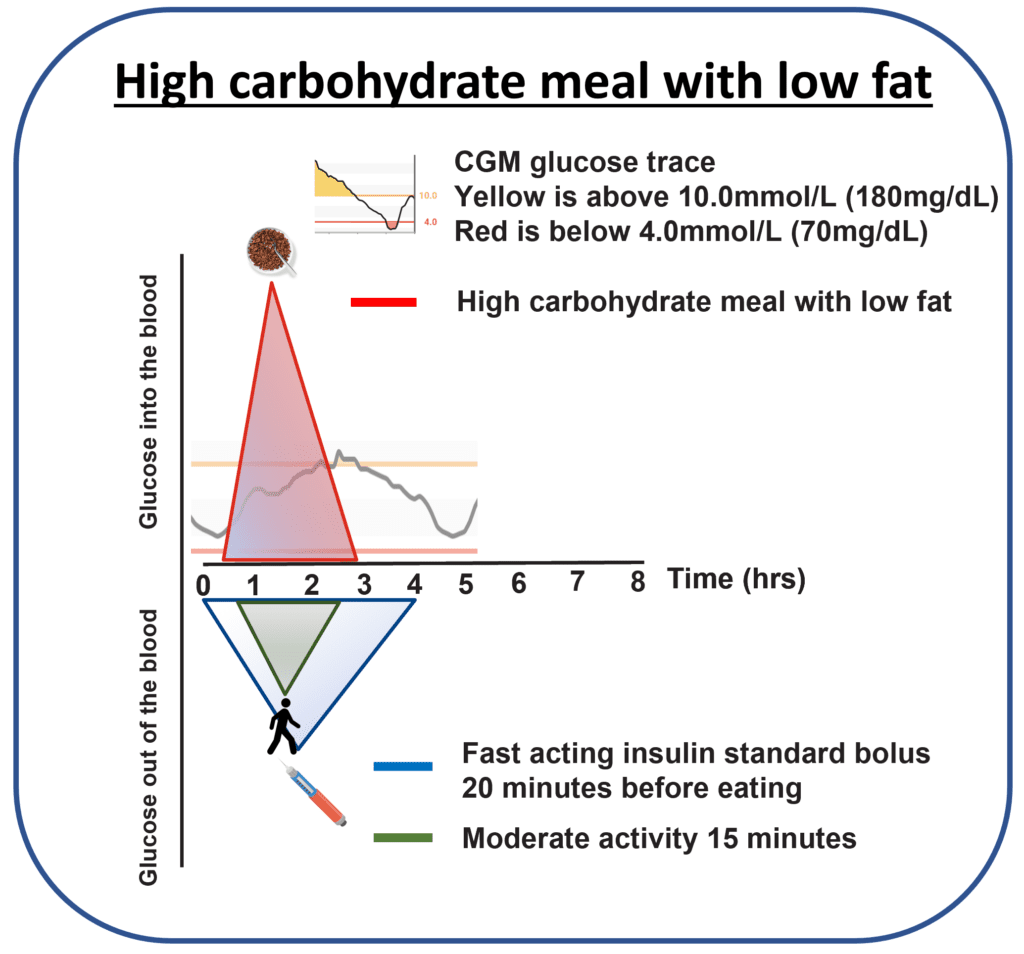
What the trace looks like
Carbohydrate arrives in the bloodstream within minutes. Injected or pumped insulin takes tens of minutes to start, longer to peak. The CGM line climbs while the insulin is still on its way; by the time the insulin is doing real work, the food is mostly absorbed.
Why the spike happens
Two structural mechanisms explain why injected insulin cannot quite catch fast carbohydrate. The first sits in anatomy; the second sits in pharmacokinetics. Neither is fixable with willpower; both are workable with timing.
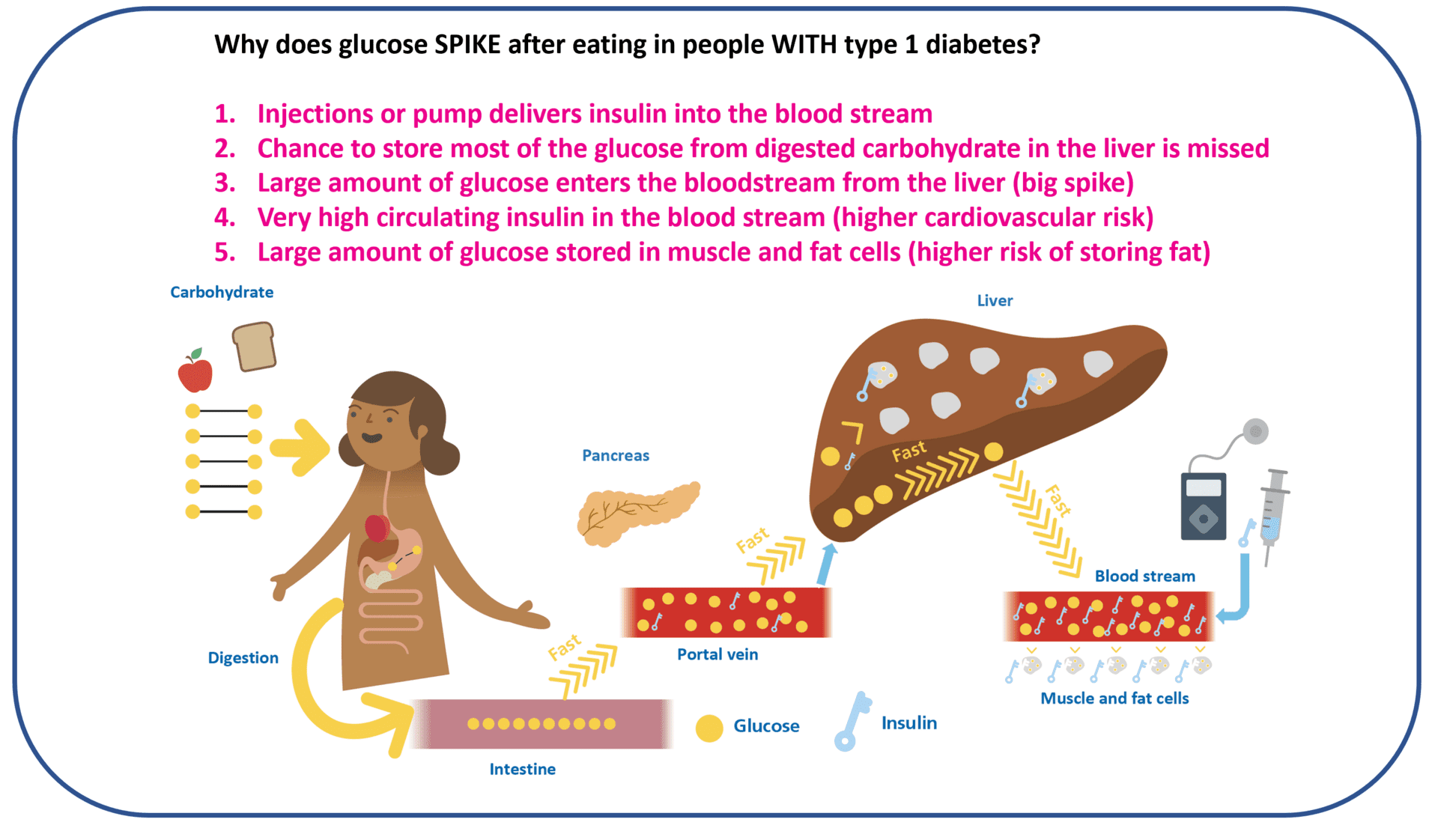
The portal vein signal that is not there
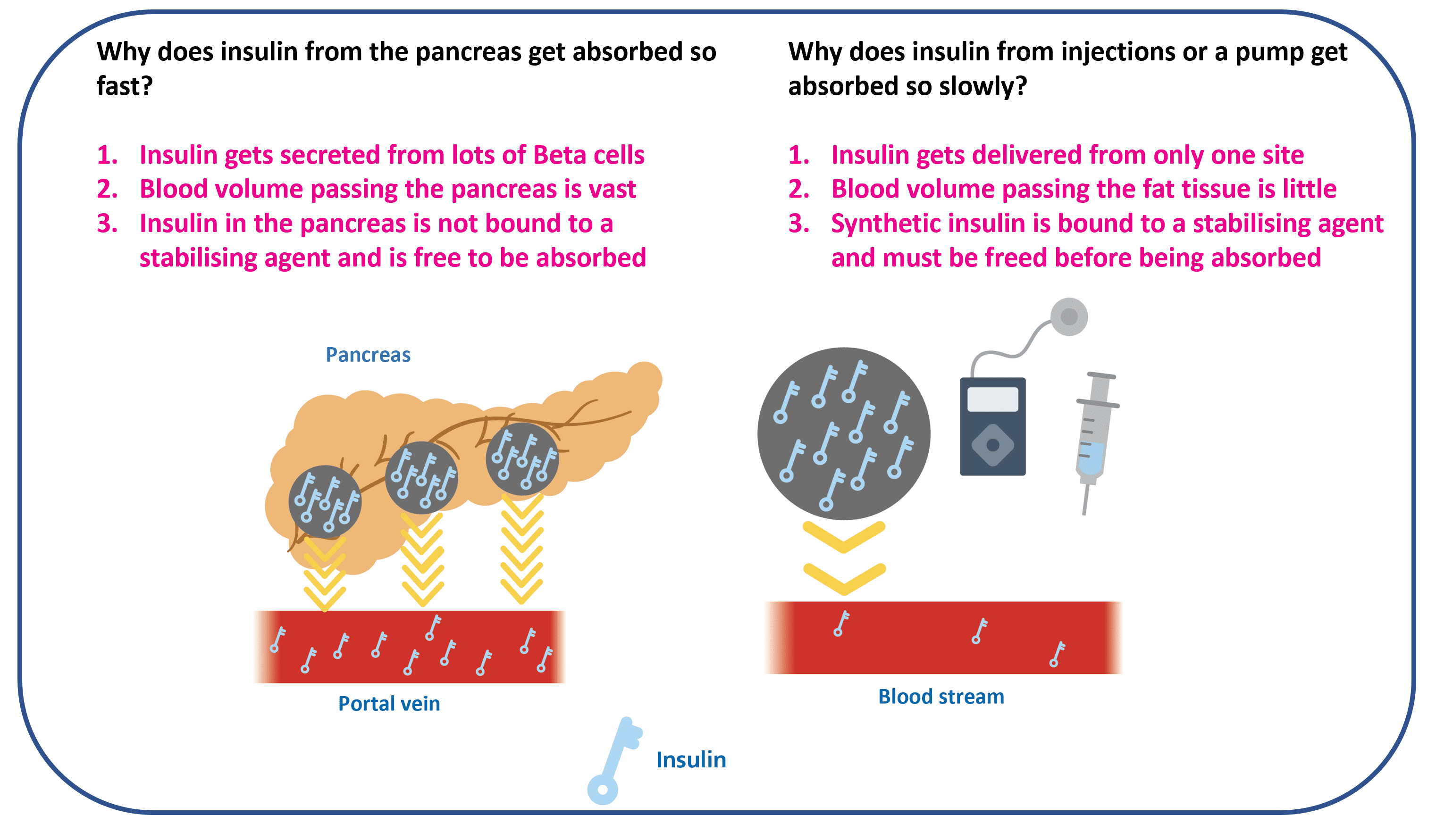
In people without diabetes, insulin secreted from the pancreas reaches the liver first via the portal vein. That early, concentrated liver dose suppresses hepatic glucose output the moment carbohydrate starts arriving. With injected or pumped insulin, that route is bypassed. The insulin takes the long way round, reaches the liver later and at lower concentration, and the early liver brake is largely missing.
Slow absorption from the depot
Whether injected with a pen or delivered subcutaneously by a pump, insulin has to dissociate from its hexamer state, diffuse through the tissue, and reach the bloodstream. That takes time. On a standard rapid analogue (Humalog, NovoRapid, Apidra), the pharmacokinetic peak lands somewhere around 60 to 90 minutes after the dose; on the ultra-rapid analogues (Lyumjev, Fiasp), the peak is faster but still delayed compared with native pancreatic secretion. High-carb meals often finish digesting before insulin has fully arrived (Leohr 2021, Clinical Pharmacokinetics).
The moves that close the gap
Two categories of move, both useful, one structurally more powerful than the other. Food-based moves slow how fast the glucose arrives. Timing-based moves change when the insulin is already working. The structural advantage of the timing moves is that they address the actual problem.
Slow the rise from the food side
Choose mainly low-glycaemic-index carbohydrates
Slower-digesting carbs (oats, lentils, wholegrain bread, basmati rice) raise glucose more gradually, which gives the insulin time to catch up. The same carb count, slower delivery, smaller spike.
Add vegetables, then add fat, then add protein, in that order on the plate
Eating the protein and vegetables first slows gastric emptying and reduces the size of the post-meal peak. Adding fat keeps the meal in the stomach longer for the same effect. Vinegar (a teaspoon or two) has a similar effect through delayed gastric emptying. None of these are a substitute for timing the dose, but they stack with it.
Close the timing gap from the insulin side
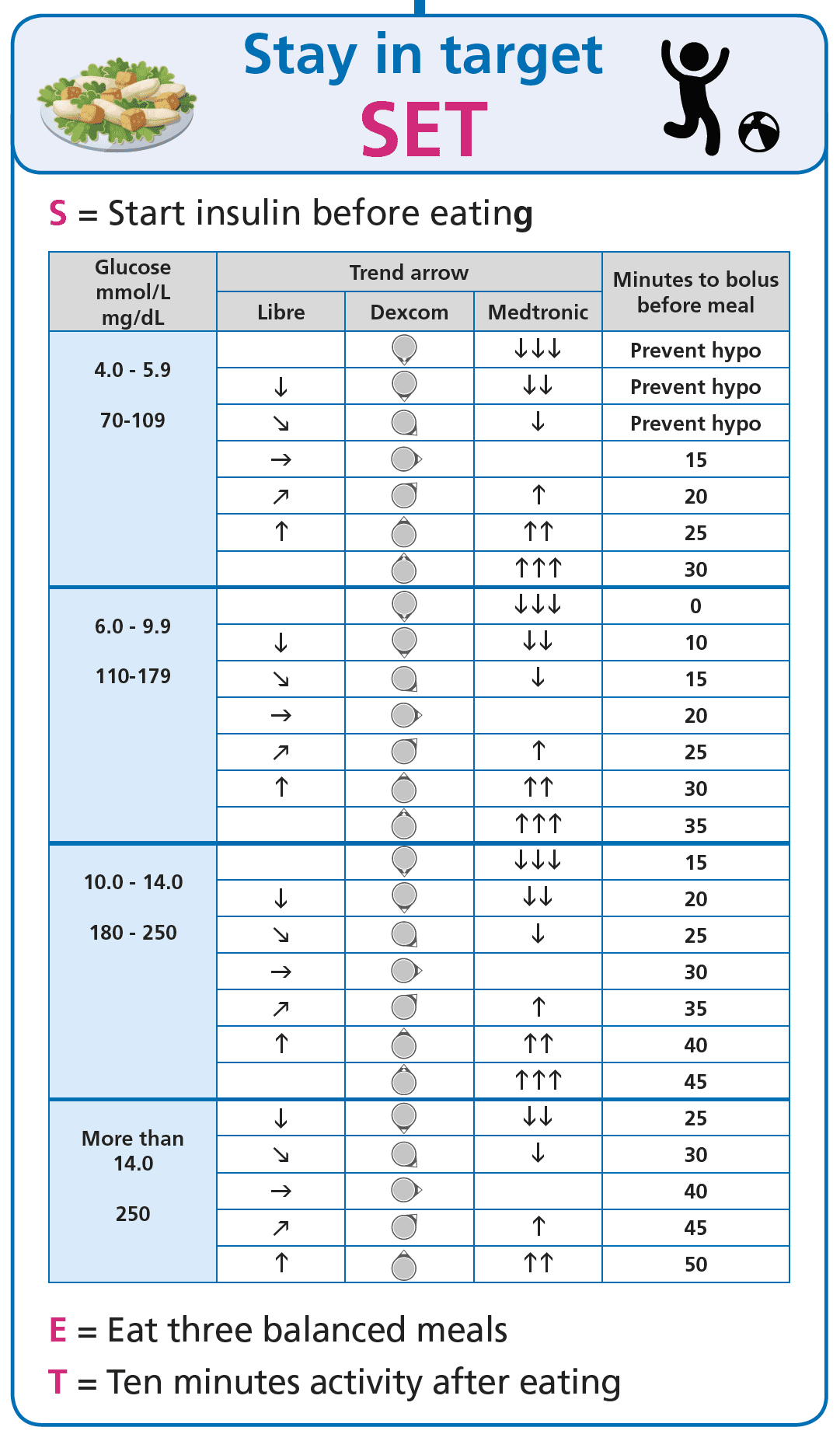
Pre-bolus, the cheapest single move
Bolusing around 20 minutes before the first bite of a usual mixed meal, on a standard rapid analogue, is the dose-timing change that most consistently lowers the post-meal spike (Slattery 2018, Diabetic Medicine). On the ultra-rapid analogues (Lyumjev, Fiasp), the window is shorter, sometimes none. If the starting glucose is low, the window shrinks; if the starting glucose is high, it lengthens. This is the S of the GNL SET framework.
Move for 10 to 15 minutes after eating
A short walk, some pottering, light housework, the school-run pavement; muscle uptake of glucose increases sharply with even gentle movement, and the size of the post-meal peak comes down. This is the T of the SET framework. Of all the strategies on this page, this is the one with the lowest cost and the most reliable effect.
The strategy in one picture
For the people who learn best from a single image rather than a page of prose, the same content as the disclosures, condensed.
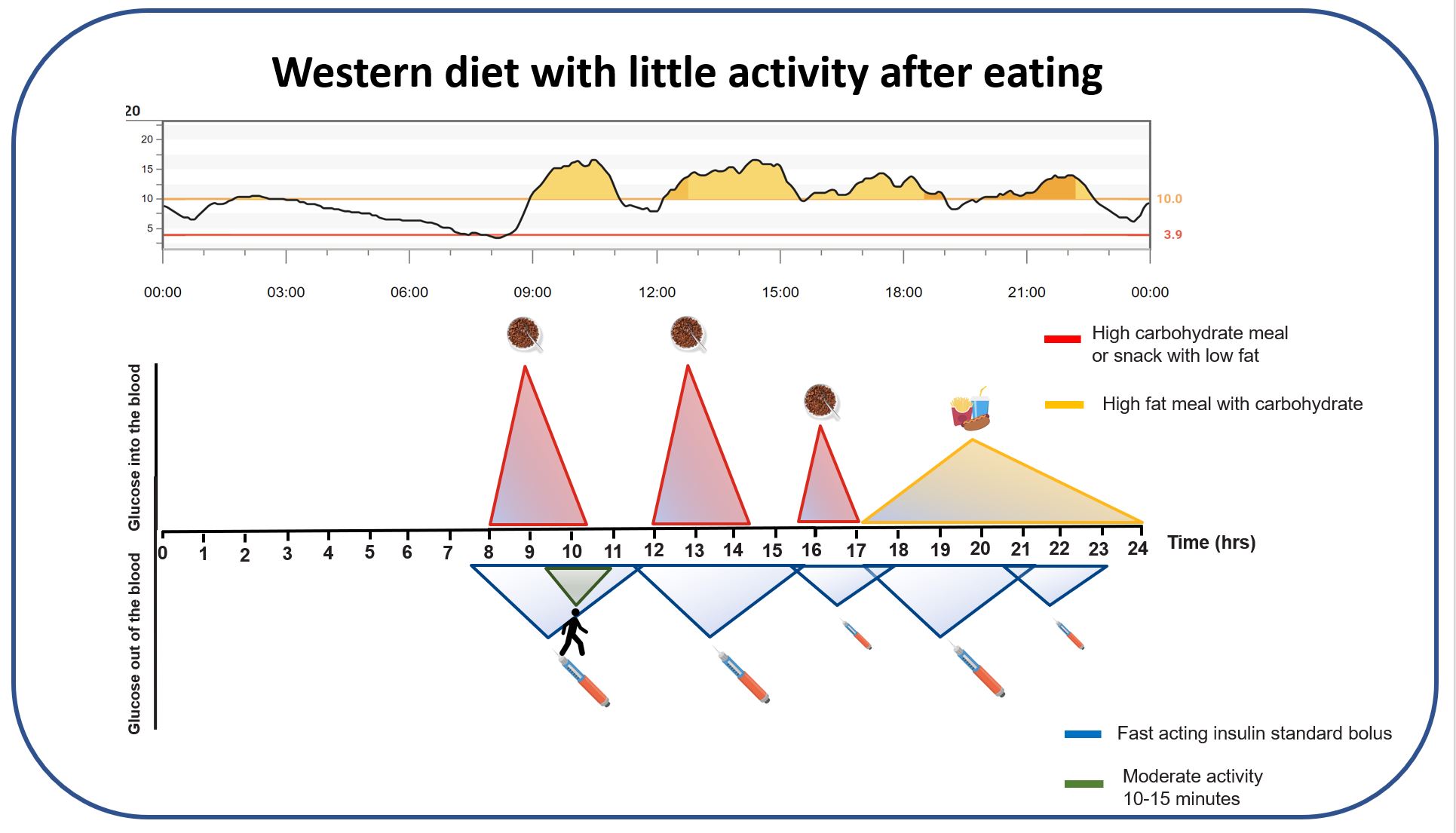
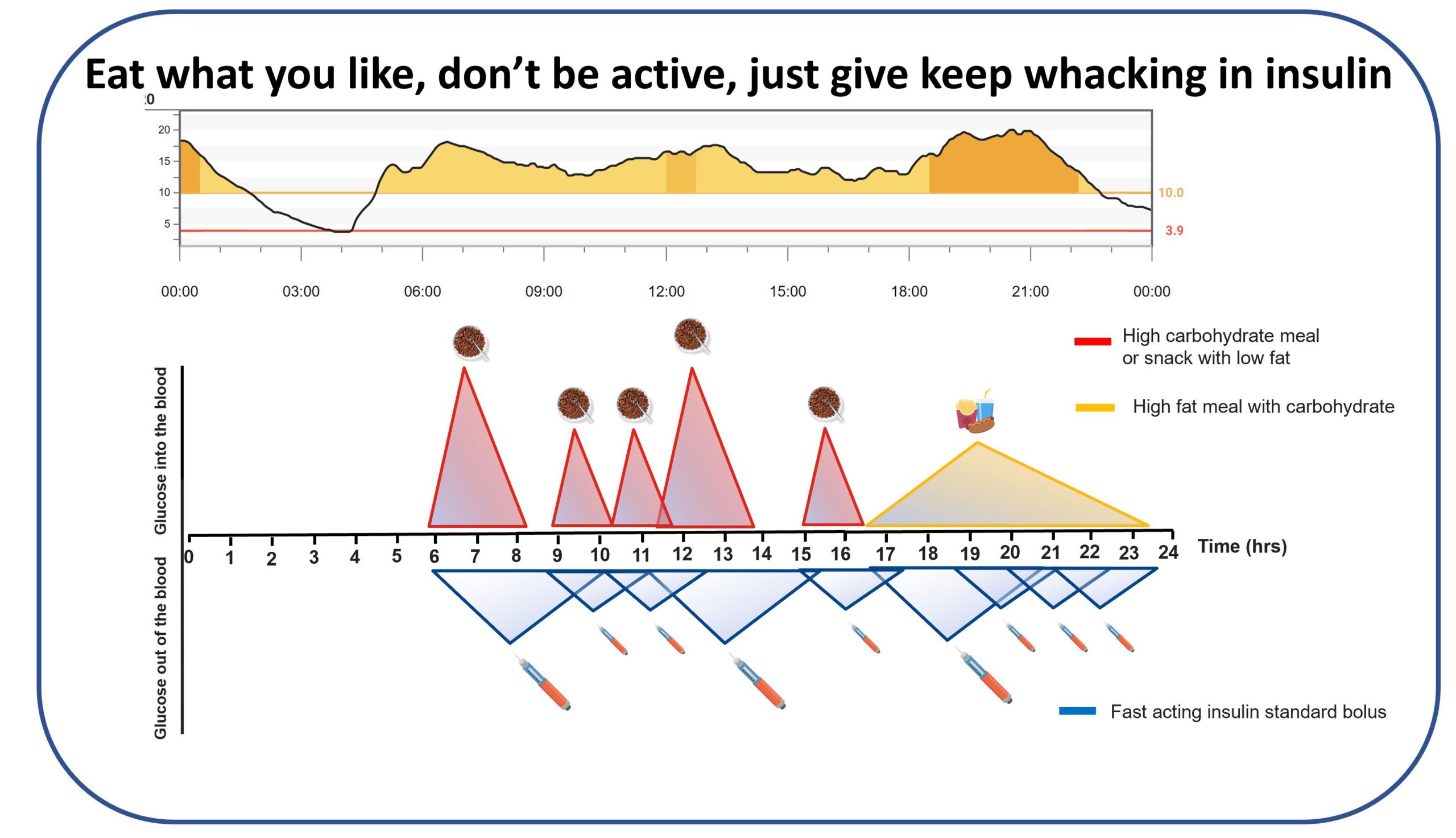
The pattern that creeps in if this becomes the daily default
If high-carb processed eating becomes the daily baseline, the structural arithmetic shifts in a direction that is hard to win. Insulin demand rises, the magnitude of the daily corrections rises with it, the peripheral insulin levels run higher more of the time (which is not how the body is designed to operate), and many people find themselves living in correction-and-hypo territory most days.
The high-carb meal is a timing problem, not a willpower problem. Carbohydrate enters the bloodstream faster than injected insulin can act. Pre-bolus and post-meal movement are the two structural moves that close that gap most reliably; food sequencing, low-GI choices, and added fat or vinegar slow the rise from the other side and stack on top. None of this turns high-carb meals into low-carb meals; it turns the spike into something the dose can keep up with.
This content is for educational exploration only. It describes population-average responses and general principles. The 20-minute pre-bolus window is a starting point on rapid analogues; on ultra-rapid analogues it is shorter or none. Refine with CGM and your diabetes care team.
Trying it on a meal you already eat
The cheapest experiment is the one you can repeat. Pick a high-carb meal you already eat regularly (the breakfast bowl, the Saturday toast, the school-night pasta with sauce). Run it twice over the next two weeks. The first time, do nothing different and watch the trace. The second time, pre-bolus 20 minutes ahead and walk for 10 to 15 minutes after, and watch the trace again. The CGM is the entry criterion and the answer; the glucose never lies. Bring both traces to your diabetes care team if the second one still climbs above target; the conversation is then evidence-anchored on both sides.
References
Slattery 2018, optimal prandial bolus timing review
Slattery D, Choudhary P. Clinical use of continuous glucose monitoring in adults with type 1 diabetes, optimal prandial bolus timing. Diabetic Medicine. 2018. The clinical literature anchor for the 20-minute pre-bolus on rapid analogues for usual mixed meals.
Leohr 2021, ultra-rapid lispro pooled PK/PD analysis
Leohr J, et al. Pharmacokinetics and glucodynamics of ultra-rapid lispro versus lispro across a clinically relevant range of subcutaneous doses. Clinical Pharmacokinetics. 2021. N=190 clamp-study analysis. Shapes the shorter pre-bolus window on Lyumjev and Fiasp.
Pemberton 2021, Mealtime Insulin Guide (the wider matrix this part sits inside)
Pemberton J, et al. The Glucose Never Lies Mealtime Insulin Guide for type 1 diabetes. Pediatric Diabetes. 2021. COI flag: John Pemberton is lead author. Anchors the dosing matrix on the Mealtime Insulin hub; carb-only meals undershoot the mixed-meal ratio by roughly 30 percent.
Part 1 of 3
High-Carb Meals: Smashing the Spike