
What gets measured gets manged!
There are so many things you can measure to see how things are going. It’s easy to get overwhelmed because:
What gets measured gets managed
It’s easy to burn out following ten different things!
I will keep it super simple.
Let’s focus on the three most important measures.
- Percentage time in range (4.0-10.0mmol/L or 70-180mg/dL)
- HbA1c (mmol/mol or %)
- Total daily insulin dose (units per kilogram, u/kg)
Time in range (4.0-10.0mmol/L or 70-180mg/dL)
You are familiar with time in different glucose ranges, I have been banging on about them from the start. Here is a graphic from the latest international consensus statement of where to aim for. There is a lot more on the For John – Research page.
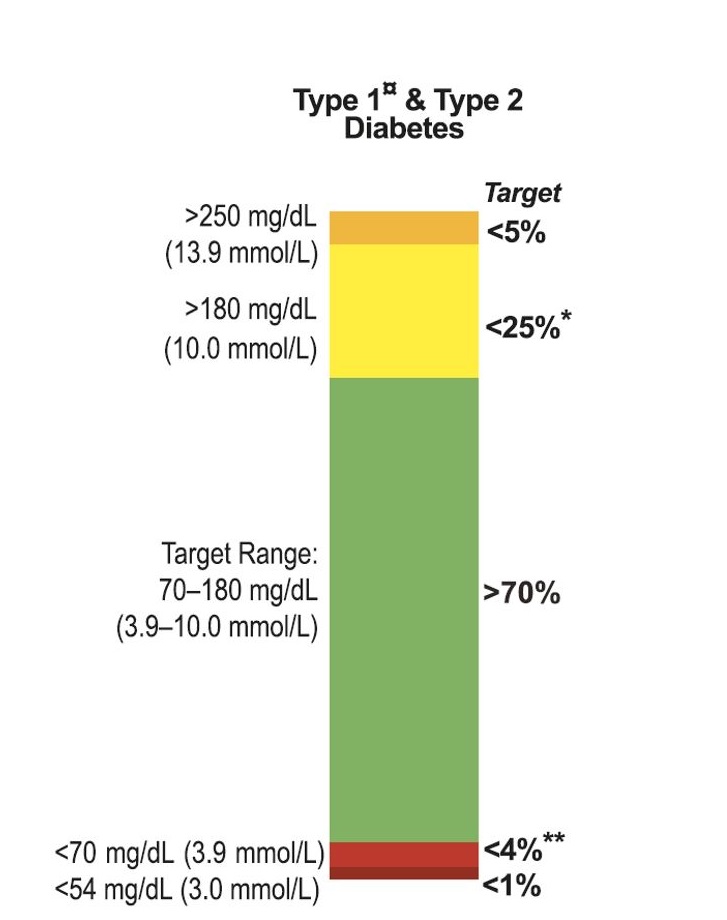
I think 70% time in range is a good place to start. However, by following Dynamic Glucose Management, 70% is the basement.
We are going up to the penthouse.
I created this table that allows you to choose what time in range you would like.
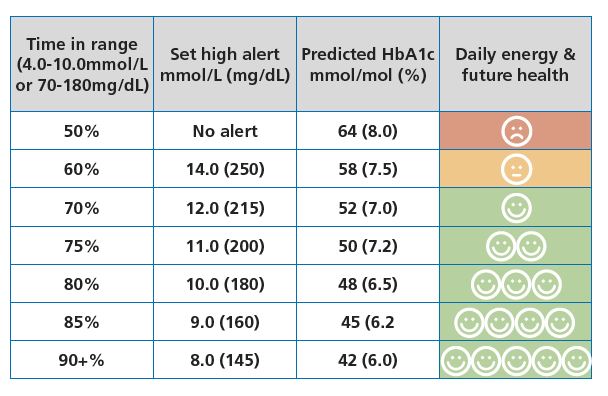
The catch is that you must set the high alarm accordingly and use the GAME part of Dynamic Glucose Management to achieve it.
Don’t start too fast.
Rome was not built in a day. Take baby steps like I did, and improve 5% every two weeks or so.
HbA1c (mmol/mol or %)
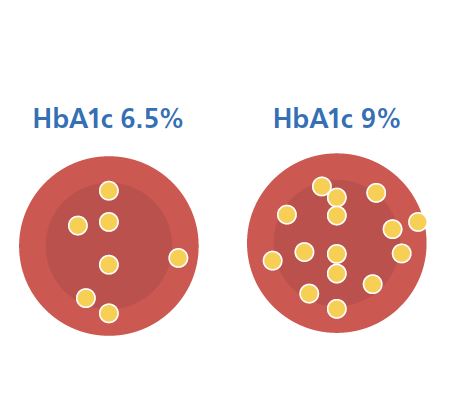
This picture explains HbA1c measures how much glucose is stuck to your red blood cells. The more glucose stuck, the higher the blood glucose has been for the last three months.
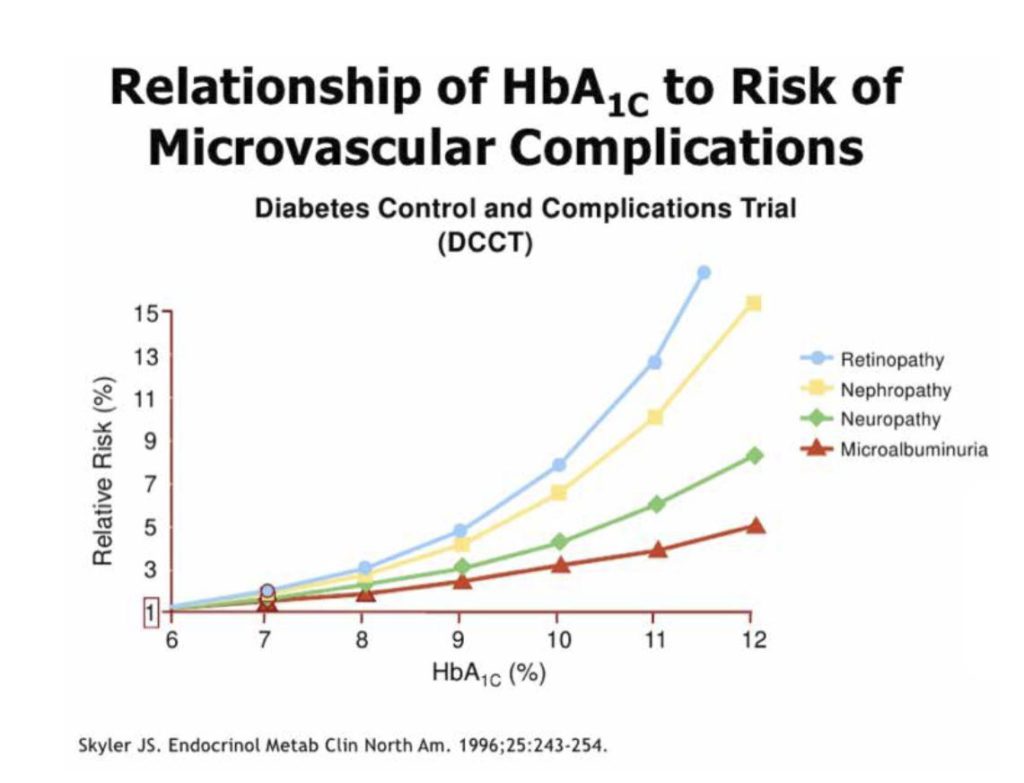
The HbA1c measurement is like a crystal ball. It allows you to see how healthy you will be on the future.
This is a famous graph from the biggest trial ever done on people with type 1 diabetes.
It shows the risk of nasty small blood vessel complications goes up as HbA1c increases.
Aim to keep HbA1c at or below 48mmol/mol (6.5%). If you keep time in range above 80%, this is almost guaranteed.
Total daily insulin dose
The average insulin dose for adults with T1D ranges from 0.4 to 1.0 units per kilogram (U/kg), but in some cases, it can be as high as 2.0 U/kg.
For example:
A 75 kg male typically requires 30–75 units of insulin, but this can go up to 150 units at the higher end. A 60 kg female typically requires 24–60 units, with a possible upper range of 120 units. Therefore;
- 0.4–0.5 U/kg → Insulin sensitive. About 10% of people with T1D
- 0.5–0.7 U/kg → Insulin resistance. About 30% of people with T1D
- 0.7–1.0 U/kg → Significant insulin resistance. About 50% of people with T1D
- More than 1.0 U/kg → High insulin resistance. About 10% of people living with T1D
For children aged 1–12, the same dose range as adults applies (0.4–1.0 U/kg).
However, from ages 12–18, due to hormonal changes, insulin needs increase slightly:
- 0.4–0.6 U/kg → Insulin sensitive. About 10% of people with T1D
- 0.6–0.8 U/kg → Insulin resistance begins. About 30% of people with T1D
- 0.8–1.2 U/kg → Significant insulin resistance. About 50% of people with T1D
- 1.2 U/kg → High insulin resistance. About 10% of people living with T1D
If you have just read that and thought OMFG!
“I have insulin resistance and need to get to 0.4 units per kg immediately!”
Relax! You are no different from 90% of people living with T1D.
Using 0.4 units per kilogram of insulin is just like trying to achieve 90%+ time in range (3.9-10.0 mmol/L or 70-180 mg/dL). It’s an aspirational goal. However, it’s important to balance what it takes to get there with where you’re starting from.
- If you’re currently using >1.0 units/kg, that’s similar to having a 40% time in range. Improving from 40% to 50% is significant, just as reducing insulin from >1.0 units/kg to below 1.0 is meaningful.
- If you’re at 0.7 units/kg, that’s like a 60% time in range, and moving to 0.6 units/kg (~70% time in range) is a major improvement.
Run your race, one that’s possible for you to win!
Essential point: Don’t sacrifice glucose control just to reduce insulin use. Lowering insulin at the expense of higher glucose levels is not a worthwhile tradeoff. The benefits of improved insulin sensitivity only matter if you maintain or enhance your current glucose control. Don’t rob Peter to pay Paul!
Read this guide to help you get on top of insulin resistance.
CONGRATULATIONS, you have laid strong foundations.
You are now ready for the game changer.
Next step: Dynamic Glucose Management