
Let’s talk hypos.
Let’s recap: what is a hypo?
Technically, it’s a glucose level less than 3.3mmol/L (60mg/dL). Remember, people without diabetes walk around with glucose levels 3.3-6.7mmol/L (60-120mg/dL) all day, every day. This is the optimal glucose range for health.
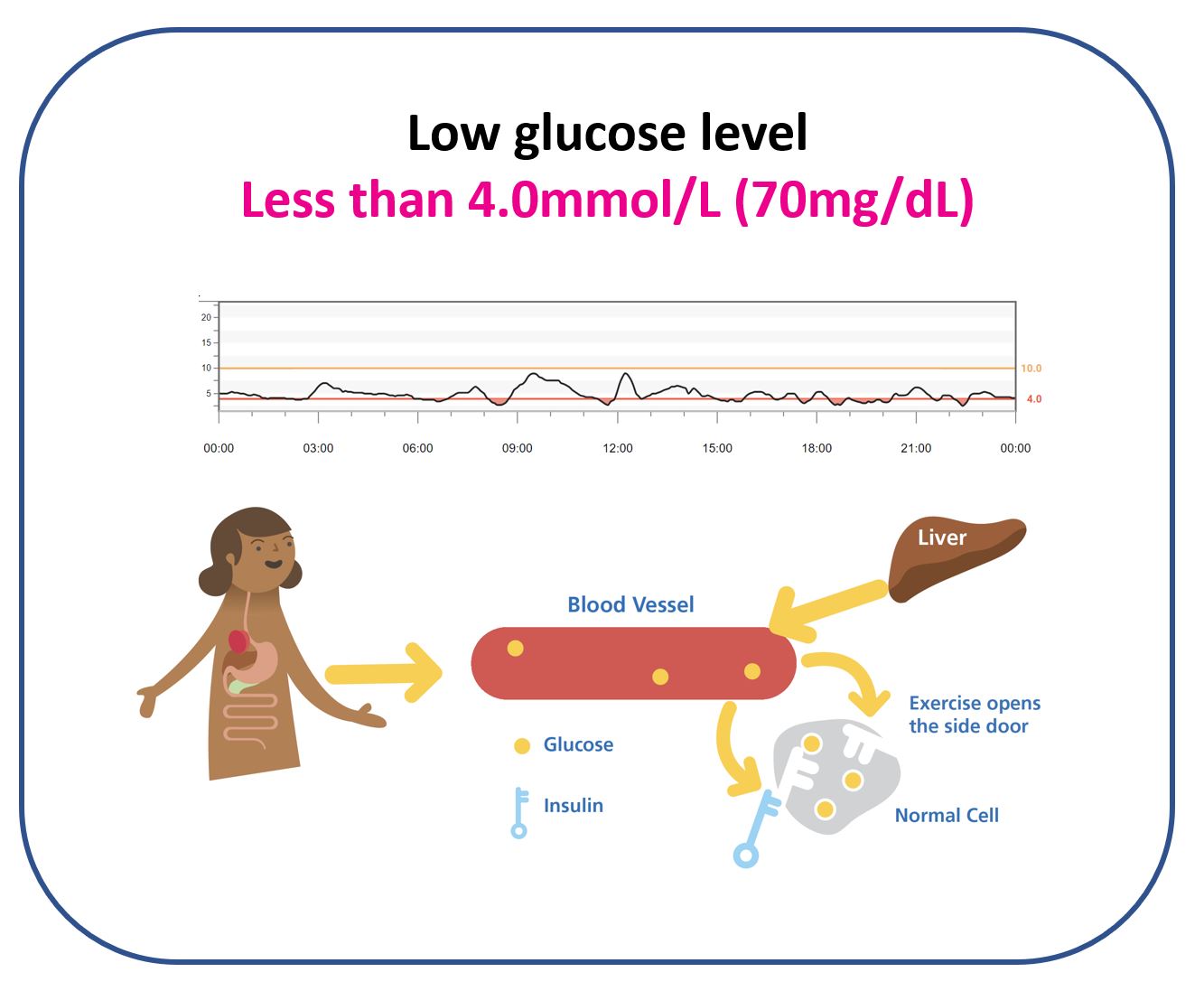
So why am I saying less than 4.0mmol/L (70mg/dL)?
Great question.
If you cast your mind back to the CGM discussion, we talked about the accuracy of CGM devices in the less than 4.0mmol/L (70mg/dL) range. One of the tables showed more than 90% of the Libre 2 and Dexcom G6 readings are deemed accurate in this range.
This sounds amazing, but let’s dig deeper.
How is accuracy defined?
In accuracy studies, a CGM reading is deemed accurate in the less than 4.0mmol/L (70mg/dL) range if it’s within 0.8mmol/L (15mg/dL) of the true blood glucose reading (measured by Yellow Spring Instrument for the John Pemberton’s out there).
This means more than 90% of the Libre 2 and Dexcom G6 readings in the less than 4.0mmol/L (70mg/dL) range are within 0.8mmol/L (15mg/dL) of the true blood glucose value.
Therefore, using 4.0mmol/L (70mg/dL) as the cut-off point to treat hypos will prevent almost all true blood glucose levels of less than 3.3mmol/L.
How so?
If the true blood glucose value is 3.2mmol/L (58mg/dL), then more than 90% of the time, the CGM will not be no more than 0.8mmol/L (15mg/dL) higher.
Viola, no higher than 4.0mmol/L (70mg/dL).
Therefore, setting the low alert at 4.0mmol/L (70mg/dL) makes sense.
If the low alert is set at 3.3mmol/L (60mg/dL), the true blood glucose can be down at 2.6mmol/L (47mg/dL), and no low alert will sound. In my opinion, this is a dangerous game to play.
Grace and Jude, we will set your low alert at 4.0mmol/L (70mg/dL) – safety first!
What should I treat a hypo with?
You may have been told:
15g of sugar to treat a hypo
If so, please erase this from your memory. Replace it with:
Treat hypos with glucose only, based on your body weight in kilograms (kg)
Why?
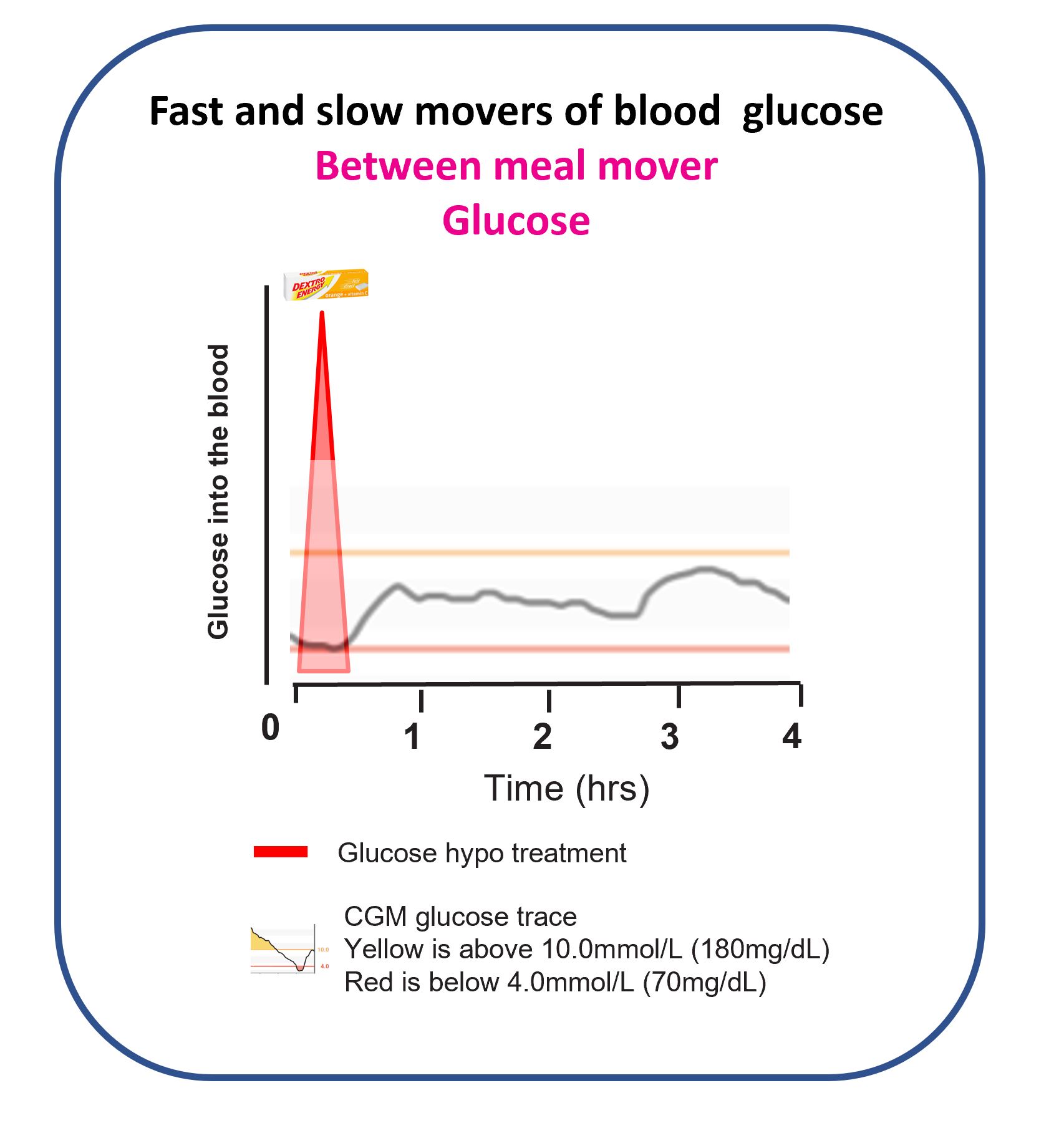
Let’s get back in the FAST lane.
This picture shows that a pure glucose hypo treatment works in ten minutes and has finished increasing the blood glucose level by twenty minutes. You can decide if another treatment is needed after twenty minutes, not before.
Why does my body weight matter?
The heavier you are, the greater the blood volume you have, and the more muscle and fat cells you have that can suck glucose out of the blood. Especially if you are hypo because of too much bolus insulin in the blood or you have exercised heavily.
This chart tells you how much hypo treatment you need based on weight. Grace, you currently weigh 20kg, so 6g of glucose is two dextrose tablets. I know you love them as you keep eating mine!
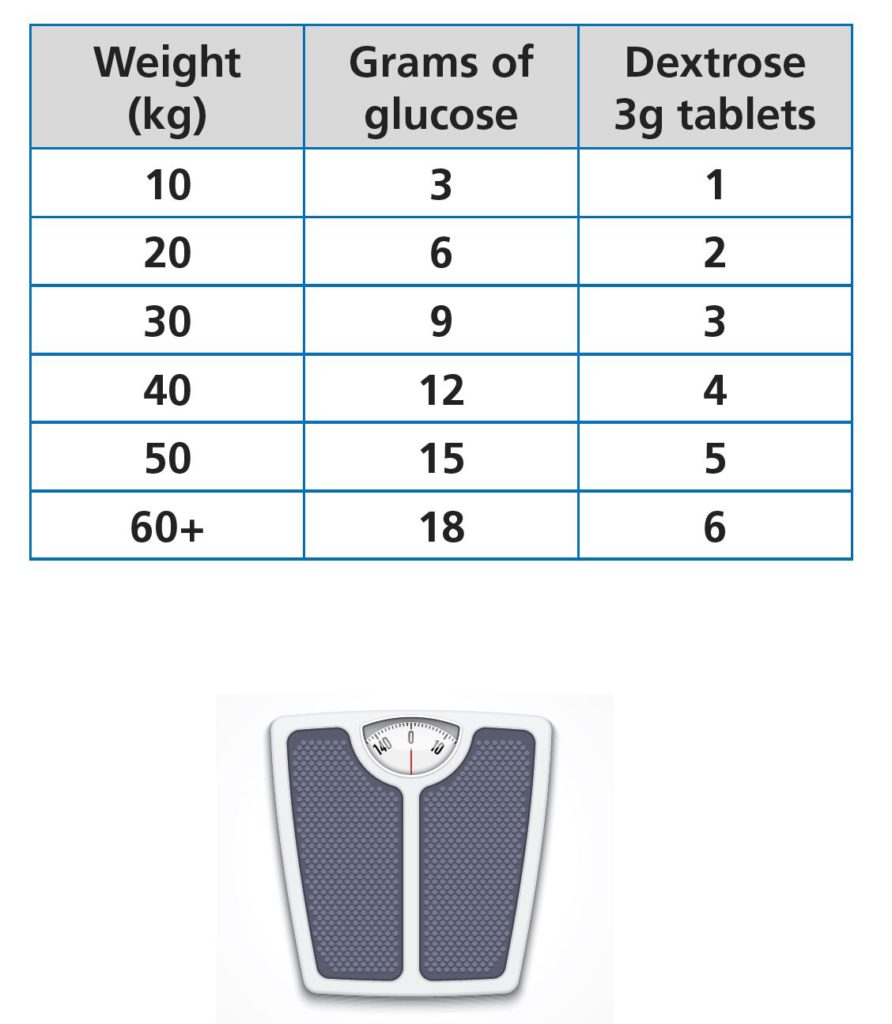
Why does the chart stop at 60kg?
The intestines’ maximum absorption of glucose is 1g per minute. Therefore, it makes no sense to treat with more than 20g of glucose when you are re-checking in twenty minutes. If you need a second treatment, it will be evident after 20 minutes.
By capping the hypo treatment at 18g and rechecking in twenty minutes, you will never stack glucose in the intestine. Stacking glucose can shoot the glucose high later, and you risk the unabsorbed glucose coming out the other end!
Why is the maximum on the chart 18g and not 20g, then? Very astute. There needs to be room for a slight just in case the arrows are double down!
Why does the table only have glucose tablets?
This is something I am passionate about. Using glucose tablets keeps things simple and prevents mistakes. It’s time for a set of bullet points to explain.
- Glucose tablets are easy to carry, very cheap, and don’t go off.
- The amount of glucose in one tablet is small, 3g or maybe 4g if glucose tabs. You can break them in half to get very specific hypo treatments.
- Treating hypos should be seen as medicine, just like insulin. Not as a rationale to have a bit of sugar, haribos or some crap like that. It’s very easy to create confusion by using “tasty” treats instead of treatments. It’s not long before the young person is saying, “I don’t like Haribo anymore, I want skittles”. You can imagine where this leads. Dani, remember, as parents, we create an environment that informs the choices; we are not held hostage by Grace and Jude.
- Liquid versions of glucose only, such as Lucozade, Gatorade, Powerade, etc, are not ideal for a few reasons:
- The carb content changes over time and between countries based on government regulations.
- Some “Glucose” drinks use a Glucose syrup that contains sugar – sneaky
- They are bulky to carry
- Hard to measure a specific amount
- Expensive
- The list goes on
- A liquid version might go down easier and a bit quicker. Why not have a glass of water with the glucose tablets? That’s free!
- Small shots of glucose liquid such as Lift and Glucojuice are ok but are seriously expensive and hard to measure when you want less than 15g.
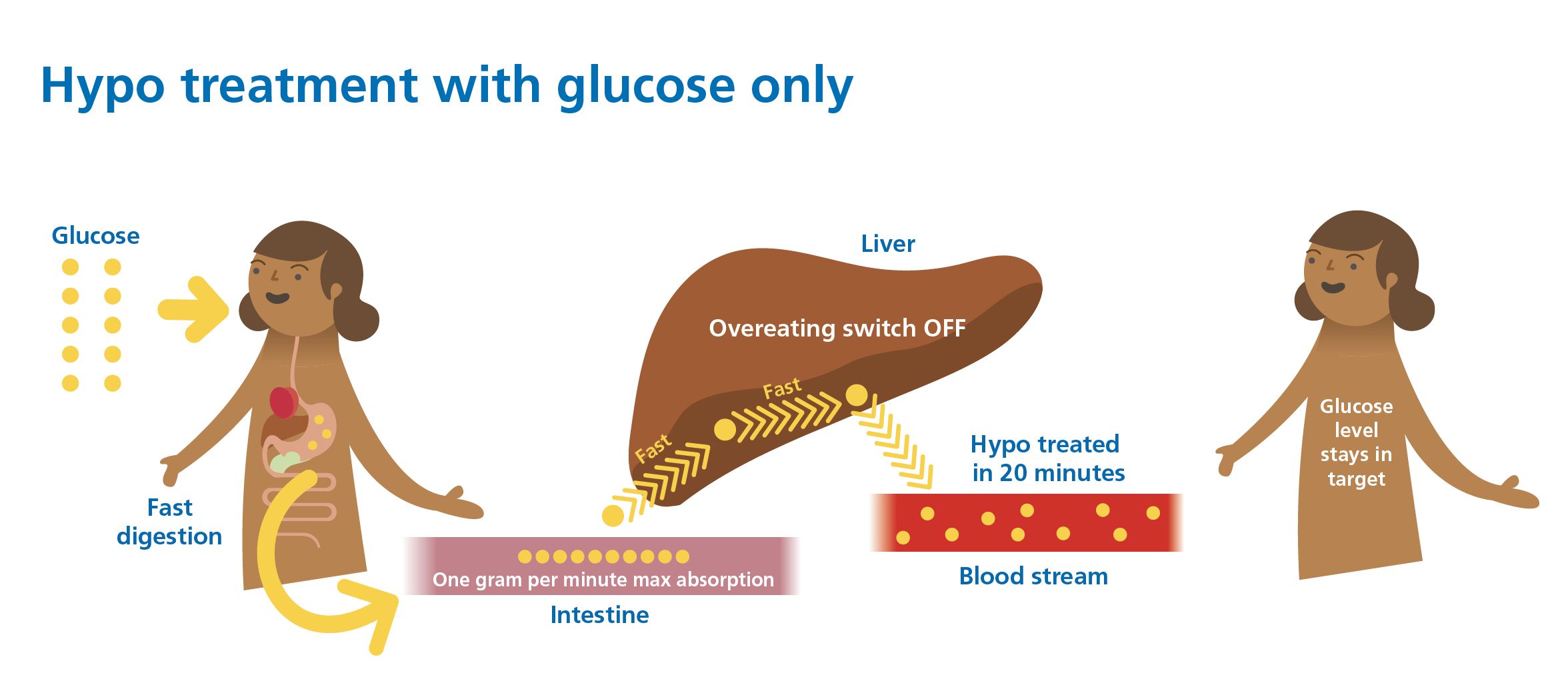
This picture pulls it all together. We will get to the overeating switch when we talk about sugar momentarily.
What about preventing hypos and using trend arrows to change the hypo treatment amount?
What a great question. It makes absolute sense to have less glucose when the arrow is falling slowly and more when it is rapidly falling. Also, less for preventing a hypo and more for treating. I feel another table is required.
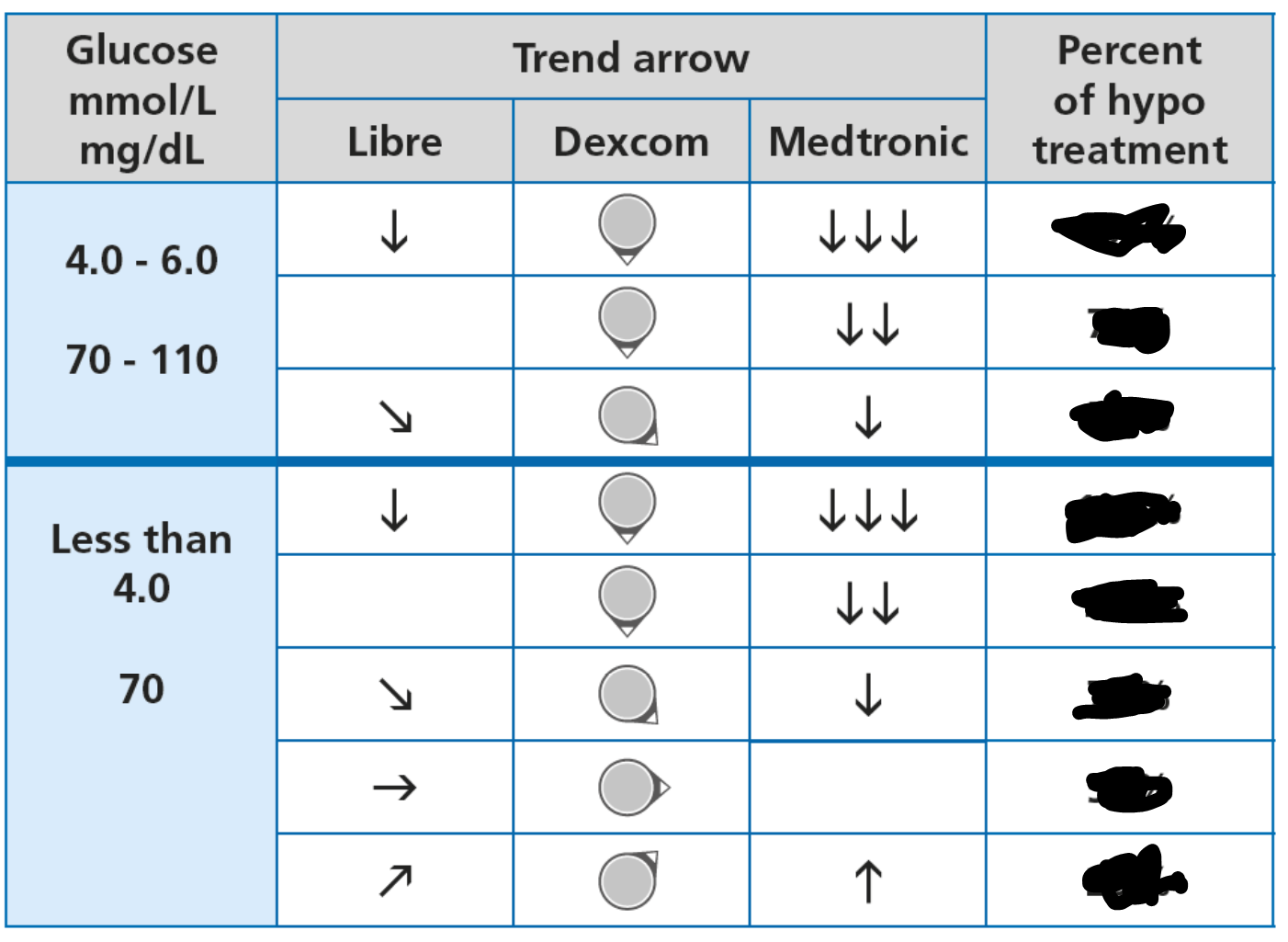
I will leave you guessing for now. I flesh this table out in Dynamic Glucose Management, the MATCH section of GAME-SET-MATCH.
Why is sugar such a rubbish hypo treatment?
This picture explains it beautifully. Sugar is just too SLOW! Treating a hypo with one sugar treatment can take up to an hour.
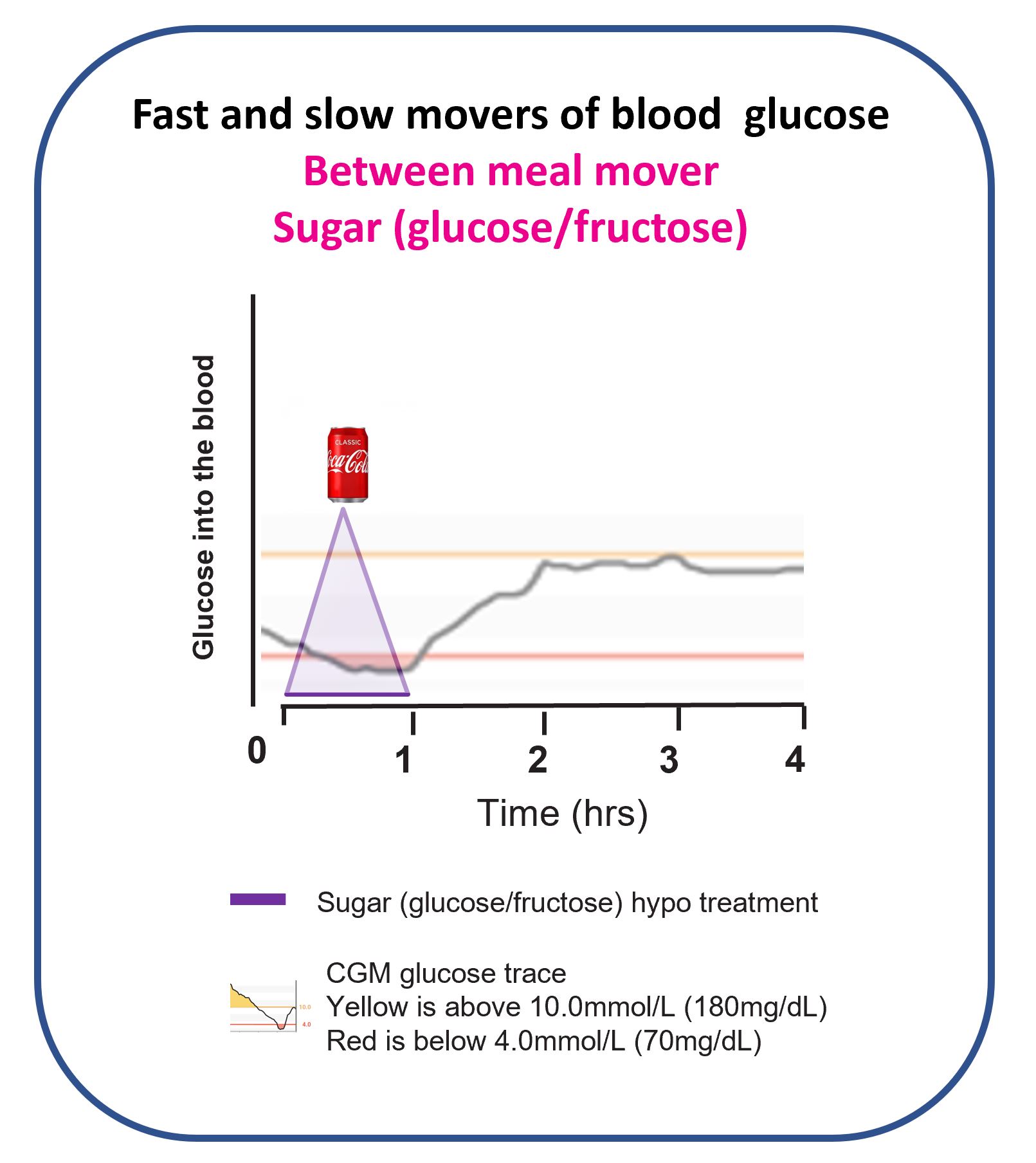
What are you going to do when the glucose level is still low twenty minutes after treating with sugar?
Have another one, maybe even a third. Then, boom, the stockpile of glucose in the intestine gets absorbed, and the glucose level heads north, rapidly! Exactly what happened to me just before bed on Christmas day 2018.
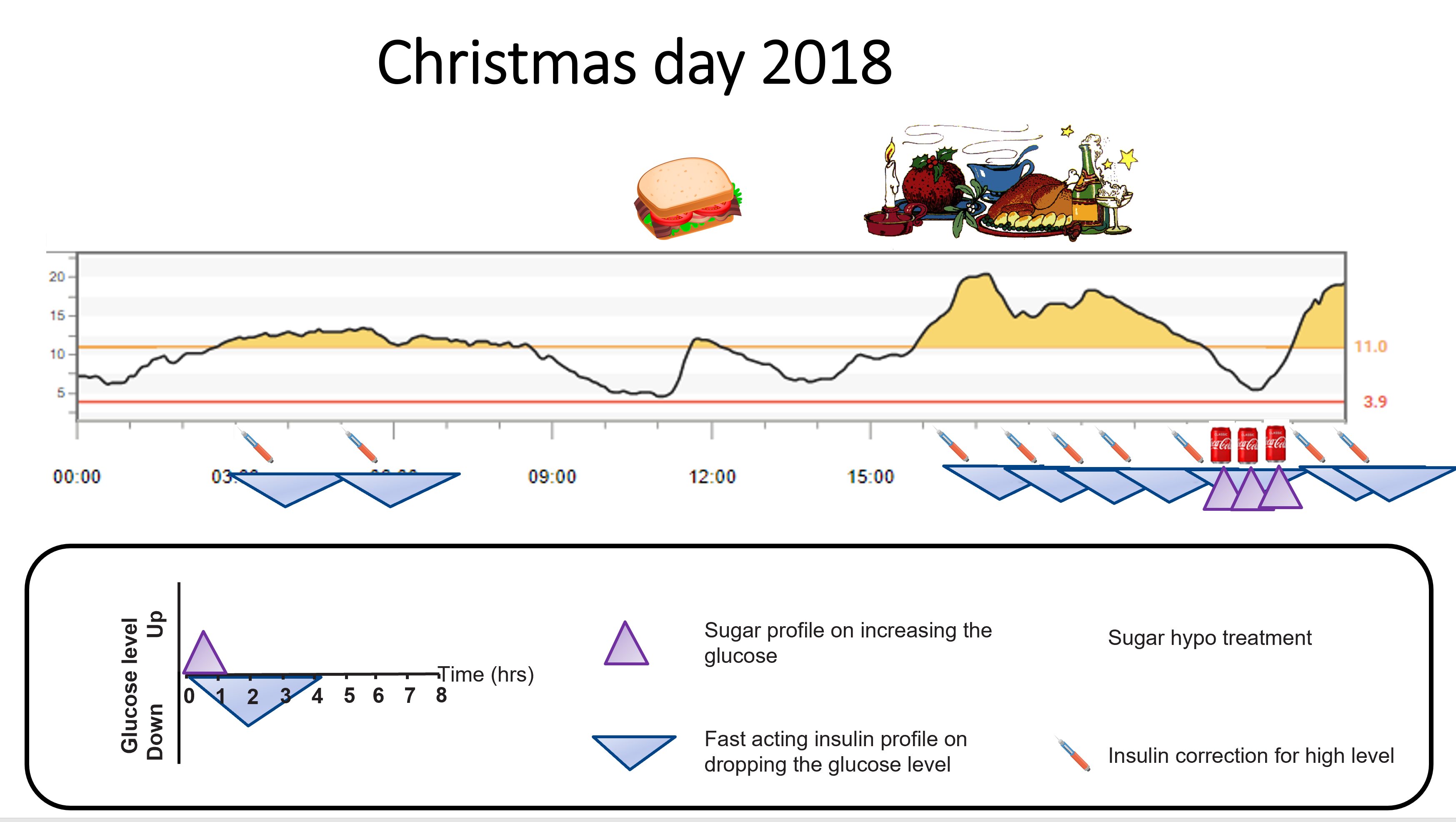
Time for a picture to explain why this happens.
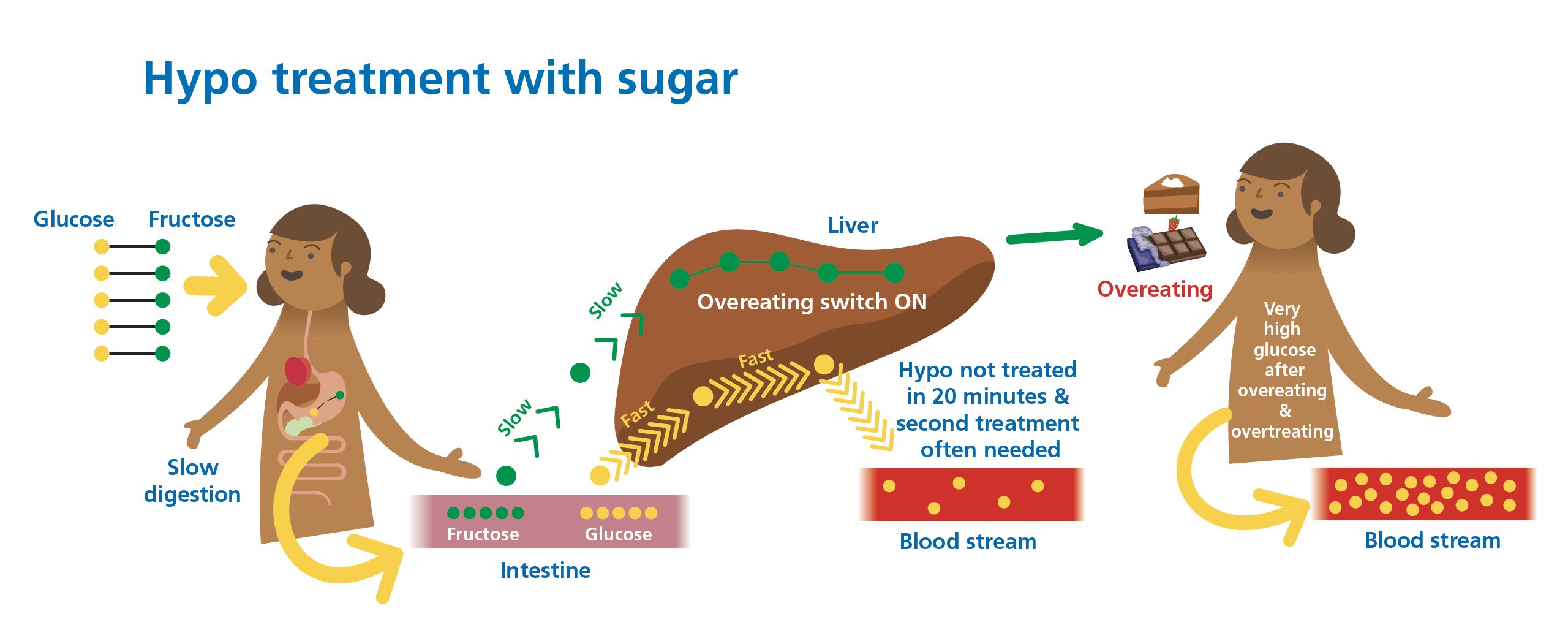
Key takeaways:
- Sugar is one glucose and one fructose molecule joined by a bond that gets broken during digestion.
- The glucose gets into the bloodstream quickly, whilst the fructose gets stuck in the liver. This means the hypo treatment is only half effective.
- The glucose is usually still lower than 4.0mmol/L (70mg/dL) after twenty minutes, and a second treatment is taken. Eventually, 40 minutes later, the hypo is treated.
- Overeating switch on? The fructose from sugar gets stuck in the liver and triggers a metabolic cascade that sounds the starvation alarm. Hunger hormones are pumped into the brain, and you can guess what happens next… the fridge is raided to quell the hunger,r and the glucose starts to climb Everest.
- Dear John, you must listen to this amazing Podcast – Rick Johnson’s revolutionary insights into sugar and obesity. Here is my whiteboard that summarises it. Dani, gloss over this!
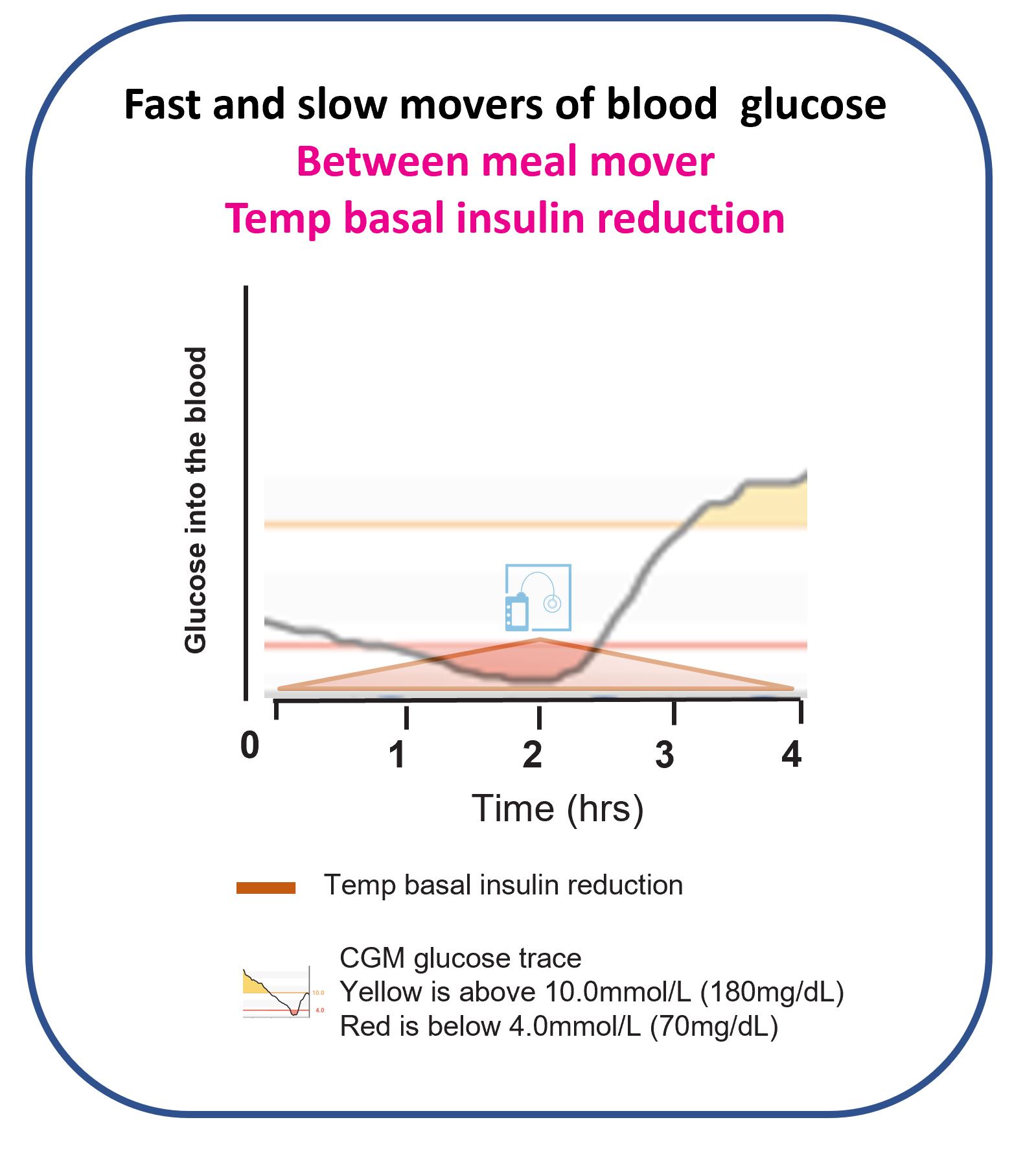
Is a temporary basal rate not effective in preventing or treating hypos?
Absolutely not; it’s the SLOWEST mover of glucose. Remember our discussion in the Basal Insulin section.
It’s the same as shutting the stable door after the horse has bolted.
Over the last few parts of the foundations sections we have discussed all the between meal movers of glucose, both FAST and SLOW. Let’s put them all together.
Next step. Fast and Slow Movers of Glucose