

You have made it to the crucial section of the blog.
Have you completed the Foundations section?
Only continue if you have worked through and understand the Foundations section.
Also, you must be using a CGM device with alarms.
Your CGM device will be your teacher and your friend, and it will keep you safe. It will also make you angry from time to time, especially when it alarms in the middle of the night!
Dynamic Glucose Management has been in development since my diagnosis in 2008. Thirteen years of trial and error. Thirteen years of tinkering after repeated failures. Thirteen years with my nose in the research to understand why the glucose behaves in mysterious ways. I hope to cut your learning time to six months or less.
The EUREKA moment came on Christmas Day 2018!
After more than doubling my Christmas dinner insulin dose to keep up with the high-flying glucose! More on that shortly.
I am sure you will understand the three pillars of Dynamic Glucose Management;

However, you will need to apply trial and error with lots of tinkering to make it your own. I will be by your side, but it’s your responsibility to put in the work.
Before we get into GAME-SET-MATCH, indulge me. Listen to my Christmas Day story.
Grace, you were a year and four months old, and we just found out Jude was on the way, a time to celebrate. Grandma and Grandad were on the way down from Bury, and the smell from the kitchen was sumptuous.
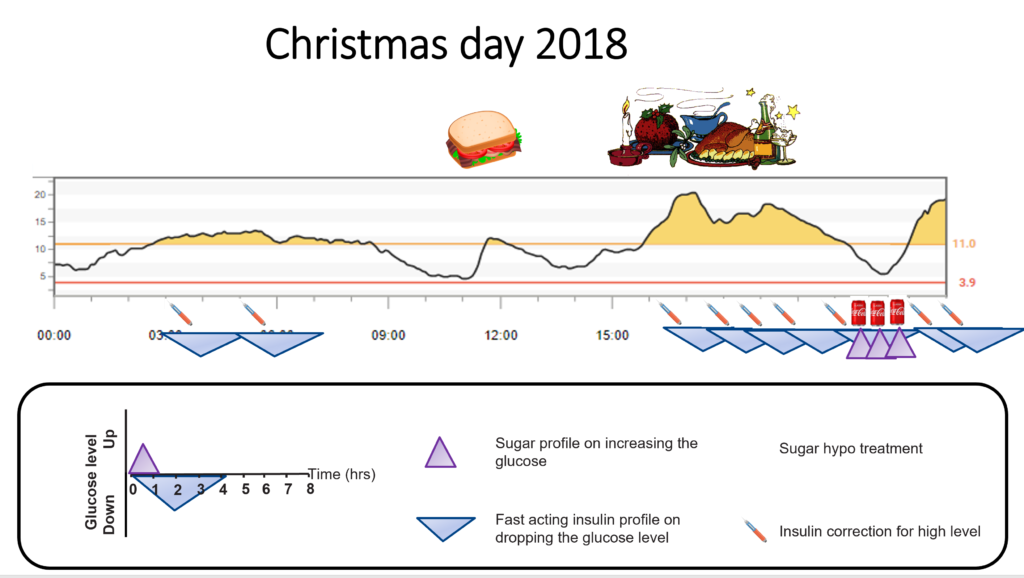
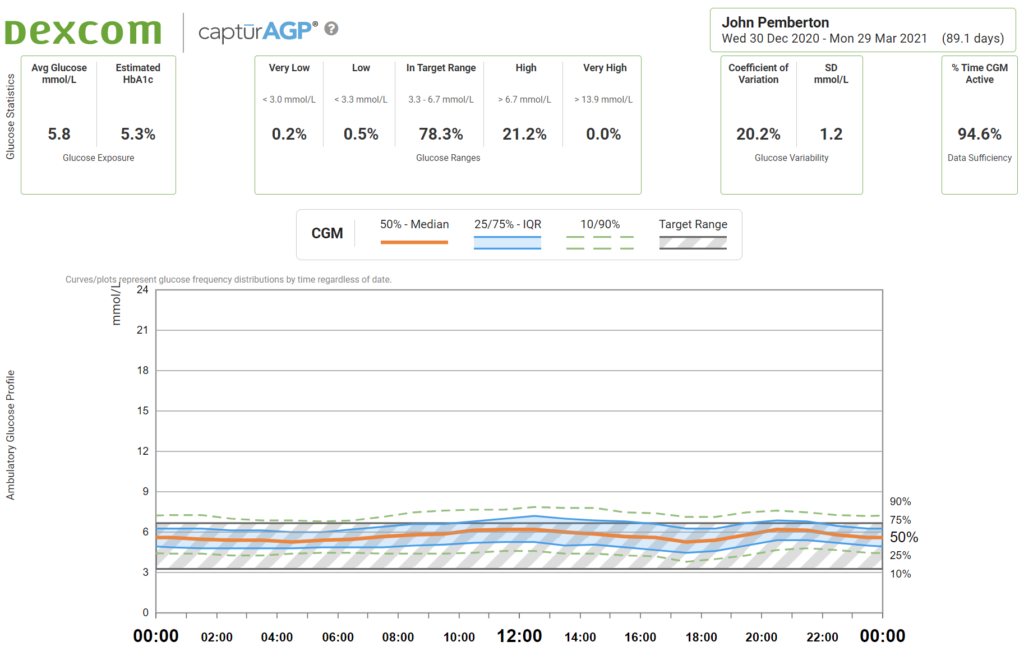
I decided to skip breakfast, have a bacon sandwich for lunch, and stuff my face with Christmas dinner. I set the CGM high alert at 11.0mmol/L (200mg/dL) and planned to correct highs with insulin. Finally, I intended to prevent hypos with Coca-Cola.
I had been duped by the Christmas day marketing with Santa chugging a bottle of the stuff. Or it was the name of the man who invented Coca-Cola, John Pemberton!
Here is how the day played out.
Even at the age of 38, the Christmas day excitement kicked in and required a couple of corrections overnight.
Skipping breakfast and having a bacon sandwich for lunch worked well. Then, all hell broke loose once I got stuck into Christmas dinner!
I had done all the “right” things. I used my scales to count the carbs within an inch of their life. I gave the insulin twenty minutes before the meal. When I ate extras, every gram of carbs was accounted for.
Then, boom, an hour after starting to eat, the glucose set off up the mountain. It took five separate correction doses over five hours to get the glucose back in range.
To say this annoyed me is putting it lightly! I don’t like seeing high levels at the best of times. I hated feeling bloated and watching the glucose go higher and higher despite correcting every hour.
The total dose required for the Christmas meal was 10 units (200g carbs), but my corrections came to a further 15 units, taking the dose to 25 units.
I understood high-fat meals need extra insulin. I knew I would need more to cover high fat’s insulin resistance effect, but I was not anticipating 150% extra!
The extra insulin was not what annoyed me.
It was how SLOW the corrections were working. Fast-acting insulin takes 90 minutes to peak and lasts about four hours.
Remember this from the Correction Insulin page of the foundation’s section?
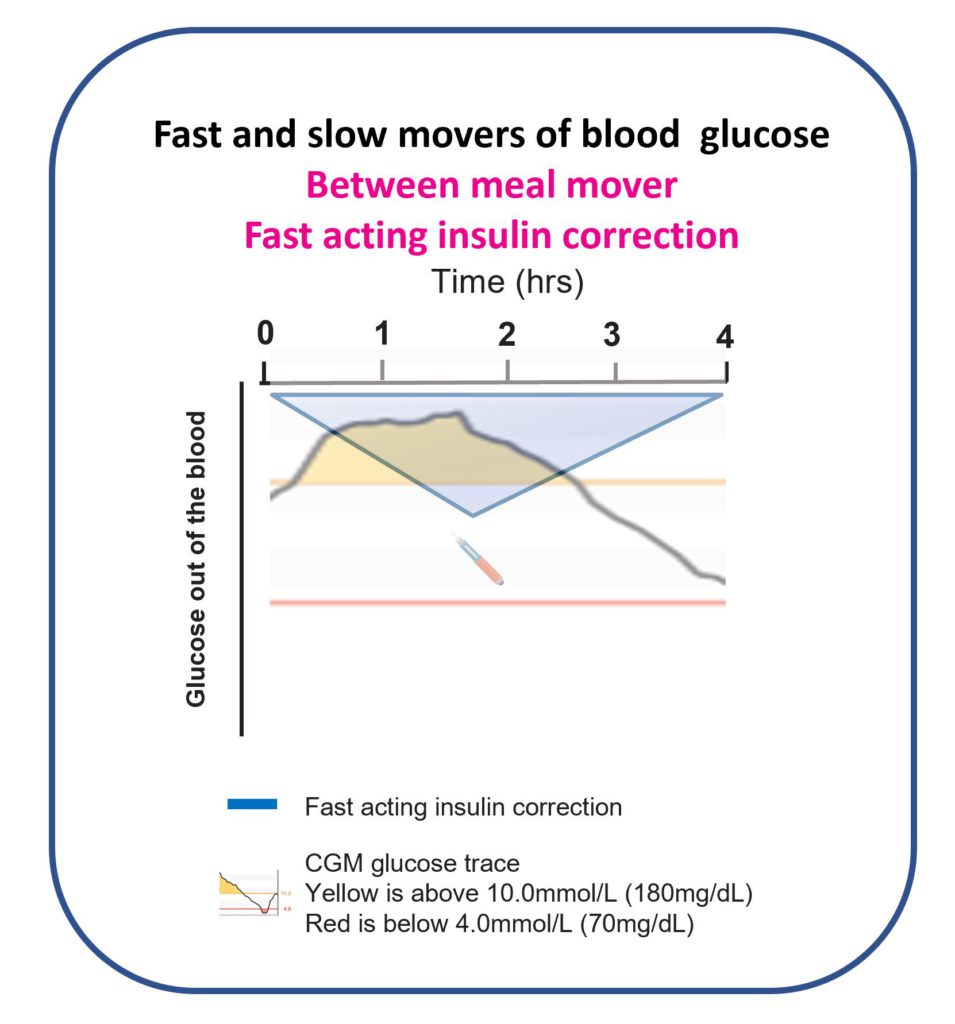
I gave one correction, then another, then another, and another! Four hours later, I could finally see some results.
By this point, I had so much insulin stacking up that only one thing could happen. The glucose started to nosedive.
I knew how much insulin I had given and started to panic. I reached for Coca-Cola. I had 200ml, which is 18g of sugar.
Remember this from the Hypoglycaemia page?
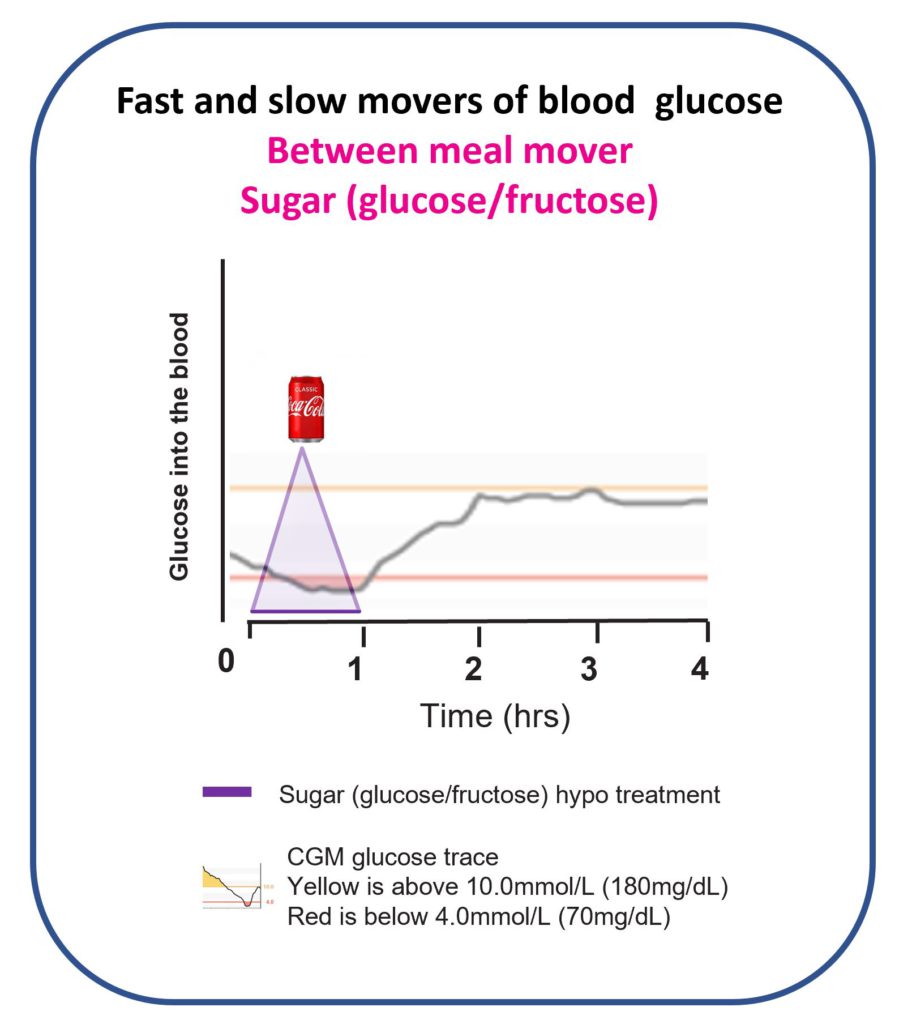
I waited 20 minutes, still dropping—another 200ml and now feeling bloated. I waited 20 minutes, still falling. A final 200ml and a stomach like Santa. Finally, the glucose levelled out.
Not for long; the glucose headed back up the mountain. With three Coca-Colas back-to-back, I was now stacking glucose!
I threw in two more corrections before bed with no visual effect on the CGM, which concluded one of my most frustrating days with diabetes.
This happened despite having diabetes for ten years, being a Diabetes Dietitian, and thinking I was an expert in type 1 diabetes.
This was indeed a lesson that The Glucose Never Lies. I was certainly no expert, not even in my diabetes.
It was time to get back to the drawing board!
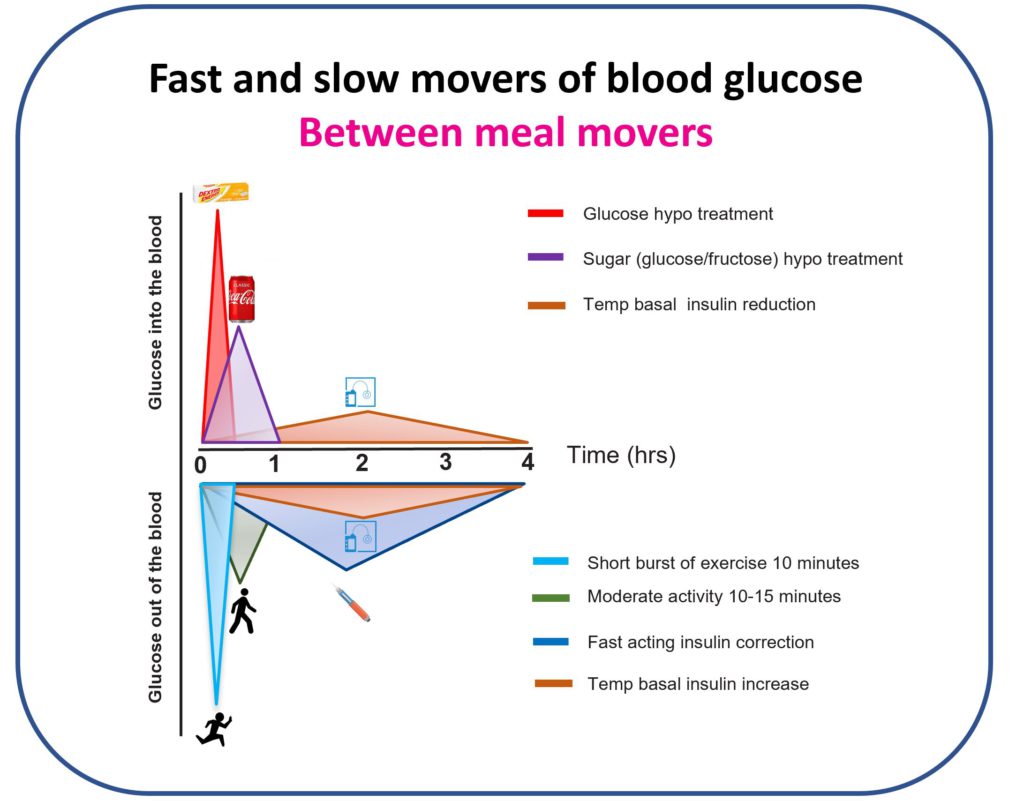
I got my nose in the books and quickly developed a new model of how to think about type 1 diabetes. It was time to start thinking about the different speed tactics to move the glucose up and down.
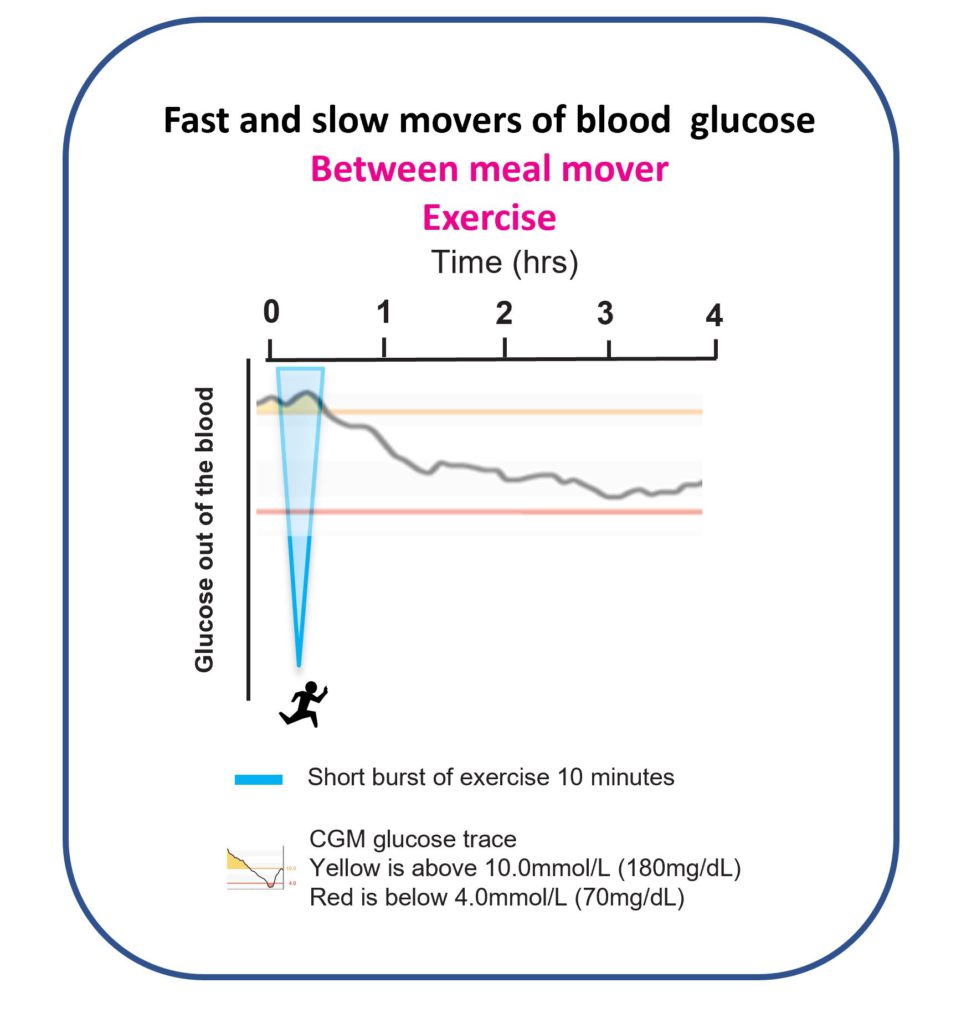
It became clear there were tactics that moved the glucose level up or down between meals very FAST and those that were painfully SLOW.
I had been prioritising the slow movers because that’s what I had been taught.
I was correcting high glucose levels between meals with corrections and using a mix of temporary basal reductions and sometimes sugar to prevent and treat hypos.
It was time to shift gears and get in the fast lane.
Can you guess what tactics I used on Christmas Day 2019?
Fast forward to Christmas Day 2019.
Grace, you were two and a bit, and Jude had joined the party. I was determined to have a much better day and planned to prioritise using fast movers of glucose to tackle the highs and lows.
I planned to skip breakfast, have a bacon sandwich for lunch, and stuff my face with Christmas dinner just as in 2018. I set the CGM high alert at 11.0mmol/L (200mg/dL), but this time, I planned to correct highs with short bursts of exercise.
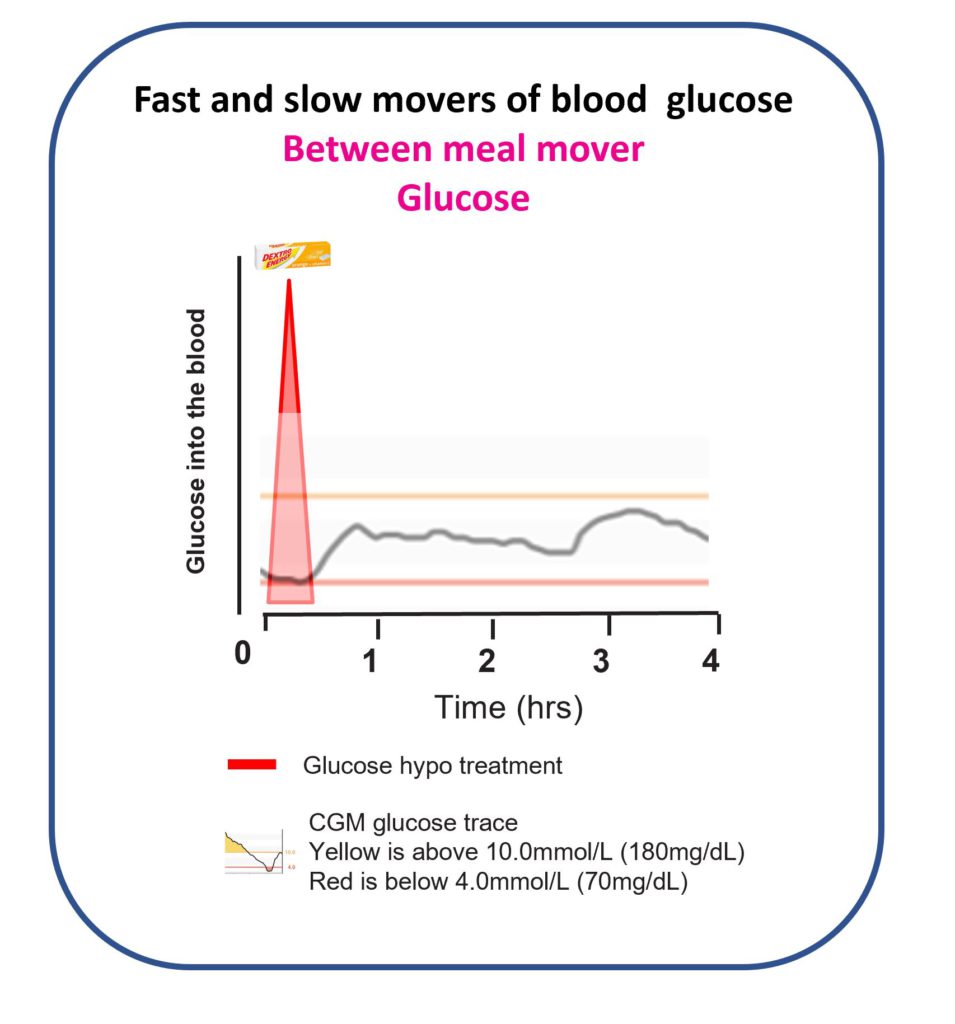
I turned down the Coca-Cola, sorry John Pemberton of sugar beverages fame, and had my dextrose tablets at the ready. Here is how the day played out.
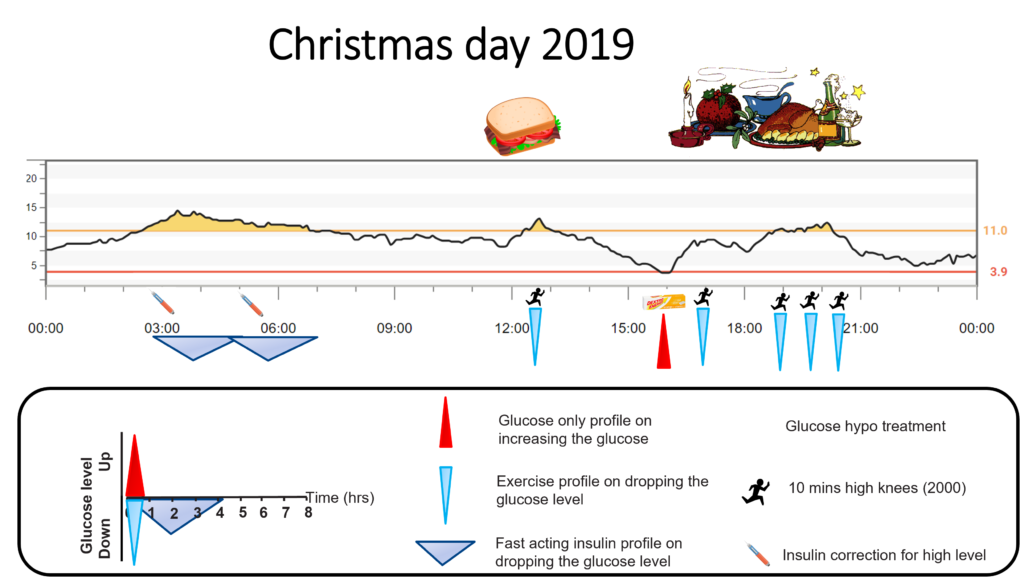
At 39, the overnight excitement was still there! Two corrections required. Even I am not obsessed enough to do exercise at three and five in the morning.
I started with nothing for breakfast and a bacon sandwich for lunch. The glucose hit 11.0mmol/L (200mg/dL), and the experiment began.
I started jogging on the spot, doing what I call high knees. Ten minutes later, I had done 2000. Quick as a flash, the glucose was back in target. Just as the Activity and Exercise page predicted!
Just before Christmas dinner, the glucose was drifting low. My standard hypo prevention treatment was 18g, six dextrose tablets, or 200ml of Coca-Cola.
I had learntthat sugar takes longer to work than glucose and often leads to unnecessary double or triple treatments. Precisely what I experienced in 2018.
The glucose was only drifting down, so I only gave half a hypo treatment. Three dextrose tablets and hey presto, a nice little bump to mid-range. I am sure, precisely what you were expecting after reading the Hypoglycaemia page?
Christmas dinner came, and I did not hold back. Just as in 2018, I got stuck in and ate my way up to 10 units (200g carbs) worth of Christmas day goodies.
I started to watch the glucose climb, spurred on by my earlier success, I put in 2000 high knees (10 minutes) before the high alert went off. Bosh, the glucose, had been whacked on the head.
Two hours later, the Christmas pudding and cheese and crackers must have been digested. The high alert sounded, and the knees started pumping. Over the next hour and a half, I did three lots of 6000 high knees, taking the total to 10,000 spread across the day.
It worked a treat. My glucose was in range by bedtime, there was no insulin stacked up, and I could drift off to sleep safely.
No sane person will do fifty minutes of high knees each day to manage their diabetes. However, no sane person would eat Christmas dinner every day.
This was an extreme example of how prioritising fast movers of glucose leads to more time in range and less insulin stacking.
Christmas Day 2019 was when the three pillars of Dynamic Glucose Management emerged.
Stop Highs – Use short bursts of activity to lower high glucose between meals, not insulin corrections.
Stay in Target – Eat three well-balanced meals.
Prevent Lows – Use glucose-only treatments, not sugar.
What followed was several months of intensive trial and error with continual tinkering.
By April 2019, Dynamic Glucose Management was fully formed.
Stop Highs – GAME.
G: Glucose time in range desired
A: Alert on high set according to the desired time in range
M: Mode of exercise that can be done anywhere.
E: Exercise on high alert based on glucose value and arrow
Stay in Target – SET.
S: Start insulin before eating
E: Eat three balanced meals
T: Ten minutes of activity after eating
Prevent Lows – MATCH
M: Measure weight to calculate hypo treatment
A: Always use glucose only, not sugar
T: Try to prevent lows
C: Change treatment based on glucose value and arrow
H: Have patience and wait 20 minutes
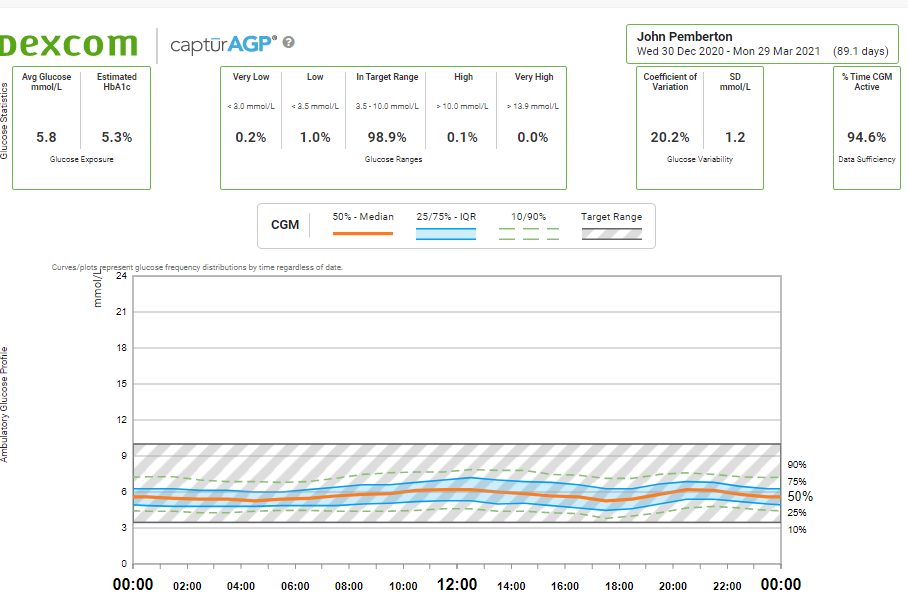
Dynamic Glucose Management rocketed my time in range from 85% to 99%
This blows the current (April 2021) automated pancreas systems out of the water.
I have tried DIY looping, Control IQ, and 670G. They all work well. Each helped me to roughly 85% time in range with 3% low, but this is no match for 99% and 1%!
It is true that AID system do a lot of the heavy lifting, which means you do not have to spend as much energy managing diabetes. They correct highs with more insulin and try to stop lows by slowing down or suspending the insulin.
This works amazingly overnight when there is only glucose output from the liver to contend with.
In fact, on both Christmas days, an automated pancreas system would have dealt with my overnight excitement, and I would not have been woken up twice.
However, only using insulin, a SLOW mover of glucose, will never keep up with the glucose when there is food, exercise, and daily stress in the mix.
Automated pancreas systems only manage 50% of the time in the optimal healthy glucose range for people without diabetes, 3.3-6.7mmol/L (60-120mg/dL).
Dynamic Glucose Management enabled me to hit 80% in the optimal glucose range of 3.3-6.7mmol/L (60-120mg/dL).
However, for nights of luxurious sleep and optimal daily control, I think using an AID System and supplementing with Dynmaic Glucose Management during the day is the best approach.
However, nothing in life comes for free. Dynamic Glucose Management requires time, love, and attention. It takes a particular type of person to flourish using it.
Grace and Jude, I think you will want to take on the challenge. But if you do not, no problem; it’s your diabetes and your life. We will get you on an AID system, and we can add a bit of Dynamic Glucose Management when you are ready.
The only way this could be beaten is by following a very low carbohydrate diet. I have experimented with different levels of carbohydrate restriction. Read the 120-day carbohydrate experiment.
My current opinion is,
“There is no need to severely restrict carbohydrates to achieve near-perfect control if you are using Dynamic Glucose Management.“
The beauty of Dynamic Glucose Management is that you do not need to go keto or very low carb (50g a day). Just be prepared to use fast movers of glucose between meals.
Dani, I have no doubt you are thinking.
“This is ok for you as an adult who is obsessed with glucose control. What about Grace and Jude?”
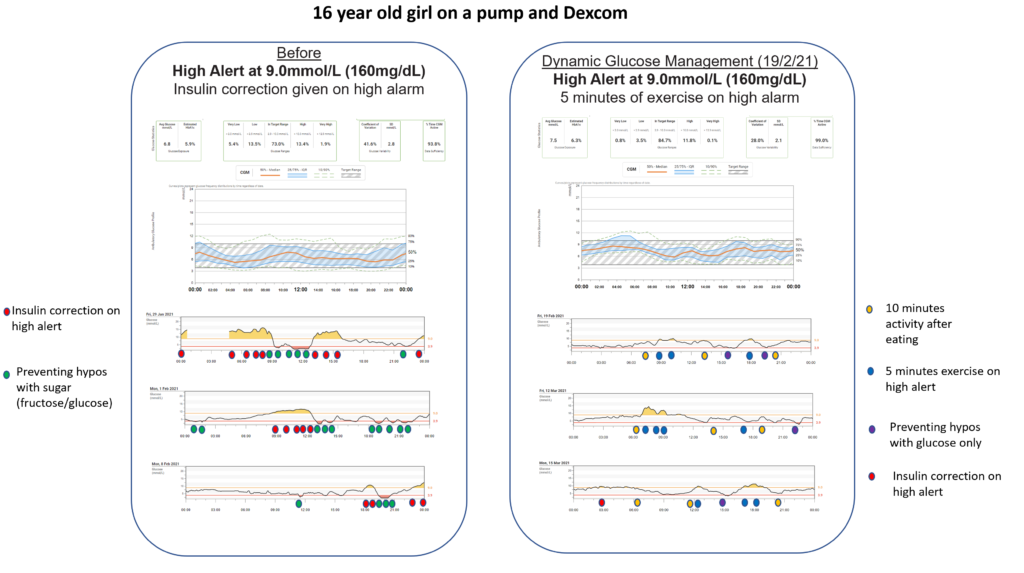
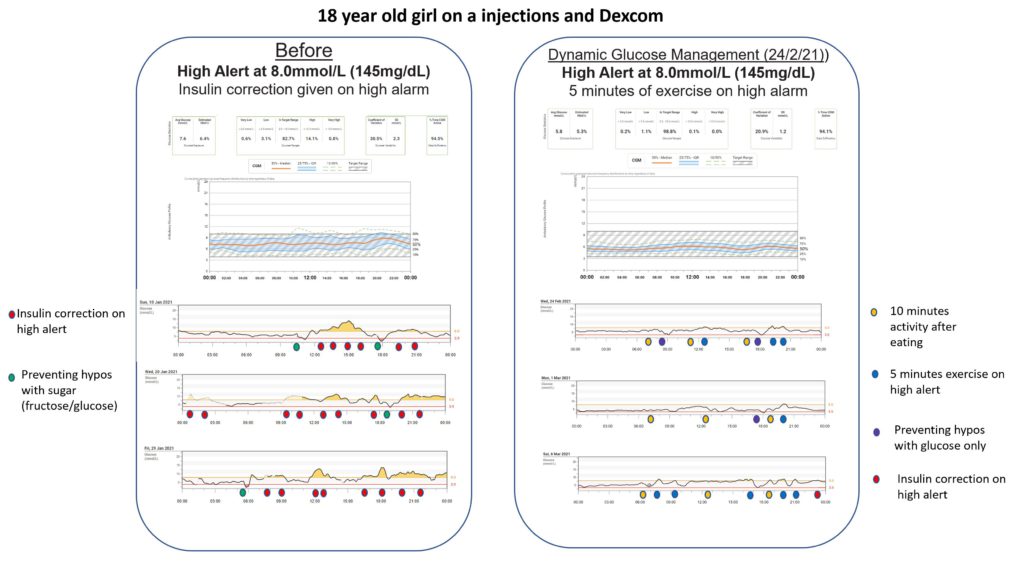
I created a CGM structured education program that teaches Dynamic Glucose Management to children and young people with diabetes and their families.
We introduced the programme at Birmingham Children’s Hospital and recently published the first fifty educated. I have broken down the paper in the research section for John.
The results showed that using Dynamic Glucose Management stopped problematic hypoglycaemia and increased time in range by 10% on average.
The young people who scored highest on using Dynamic Glucose Management had the most time in range, 70-90%.
Our audit of the first hundred educated looked at what elements of Dynamic Glucose Management produced the highest time in range.
Those with at least 80% time in range prioritised short bursts of exercise to correct highs, changing before meal insulin based on glucose value and arrow, and preventing lows with glucose.
I hope I have convinced you that Dynamic Glucose Management is worth exploring.
The next steps are to work through:

Then, you will get to the infographic that pulls everything together on one sheet.
Don’t be cheeky and jump ahead, Jude. Put in the work first.
Start with GAME
