Core Guide
Exercise and Type 1 Diabetes
Making exercise predictable enough to manage, without pretending it can ever be perfectly controlled. From ten minutes after a meal to training for an endurance event: the same physiology, the same three variables.
Ask Grace
Want to ask what insulin on board, starting glucose and trend arrows mean for the sport you actually do? Ask Grace.
TL;DR
- Insulin on board is the dominant driver of exercise hypo risk. The 90-minute window and the Three-Hour Rule are how you manage it.
- Three variables decide almost everything: insulin on board, starting glucose, trend arrows. Address these first.
- AID changes the levers, not the physics. Announcing exercise and pre-emptive reductions matter more on an AID system, not less.
- Assess before you start and every 30 minutes. A weight-and-glucose carbohydrate guide sits further down, sourced from the live GNL explorer.
Start here if exercise feels daunting
If formal exercise management feels like a lot, the most accessible entry point is activity snacking: ten to twenty minutes of movement after the meal that produces your biggest spike. It is lower risk than structured exercise and it has its own dedicated guide.
Major in the majors
Three variables decide almost everything
If exercise has felt chaotic, start here. Across almost all forms of exercise, glucose behaviour is dominated by three variables, in order of importance.
1 · Most important
Insulin on board
Recent bolus insulin is the dominant driver of exercise hypo risk.
2
Starting glucose
Where you start shapes where you land, especially for aerobic work.
3
Trend arrows
Direction and speed of change. Numbers without direction are incomplete.
Insulin on board is also the variable you can most directly change. When these three are prioritised first, most exercise-related hypoglycaemia and volatility becomes predictable from the starting conditions.
What this guide is for
Exercise is not random. It is fast physiology meeting slow insulin.
For people living with type 1 diabetes, exercise can feel uniquely destabilising: drops that arrive fast and hard, spikes that linger, sessions that look identical on paper but behave very differently in real life. The common conclusion is that exercise is “unpredictable”. That conclusion is understandable, and usually wrong.
Exercise does not introduce randomness. It introduces fast, powerful physiology into a system otherwise governed by slow, blunt insulin. When you understand the dominant drivers, patterns appear, and with them a clearer picture.
This guide is built around heuristics to experiment from, grounded in the evidence base (the EASD/ISPAD 2025 consensus, the ISPAD exercise chapter, and GNL’s own causal modelling) and tailored by individual response. They are not rigid rules. They are starting points that survive contact with CGM and real life.
The core problem exercise creates
Exercise is hard to manage in type 1 diabetes not because it is dangerous, but because it amplifies insulin action.
Muscle contraction increases glucose uptake. Blood flow accelerates insulin delivery. Counter-regulatory hormones may push glucose out of the liver. These processes act quickly. Injected or pumped insulin does not.
Why exercise hypos are usually insulin problems, not exercise problems
Large glucose drops during exercise are rarely caused by exercise itself. They are almost always caused by supercharged insulin action: exercise increasing blood flow and glucose uptake, amplifying the effect of insulin that is already present. This is physiology doing exactly what it should.
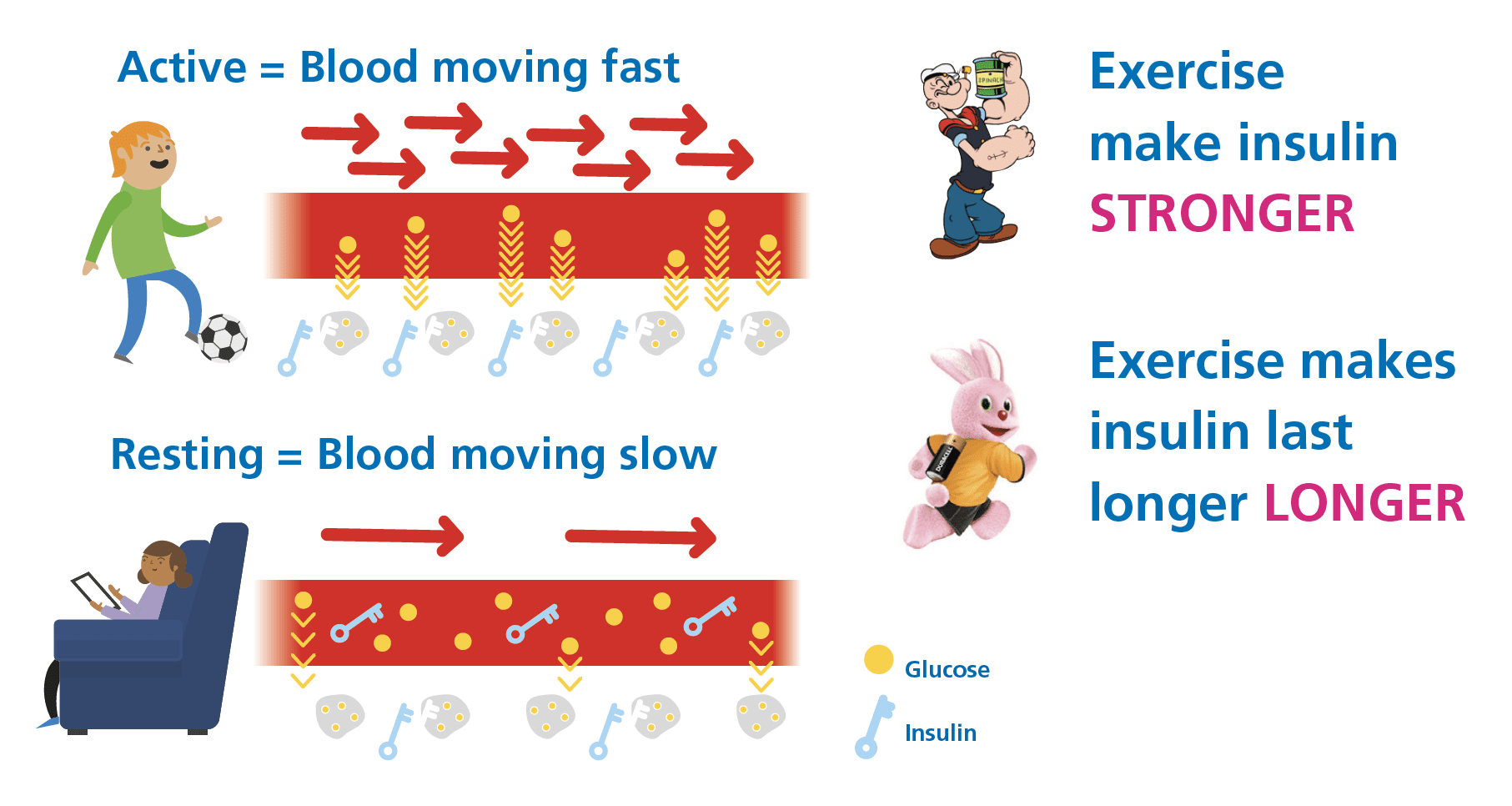
The implication is practical: reducing insulin on board before exercise, through timing, bolus reduction, or basal adjustment on a pump, addresses the actual cause rather than the symptom.
Counter-regulation is real, but blunted in T1D
In people without diabetes, falling glucose during exercise triggers a prompt counter-regulatory response (glucagon and adrenaline release glucose from the liver). In long-standing type 1 diabetes this response is often blunted, which is part of why the same session that a friend without diabetes shrugs off can drop you hard. The muscle also acts as an endocrine organ: contracting muscle releases myokines and increases insulin-independent glucose uptake, which continues for hours after the session ends.
Risk factor 1, the one that matters most
How much bolus insulin is on board
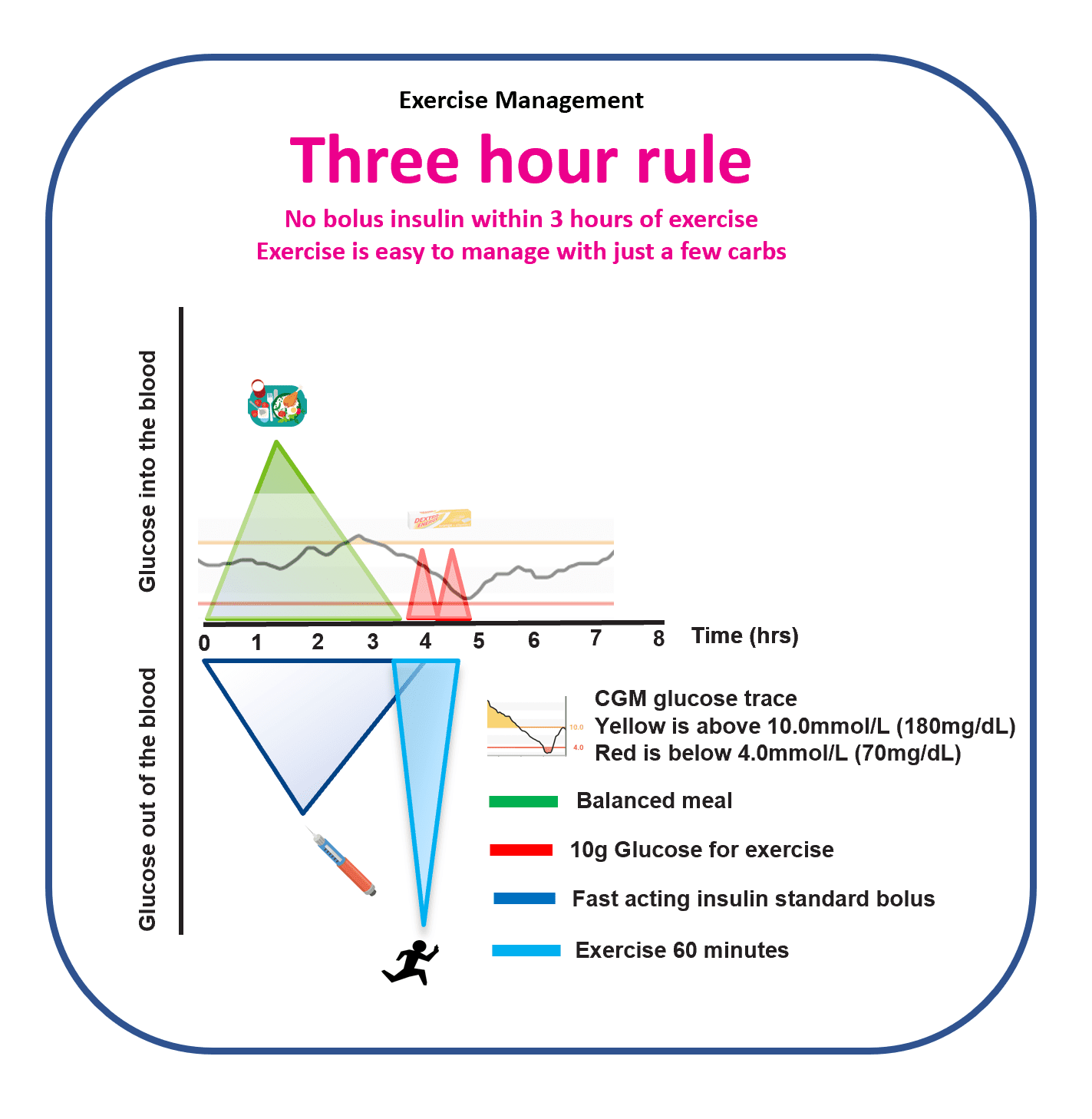
Because exercise amplifies insulin action, the single most important thing to know before you start is how much bolus insulin is still working. This is the main reason to try to eat and give insulin about three hours before a planned session, or to exercise first thing in the morning before any meal bolus: both leave you with low insulin on board and a far more predictable session.
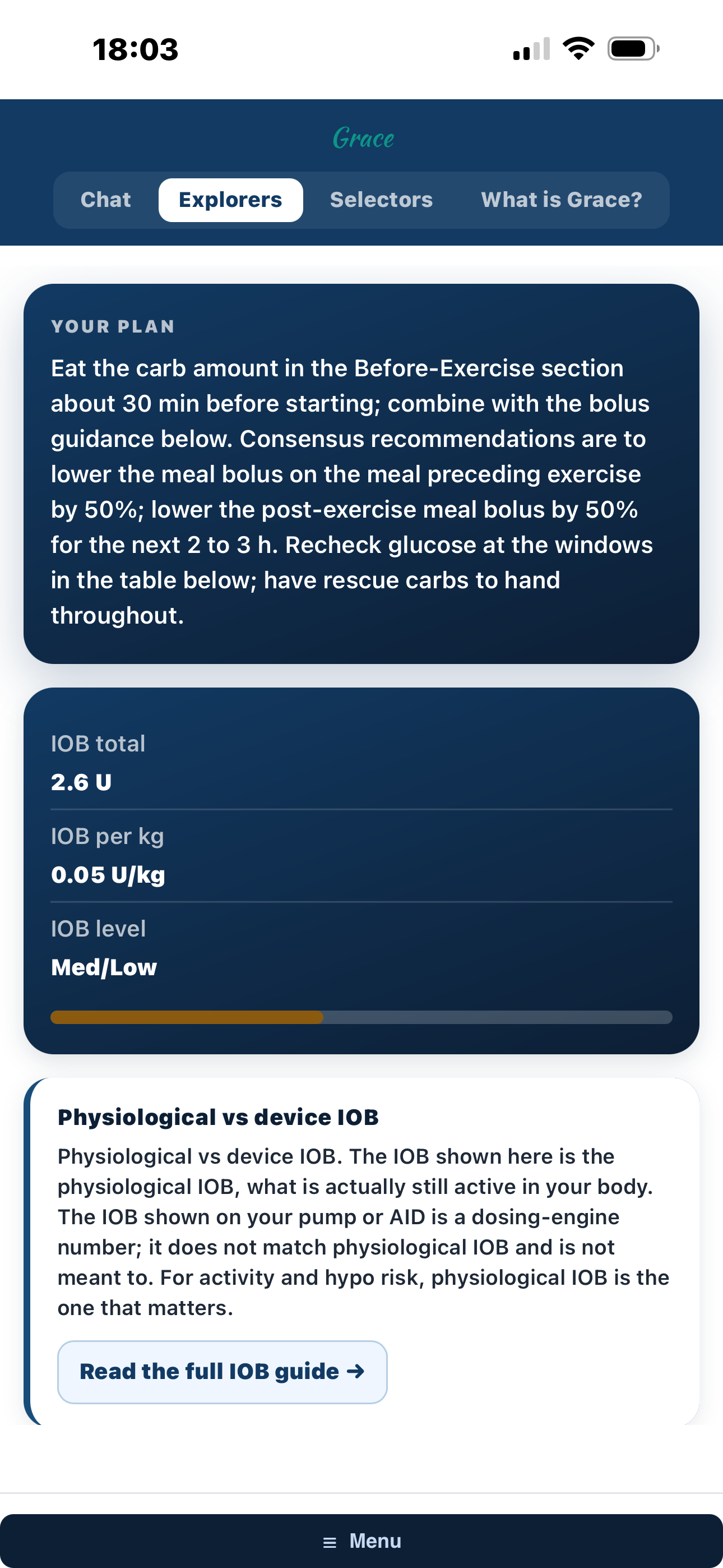
Your device IOB figure cannot be fully trusted. The insulin-on-board number on your pump or app is driven by its Active Insulin Time setting, which is often shorter than insulin genuinely stays active in the body. When the screen shows a low or zero figure, meaningful insulin can still be working. Around 40 to 45 percent of a typical bolus can still be physiologically active even when the device reads low. Rather than trusting the number, think in terms of when your last significant bolus was. For the full detail on why device IOB and physiological IOB differ, see the Insulin On Board guide.
A simple, robust way to think about it:
- Bolus within the last 3 hours: insulin on board is meaningful. Hypo risk during exercise is high. Plan a reduction or carbohydrate.
- Bolus more than 3 hours ago (or fasted / basal only): insulin on board has fallen. Hypo risk is reduced, and the session becomes far more predictable.
The 90-minute fuel window
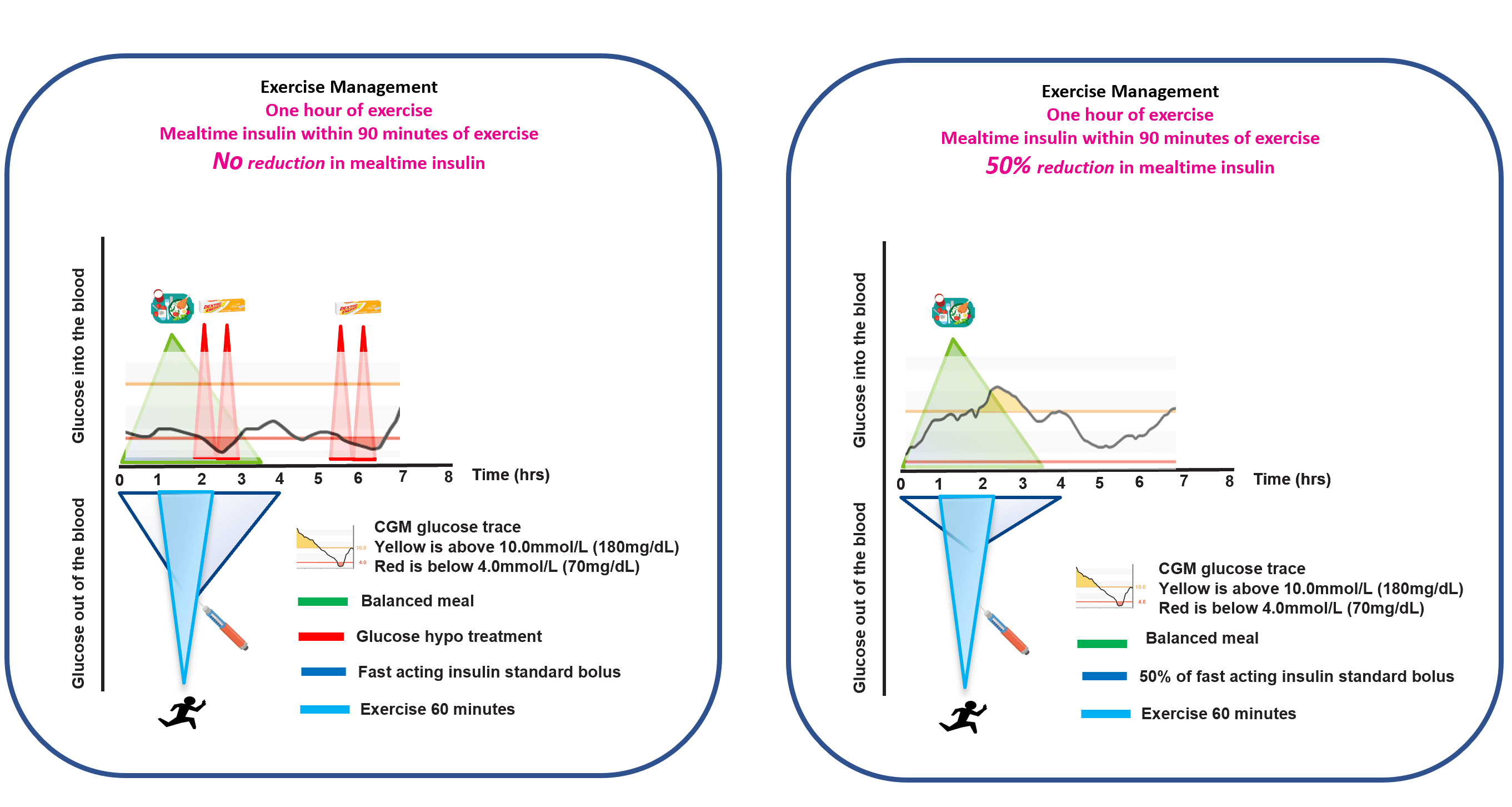
If you have to eat close to exercise, aim within 90 minutes
When exercise falls within roughly 90 minutes of a meal bolus, insulin action is often near its peak, and a bolus reduction is commonly needed to avoid a predictable hypo. Exercise and peak bolus action overlap.
The practical consequence: if you are going to eat within about two hours of exercise, try to make it within 90 minutes of starting, so you can begin the session having already reduced the bolus, rather than trying to catch a fall with carbohydrate mid-session. Smaller, earlier interventions consistently outperform larger, later corrections. Even an AID algorithm cannot override the physiology of this window; it can only react to the glucose that results.
Setting the starting insulin conditions
The reduction protocols
Two population-average starting frameworks: 50/50/20 for multiple daily injections, and T25/T25 for an automated insulin delivery system (hybrid closed loop). Both are teaching simplifications, not fixed doses; any insulin change is a care-team decision.
50/50/20: for MDI (multiple daily injections)
For more specific guidance than the general 50/50/20 starting point, GNL’s Exercise Planner uses a graded reduction table by exercise type and duration.
| Exercise type | Up to 30 min | 31 to 60 min | Over 60 min |
|---|---|---|---|
| Aerobic | 25% | 50% | 75% |
| Mixed | 25% | 50% | 50% |
| Anaerobic (HIIT, resistance) | 25% | 25% | 25% |
GNL’s operational reduction table for those wanting more specifics than the 50/50/20 starting point, informed by Rabasa-Lhoret (2001) and the EASD/ISPAD 2025 consensus (Moser, Zaharieva, Pemberton); not a fixed prescription, agree changes with your care team. AID users have a simpler in-built gate and do not need this table.
T25/T25: for AID (automated insulin delivery / hybrid closed loop)
With the pre-exercise insulin conditions set, the starting point is done. The next thing to read, before and throughout the session, is glucose and its trend.
Risk factor 2, read it before and every 30 minutes
Starting glucose and the trend arrow
Once insulin on board is accounted for, the next question is where your glucose is and which way it is moving. This is not a one-off check at the start; it is a running assessment before you begin and roughly every 30 minutes during the session. A number without a direction is incomplete: 7 mmol/L falling fast and 7 mmol/L rising slowly are two different situations.
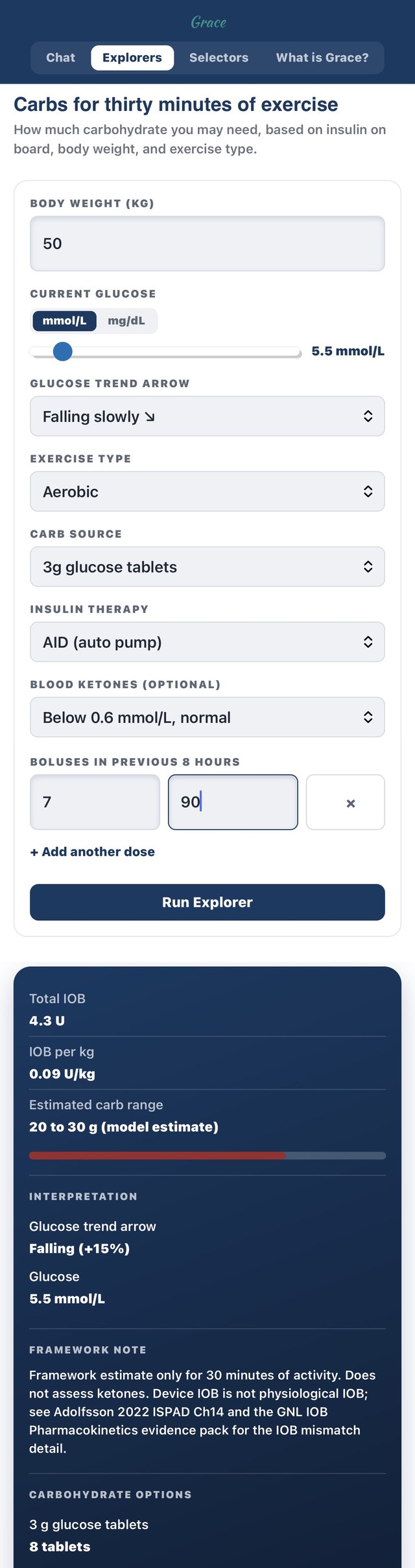
A weight-and-glucose starting guide for carbohydrate
Body weight and starting glucose set the starting carbohydrate for a 30-minute session, with a meaningful recent bolus on board. The rates below are the clinical per-kilogram figures used on this guide: 0.5 g/kg at 4 to 7 mmol/L, 0.3 g/kg at 7 to 10 mmol/L, and 0 g/kg at 10 to 15 mmol/L and above (the higher glucose already provides the headroom). Weight is capped at 60 kg, the population-average ceiling used across every GNL carb calculator. It is an education tool, not a personal dose.
| Starting glucose | 20 kg | 30 kg | 40 kg | 50 kg | 60 kg and above |
|---|---|---|---|---|---|
| 4 to 7 mmol/L (0.5 g/kg) | 10 g | 15 g | 20 g | 25 g | 30 g |
| 7 to 10 mmol/L (0.3 g/kg) | 6 g | 9 g | 12 g | 15 g | 18 g |
| 10 to 15 mmol/L and above (0 g/kg) | 0 g | 0 g | 0 g | 0 g | 0 g |
Below 4 mmol/L: treat the low first and do not start, using the Hypo Treatment approach. At 15 mmol/L or above: hold, and check for ketones before any activity. No single 30-minute window needs more than 30 g, because the gut absorbs glucose at roughly 1 gram per minute.
Adjusting for the trend arrow
Take the figure from the table, then adjust it for the direction of travel (cap the result at 30 g). Worked example, a 40 kg person in the 4 to 7 mmol/L band, starting figure 20 g:
| Trend | Adjust the table figure by | Example: 40 kg, 4 to 7 mmol/L (base 20 g) |
|---|---|---|
| Falling fast | +40% | 28 g |
| Falling | +20% | 24 g |
| Steady | no change | 20 g |
| Rising | -20% | 16 g |
| Rising fast | -40% | 12 g |
Lower insulin on board means fewer carbohydrates. This table assumes a meaningful recent bolus. If your last bolus was longer ago, or you are exercising fasted, the figure drops, often substantially. For a figure based on your actual glucose, trend, weight and recent insulin, use the live explorer.
Clinical per-kilogram rates (0.5 / 0.3 / 0 g/kg), aerobic exercise, with the 60 kg weight cap and 30 g absorption ceiling per GNL calculator canon. See the note above on how these relate to the live explorer.
Different kinds of exercise behave differently
Endurance, mixed, anaerobic and competition
The type of exercise shapes the direction glucose tends to move. The live explorers use three categories; competition sits on top as a framing overlay rather than a fourth setting.
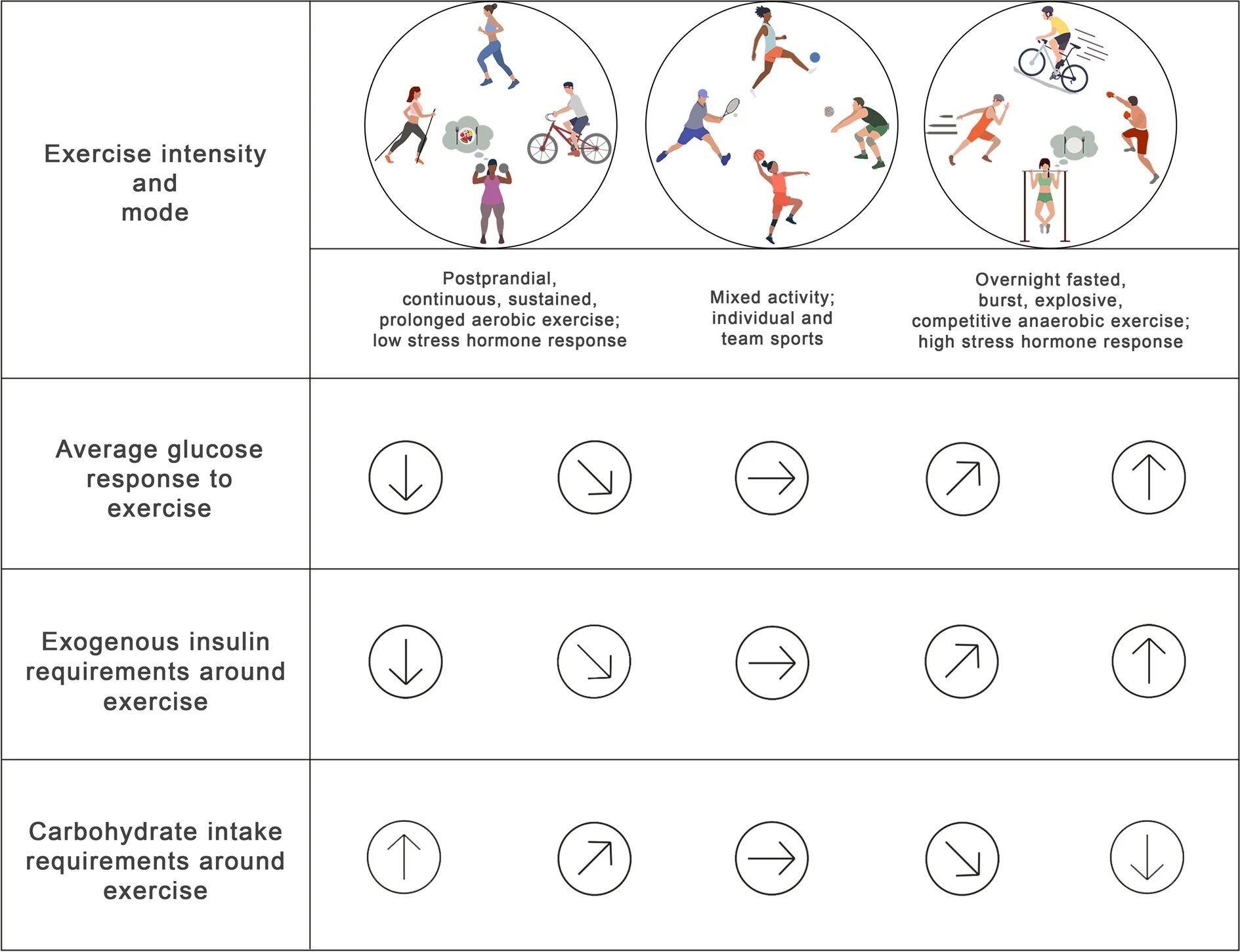
- Endurance / aerobic (steady running, cycling, swimming): tends to lower glucose, sometimes sharply. The classic hypo-risk profile.
- Mixed (team sports, circuits, interval work): a tug-of-war. Aerobic segments pull glucose down; short intense bursts and adrenaline can push it up. The net effect is less predictable.
- Anaerobic (sprints, heavy resistance work, HIIT): adrenaline and hepatic glucose output can drive glucose up during and just after the session, with a delayed fall later.
- Competition: not a separate physiology, but a framing overlay. Adrenaline runs higher, the day is less controllable, and the stakes of a hypo are greater. This is exactly where leaning on the Three-Hour Rule (starting with low insulin on board) earns its keep.
How much the type matters depends heavily on insulin on board. If insulin on board is high, glucose will tend to fall whatever the activity type; the circulating insulin dominates. If you are in basal-only conditions (three or more hours after a meal bolus), the type of exercise then has much more influence, and it is what should shape the plan. An AID algorithm sees only the resulting glucose, not whether the effort was aerobic or anaerobic, so anticipating the type is still your job.
New to this? Do not try to model all of it at once. Start aerobic, start with the Three-Hour Rule where you can, and use 50/50/20 (or T25/T25 on a loop) as your default starting point. Refine from there with your CGM data over weeks, not within a single session.
After the event
The post-exercise window is the harder problem
The session is not where planning ends. Insulin sensitivity stays elevated for hours afterwards, and the one-to-two hour window after exercise, plus the following evening and overnight, is where a lot of exercise hypos actually happen, even when the session itself went smoothly.
This is the second half of both frameworks:
- 50/50/20 (injections or pump): cut the next meal bolus after exercise by about 50 percent, because sensitivity is still high. For exercise in the evening (after about 4 pm), use any one of a 20 percent basal reduction overnight, 20 g of carbohydrate without insulin, or 20 g of protein, to protect against a later or overnight low.
- T25/T25 (closed loop): return the target to normal once the session is done, then cut the next meal bolus by about 25 to 33 percent. The loop keeps helping in the background, which is why the manual cut is smaller.
Two patterns worth knowing: late-afternoon vigorous exercise tends to shift hypo risk into the evening rather than overnight, and long sessions (over about an hour) can leave elevated hypo risk into the following day. Smaller, earlier interventions again beat larger, later corrections.
Ten tactics that hold up in real life
Key tips for exercise
- Treat CGM accuracy during exercise as conditional. CGM is your best learning tool, but it is less accurate during exercise. Read the number alongside the trend arrow and the context, and be slower to react to a single mid-session reading. Iterate over weeks, not within a session.
- Run the three-majors checklist before every session: insulin on board (how much, and when was the last bolus), starting glucose, and trend. Get those right and the rest is refinement, not rescue.
- Sex differences are real and underappreciated. The same session on different days of the menstrual cycle can behave quite differently. That is signal, not noise; tracking it over a few cycles often reveals the pattern.
- Fear of hypoglycaemia is a planning variable. The fear is reasonable; the cost of avoiding exercise is usually larger than the hypo it prevents. A rehearsed hypo response, fast carbs within reach, a plan made with your team, and sensible CGM alarms all lower the cost of starting.
- Barriers and facilitators matter as much as physiology. The right plan is one that fits the rest of your life. The most evidence-based session you cannot actually do is worse than a less optimal one you can repeat for years.
- Altitude changes the rules. The first few days at altitude often need different settings from sea level. Plan altitude trips with your diabetes team rather than improvising on arrival.
- Muscle damage matters for days, not hours. Heavy eccentric or novel work (long downhill runs, new resistance training, certain team sports) can alter insulin sensitivity for two or three days afterwards, not just in the immediate post-exercise window.
- Calibrate to real-world data, not the trial average. Large datasets (T1DEXI and its follow-ons) show hypo risk on exercise days is meaningfully higher than on non-exercise days, and that real-world response is more variable than pivotal trials suggest. The trial average is a starting point, not a forecast for you.
- What the largest GNL-analysed datasets show. Exercise improves time-in-range (modestly, a little more for AID users); the biggest gain from daily steps is between zero and about five thousand steps; strength training appears the safest type for hypo risk; long sessions leave elevated risk into the next day; and on AID, more frequent correction boluses did not raise time-below-range, the automated suspension does its job.
- Know when to ask your care team. This guide is education, not prescription. Bring your team in for recurrent unexplained exercise hypos, post-exercise highs that do not resolve, new exercise types or intensities that shift the pattern, pregnancy, altitude trips, and any change to your insulin regimen or AID system. The point of this guide is to make that conversation a structured one.
Bringing it all together
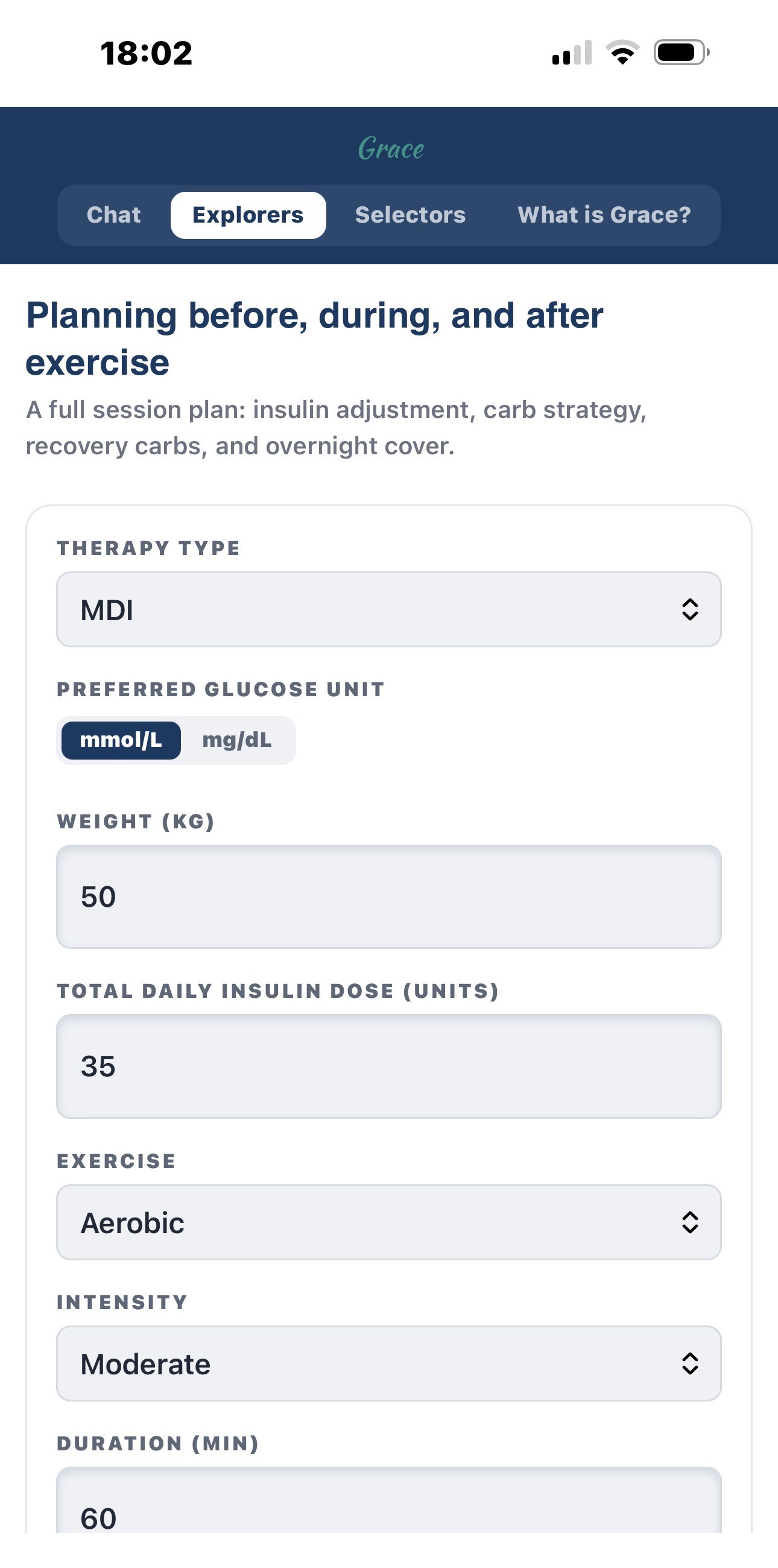
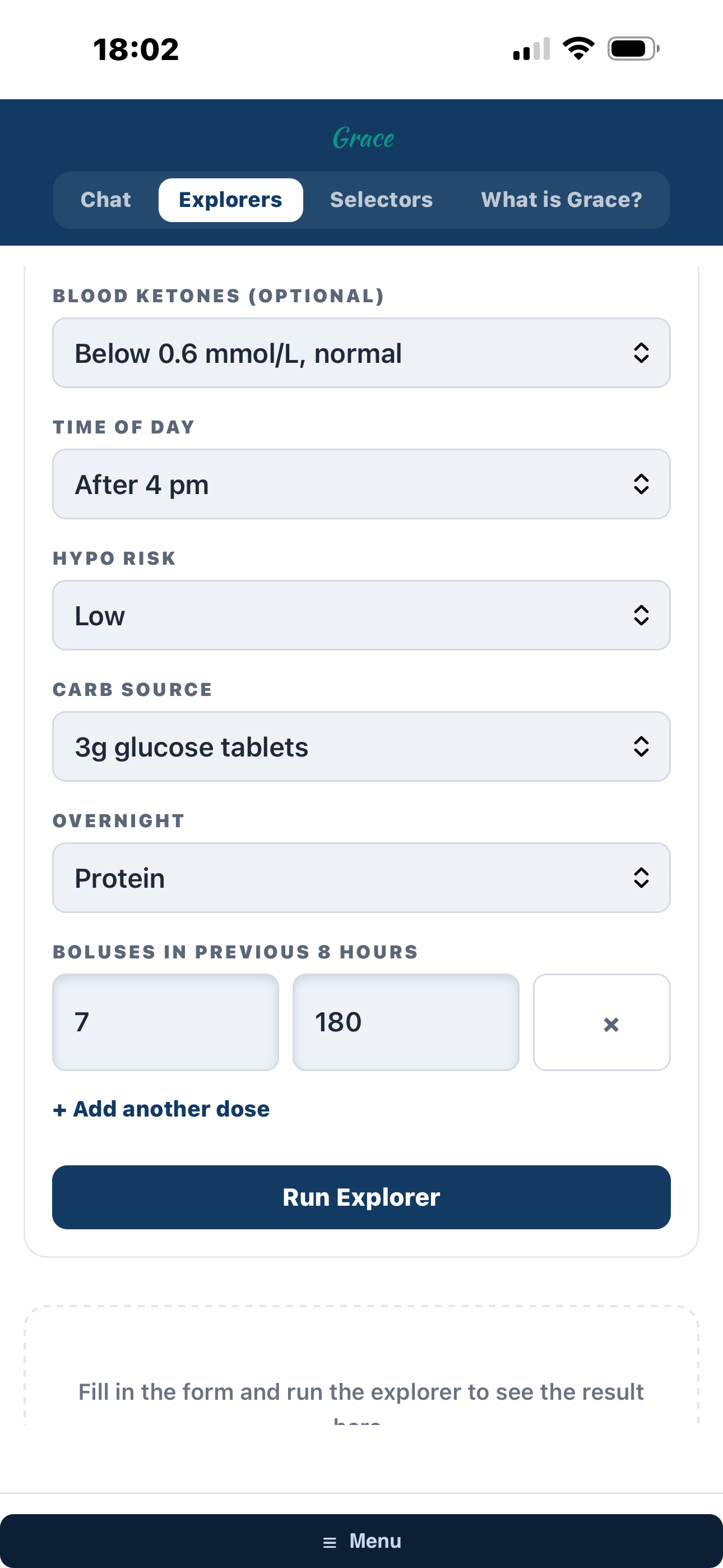
The Exercise Planning Explorer
The Exercise Planning Explorer pulls the whole sequence together in one place: the activity, its timing relative to insulin on board, the meal-bolus reduction, the AID exercise mode or temporary target, and the carbohydrate to have to hand.
Before you start, a short safety checklist
Set up for a safe session
Set your CGM low alert at 5.0 mmol/L
CGM lag lengthens during exercise: the sensor can read meaningfully higher than your true glucose when glucose is falling, and the delay stretches from the usual few minutes to around 12 minutes during prolonged aerobic work. A low alert set at 5.0 mmol/L gives you the headroom to act before you are actually low. If a hypo is suspected mid-session, confirm with a fingerstick rather than trusting the sensor alone.
On an AID system, two ways to set stable conditions
The mainstream default (stay in closed loop): switch on your system’s exercise feature 60 to 90 minutes before you start and leave it running through the session. On Tandem Control-IQ this is Exercise Activity mode (raises the target to 8.9 mmol/L); on MiniMed 780G it is Temp Target (raises the target to 8.3 mmol/L). Both give the algorithm time to reduce insulin on board before you begin, while keeping the automated safety net on.
An advanced alternative for maximal predictability (open loop): some people prefer to come out of auto mode into open loop (manual mode) about two hours before starting, running a constant manual basal rate so insulin delivery is steady and known going into the session. The trade-off is that you lose the algorithm’s automated suspension if glucose drops unexpectedly, so this suits experienced users who want fixed, consistent starting conditions and are monitoring closely. It is an option, not the default.
Have plenty of hypo treatment to hand
Fast-acting carbohydrate within reach is non-negotiable for any structured session. Rehearse the response so it is automatic, not a scramble.
Review and adapt
Treat every session as data. Look back at the CGM trace, note what your starting conditions were, and adjust the next attempt. Exercise with type 1 diabetes is learned over weeks and months of iteration, refined with your diabetes team, not solved in one session.
Exercise and T1D Knowledge Check
Try the assessment on this page any time, before you read the guide or once you have worked through it. It is a quick way to see where exercise and Type 1 still feel uncertain, and 9 out of 10 earns your certificate.
Explorers and tools
Three GNL explorers are built directly on the evidence and algorithms in this guide.
- 10, 20, 30 Minutes Walking to Lower Highs, the activity-snacking tool that pairs with the Activity Snacking guide
- Carbs for 30 Minutes of Exercise, the explorer behind the carbohydrate table above
- Planning for Before, During and After Exercise, the full planning explorer
Further listening and related content
- FAQ, Activity, Exercise and Type 1 Diabetes
- Podcast with Prof Othmar Moser on exercise and T1D
- Episode 33, Exercise, hormones and T1D in females
- The Menstrual Cycle and Type 1 Diabetes, three-part guide
- Foundations, Activity and Movement
- CGM and exercise: bolus reduction and carbohydrate timing
- Fast and slow movers, understanding your individual activity response
- Hypoglycaemia in T1D, understanding and preventing lows
Pairs with the CGM and AID guides
Exercise, CGM and AID are one decision system. If you are planning for all three, start with the guide you have not yet read.