Guide series · Part 1 of 5
How exercise moves glucose
The physiology underneath every other Part. Mechanism, exercise types, the three majors, the 90-minute window, and the Three-Hour Rule.
Part 1 · Anchor thesis
Exercise amplifies insulin action. That is the whole story.
Muscle contraction pulls glucose out of the blood through pathways that are largely insulin-independent. Blood flow rises, insulin already injected or pumped is absorbed faster, and glucose uptake accelerates. The apparent chaos of exercise in type 1 diabetes is not randomness – it is fast physiology meeting slow insulin.
Once you know how the mechanism works, the rest of the guide becomes a set of levers rather than a list of rules. Everything in Parts 2, 3 and 4 traces back to this Part.
Major in the majors
Three variables decide almost everything
Across almost all forms of exercise, glucose behaviour is dominated by three variables, in order of importance.
1 · Most important
Insulin on board
Recent bolus insulin is the dominant driver of exercise hypo risk.
2
Starting glucose
Where you start shapes where you land, especially for aerobic work.
3
Trend arrows
Direction and speed of change. Numbers without direction are incomplete.
The mechanism in plain terms
Working muscle needs fuel. Contracting muscle fibres translocate GLUT4 glucose transporters to the cell surface through calcium- and contraction-driven pathways that do not require insulin. Sylow and colleagues describe this as the dominant pathway of exercise glucose uptake – which is why exercise lowers glucose even in near insulin-deficient states.
At the same time, blood flow to working muscle and skin increases several-fold. Any injected or pumped insulin already in subcutaneous tissue is absorbed faster. The net result is that circulating insulin rises at the moment muscle is most sensitive to it. Exercise does not inject extra insulin – it supercharges the insulin that is already there.
Counter-regulation is real but blunted in T1D
In people without diabetes, liver glucagon release and sympathetic drive push glucose out of storage to match muscle demand. In type 1 diabetes, the alpha-cell glucagon response is blunted (Colberg 2022). This is one of the primary reasons people with T1D are disproportionately vulnerable to exercise-induced hypoglycaemia – counter-regulation is not doing its usual job.
Myokines – muscle as an endocrine organ
Severinsen and Pedersen (2020) review myokines, the proteins released by contracting muscle that act on other tissues. Regular exercise is not only about the glucose curve on the day. It is about the slower, cumulative benefits that follow repeated contraction. This is the non-glycaemic case for activity.
Exercise type explains direction
Different modalities tend to move glucose in different directions. The three majors still decide risk – but exercise type tells you what risk to plan for.
| Type | Typical glucose response | Mechanism |
|---|---|---|
| Aerobic (running, cycling, swimming) | Tends to lower | Sustained muscle glucose uptake dominates |
| Anaerobic (sprinting, heavy lifting) | Often rises | Catecholamine and cortisol release push glucose out of the liver |
| Mixed / team sports | Can rise or fall | Depends on intensity balance and IOB at the start |
The 10-second sprint trick
Bussau et al (2006) showed that a single maximal sprint at the end of moderate exercise triggers enough catecholamine response to blunt the post-exercise glucose decline. This is mechanism translated directly into a practical tool. When aerobic exercise is dropping glucose faster than wanted, a short, very hard effort can lift glucose without requiring carbohydrate.
Iscoe and Riddell showed the same principle holds for brief high-intensity intervals dropped inside continuous moderate exercise.
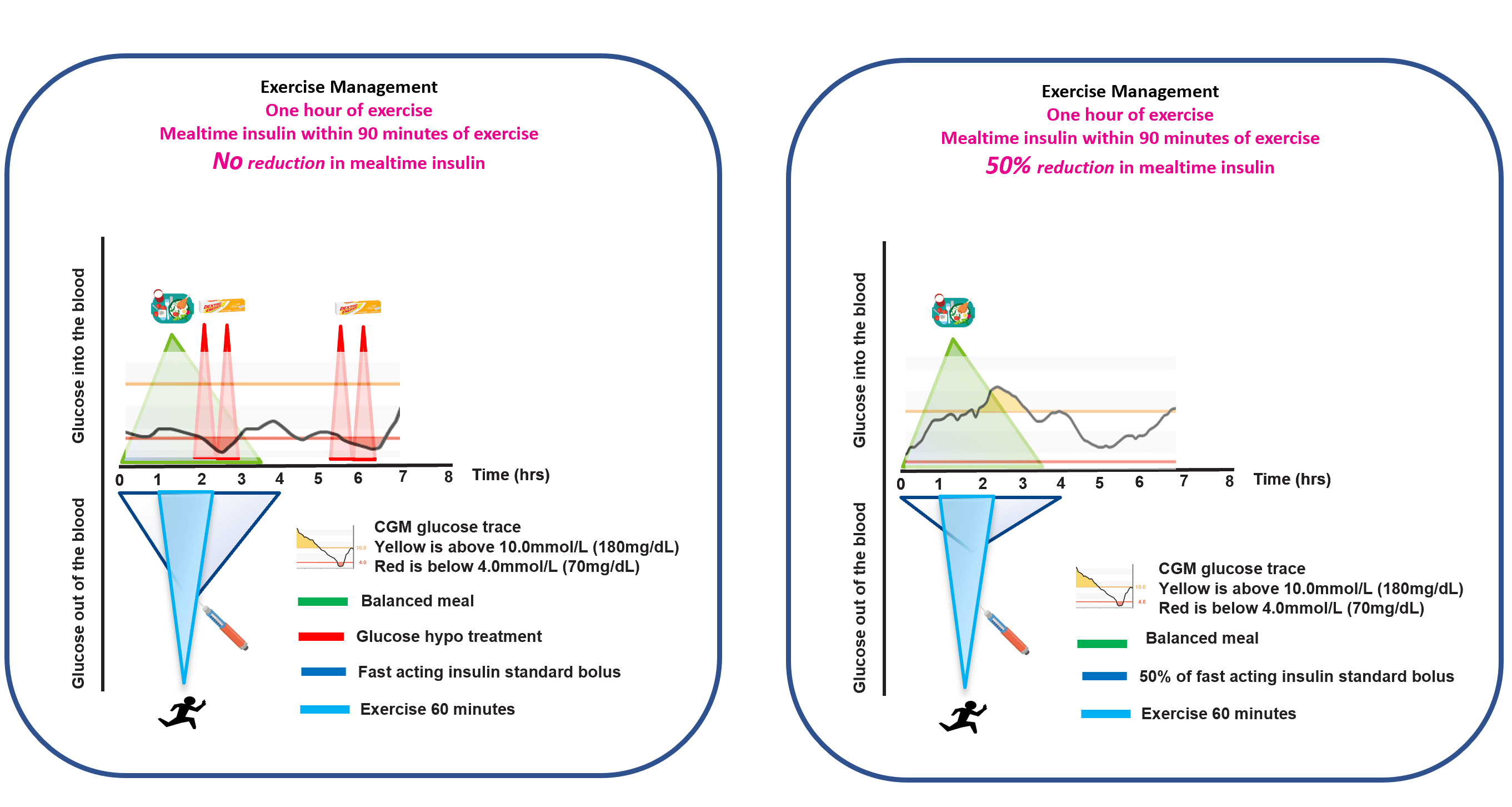
The 90-minute window
When exercise begins within roughly ninety minutes of a meal bolus, insulin action is often near its peak. In this window, rapid-acting analogues are doing their heaviest work and exercise is amplifying every unit of it. This is where the largest, fastest drops tend to happen.
A common starting point is that exercise planned within the 90-minute window after a meal bolus usually needs a bolus reduction. Part 2 covers the 25/50/75% framework that Rabasa-Lhoret, Moser, West and Campbell have developed for this.
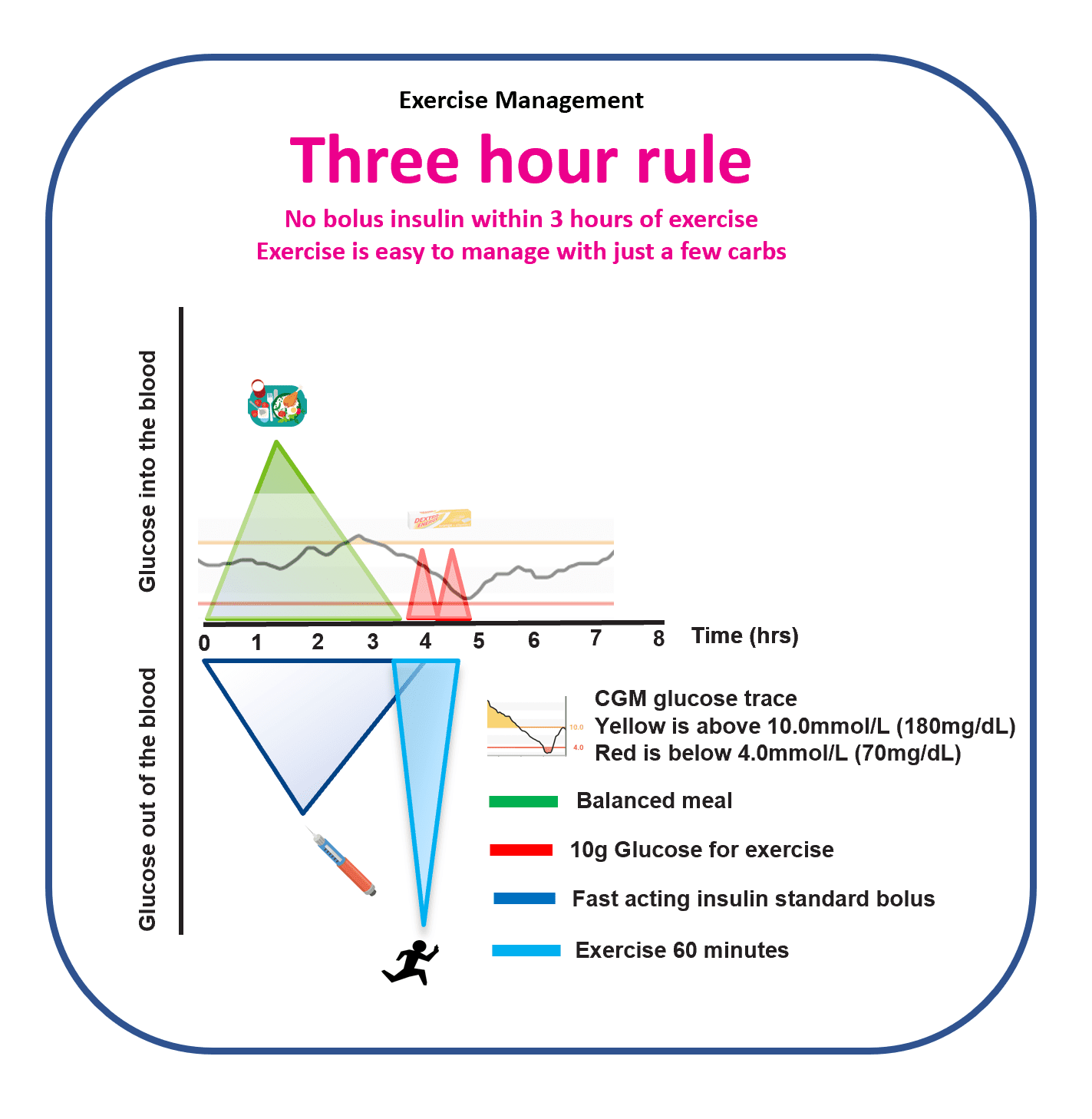
The Three-Hour Rule
One heuristic simplifies exercise management more than almost any other. When the last bolus was at least three hours before exercise, glucose behaviour is often far more predictable. Insulin on board has fallen, peak action has passed, and the exercise effect is less likely to be amplified into a fast drop.
This is not a guarantee. It is an organising principle. Where possible, arranging exercise three hours or more after the last meal bolus tends to reduce hypos, corrections and mental load.
What GNL research shows
The GAME framework
Pemberton et al (2023, Pediatric Diabetes) set out the GAME framework – Glucose, Activity, Meal, Environment – as a way to make exercise decisions in paediatric T1D less reactive and more structured. The framework anchors the majors (IOB, starting glucose, trend) alongside the activity itself, the recent meal, and the context (heat, altitude, sleep). It is the foundation for the Dynamic Glucose Management approach that runs through the GNL explorers and the rest of this guide.
Exercise and CGM
CGM becomes less reliable during exercise. Sensor lag is real, movement artefacts happen, and rapid glucose change stretches the gap between interstitial and capillary glucose. Numbers during and immediately after exercise should be interpreted with a little more caution than usual. Part 5 covers the specific CGM-in-exercise evidence in more detail.
That said, CGM is still the single most useful tool for learning how your body responds to exercise. The goal is not to distrust the number. It is to read it alongside the trend and the context, and to iterate over weeks – not to chase every data point in the moment.
Explorers that pair with this Part
- 10, 20, 30 Minutes Walking to Lower Highs – the activity-snacking tool grounded in the physiology covered here.
- Carbs for 30 Minutes Exercise – operationalises the three majors and the 90-minute window.
- Planning for Before, During and After Exercise – the full planner that pulls all five Parts together.
This guide is educational. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.