
Special note: I did this experiment BEFORE I developed Dynamic Glucose Management.
It’s a bit of a heavy read but has some great insight into carbohydrate intake and type 1 diabetes management.
So, Dani, Grace and Jude, I have brought the conclusion to the top so you do not have to read the rest!
John, what follows after the conclusion is for you!
My top takeaways from this experiment are:
- You need macronutrient consistency if you want good diabetes control for any type of dietary strategy. This is best achieved by creating three meal choices for each mealtime that have consistency in macronutrient (carbs, fat & protein) splits. Make sure these meals cover as many of the nutritional bases as possible e.g. five a day, high in fibre, based on monounsaturated fat etc.
- You need to change your insulin dosing regimen as your carbohydrate intake reduces.
- You need to start considering counting 50% of the protein as carbohydrate intake goes lower than 150g per day.
- You only need to count 25% of protein when carbohydrate intake is less than 50g per day..
- Managing blood glucose during exercise becomes easier as carbohydrate intake reduces. But performance, especially high-intensity exercise suffers.
- If you want to be true KETO as an adult (not good for children!), you need to keep protein to less than 1.5g/kg (0.7g/lb) and increase fat up to 75% of energy intake. If blood ketones are not 0.6-3.0mmol/l, you are not getting the proposed benefit of nutritional ketosis.
- Reducing carbs and increasing fat may change your lipid profile. You need to get a detailed lipid breakdown to understand if it’s a positive or negative change. Ideally, you want to get your Apo-B measured before and after any change.
- It’s energy restriction that drives fat loss, not carbohydrate restriction.
Dani, you can check out here.
John, Let’s begin.
In 2018 I was personally and professionally obsessed with the carbohydrate debate surrounding body composition and diabetes control. Special note:
Professionally, as a Diabetes Dietitian, one question that kept coming up was:
“Should I go low carb? what about KETO?”
Not an easy question to answer. There is a lot of nuance, caveats and I usually ended up saying “it depends”.
But what they really needed to know was:
“What is required on a daily basis to follow diets lower in carbohydrate”?
Some questions that were whirling through my mind:
• Should people with type 1 diabetes go KETO (ketogenic diet), is it safe?
• Is low carb high fat (LCHF) low carb enough to get the same benefit at KETO?
• How will LCHF and KETO impact my physical performance?
• Are LCHF and KETO manageable for a social person?
• How will increasing fat impact my blood lipids?
• What changes to my insulin regimen and daily diabetes habits will I have to make to keep my blood glucose in target?
To answer these questions, I embarked on a 120-day experiment where I manipulated my carbohydrate intake.
My ultimate aims were to drop 10% in body fat, whilst learning the daily strategies needed to manage diabetes with different carbohydrate amounts.
Here is some of the key information you need to know about the 120-day experiment:
- I kept my energy intake constant for the 120-days at 2500kcal per day, a 1000kcal daily deficit. By the end of the experiment, it was probably closer to a 400-600kcal daily deficit due to a reduction in metabolic rate from the lost weight, reduction in NEAT (non-exercise activity Thermogenisis) and hormonal compensation from prolonged energy restriction.
- I kept my daily step count at 10,000 and I tracked my kcal and macronutrient intake via MyFitnessPal.
- I kept my exercise regimen consistent for the 120 days.
- 4 x 60 minute gym sessions: 2 x Strength, 2 x Bodybuilding.
- 2 x 45-minute HITT/circuit style sessions – specifically for cricket
- I used a Medtronic Insulin Pump and Enlite Sensor and tracked all the data.
- I followed three different dietary regimens for 40 days each (see the table below for a full breakdown). I kept protein constant at 1.9kg/d for all three dietary regimens.
o Days 0-40: High Carbohydrate Low Fat (HCLF) – usually defined as carbs at 50% or higher and fat at 20% or lower.
o Days 40-80: Low Carbohydrate High Fat (LCHF). Usually defined as carbohydrate intake of 50-150g per day.
o Days 80-120: Ketogenic Style Diet (KETO) – usually defined as carbohydrate less than 50g per day. The amount of protein allowed is hotly debated. I cover this in detail in the blood ketone level section. You will discover the majority of dietary regimens and people who think they are KETO, have blood ketones well below the needed 0.6-3.0mmol/l.
Nutritional breakdown and Lifestyle Parameters
| Usual diet before experiment | HCLF 40 days | LCHF 40 days | KETO 40 days | |
| Average daily carbohydrate intake (g) | 350g (3.6g/kg) | 345g (3.5g/kg) | 131g (1.4g/kg) | 16g (0.2g/kg) |
| % total energy from carbohydrate | 44% | 50% | 20% | 3% |
| Average daily fat intake (g) | 140g (1.5g/kg) | 55g (3.5g/kg) | 140g (1.5g/kg) | 186g (2.0g/kg) |
| % total energy from fat | 35% | 20% | 50% | 67% |
| Average daily protein intake (g) | 185g (1.9g/kg) | 185g (1.9g/kg) | 185g (1.9g/kg) | 185g (1.9g/kg) |
| % total energy from protein | 21% | 30% | 30% | 30% |
| Daily energy intake | 3,500kcal | 2,500kcal | 2,500kcal | 2,500kcal |
| Supplements | Creatine 3g/d Multi-vit& min 1xd Caffeine 400mg/g Whey Protein 90% | Creatine 3g/d Multi-vit& min 1xd Caffeine 400mg/g Whey Protein 90% | Creatine 3g/d Multi-vit& min 1xd Caffeine 400mg/g Whey Protein 90% | Creatine 3g/d Multi-vit& min 1xd Caffeine 400mg/g Whey Protein 90% Slo-Mag (300mg Mg, 500mg Ca) Potassium 2g/d Sodium 2g/d |
| Average hours sleep per night | 7.5 hours | 7.5 hours | 7.5 hours | 7.5 hours |
| Average time exercising per week | 300 minutes | 300 minutes | 300 minutes | 300 minutes |
I wanted to see what would happen over the 120 days to my:
- Diabetes control and insulin requirements.
- Insulin regimen, daily diabetes management, how did I feel on the diet.
- Blood Ketone levels.
- Metabolic markers.
- Body Composition.
- Exercise Performance.
Diabetes control and insulin requirements
I kept a close eye on my diabetes results and insulin requirements during the 120 days. This table and the below download graphs present the key information.
| Before change | After HCLF 0-40 days | After LCHF 40-80 days | After KETO 80-120 days | |
| Predicted HbA1c% from sensor glucose readings | 6.5% | 6.3% | 5.1% | 5.5% |
| Average blood glucose (mmol/l) | 8.5mmol/ | 8.0mmol/l | 6.2mmol/l | 6.1mmol/l |
| Standard Deviation | 3.5mmol/l | 3.1mmol/l | 1.8mmol/l | 1.3mmol/l |
| Number of hypos (<3.5mmol/l) each week | 5 | 4 | 2 | 1 |
| Total daily insulin (TDD) (units) | 45units | 38 units | 25 units | 18 units |
| Total daily basal insulin (units& %TDD) | 18units (40%) | 15 units (39%) | 15.5units (62%) | 11 units (61%) |
| Total daily bolus insulin (units& % TDD) | 27units (60%) | 23 units (61%) | 9.5 units (38%) | 7 units (39%) |
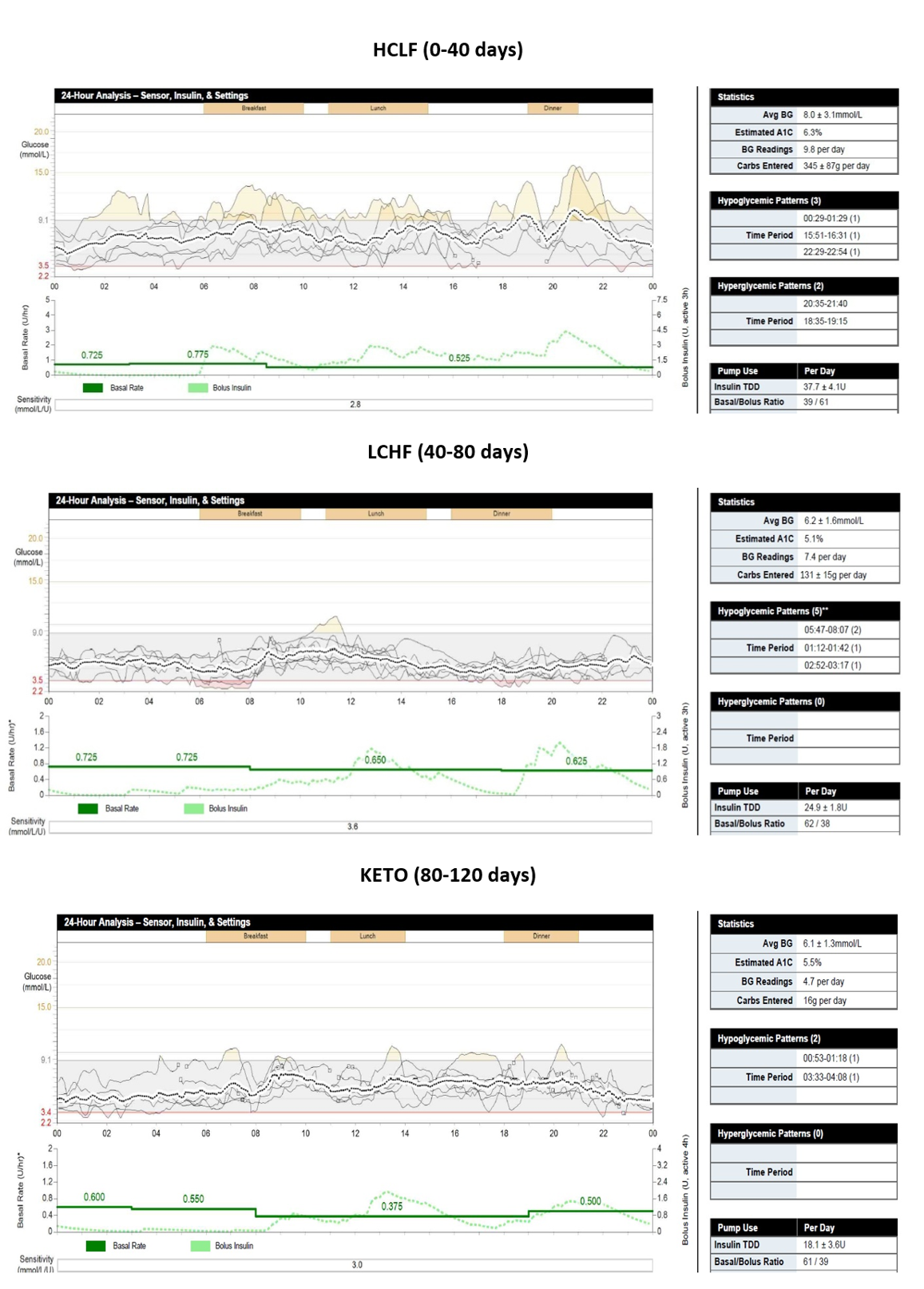
The results and downloads above show:
The experiment clearly shows as I lowered the carbohydrate, my blood glucose was much easier to manage. This was mainly due to never having a high amount of bolus insulin in my system at any one time. The lower the bolus insulin in your system, the less chance of a quick drop in glucose. Also, the less carbohydrate ate, the less chance of spikes in blood glucose.
Put simply, smaller inputs, smaller outputs!
Interestingly, I enjoyed the majority of the benefit in blood glucose control by dropping from 345g a day to 131g a day. There was only a slight further benefit in diabetes control by dropping from 131g to 16g a day.
How did I insulin dose for the different macro splits of the diets?
Insulin dosing for the different diet types created a unique challenge. One thing is for sure, carbohydrate counting alone did not work for the different macronutrient splits.
Taking a deep dive into the research and science is beyond the scope of this write-up. That information can be found in the Ultimate Guide to Insulin Dosing. The graph below is taken from the insulin dosing guide. It presents a summary of the research on the insulin and glucagon response to different macronutrients splits.
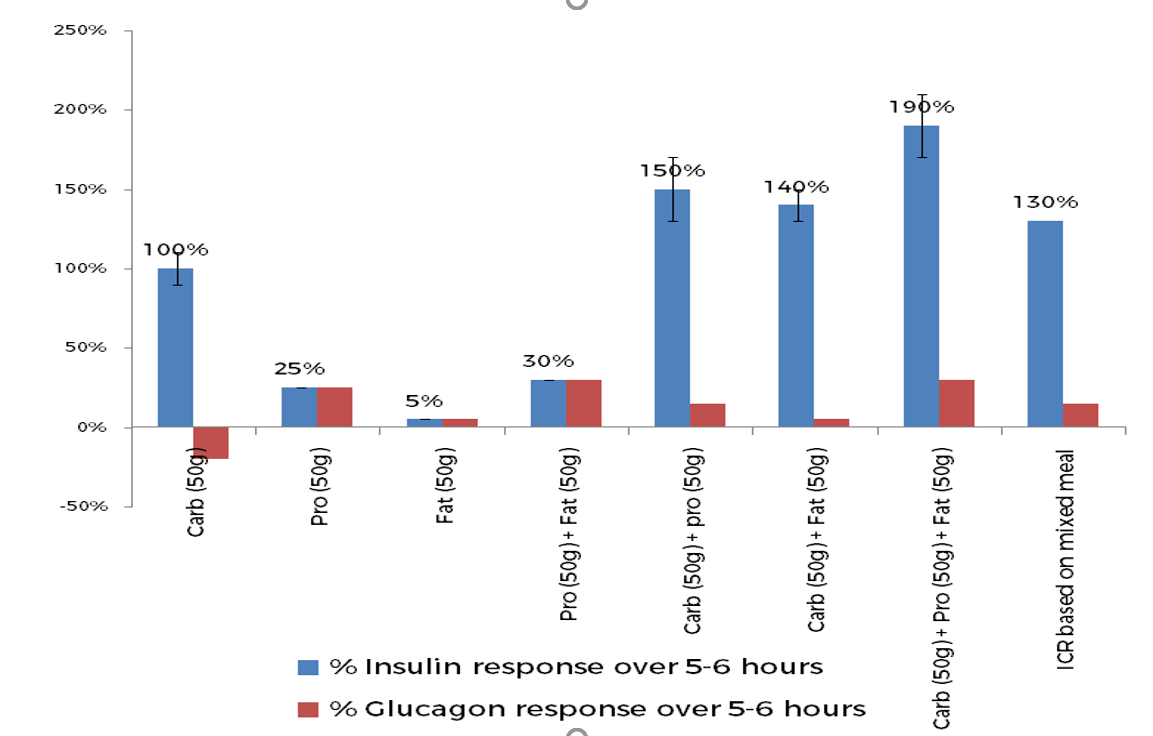
The key things to understand from this graph are:
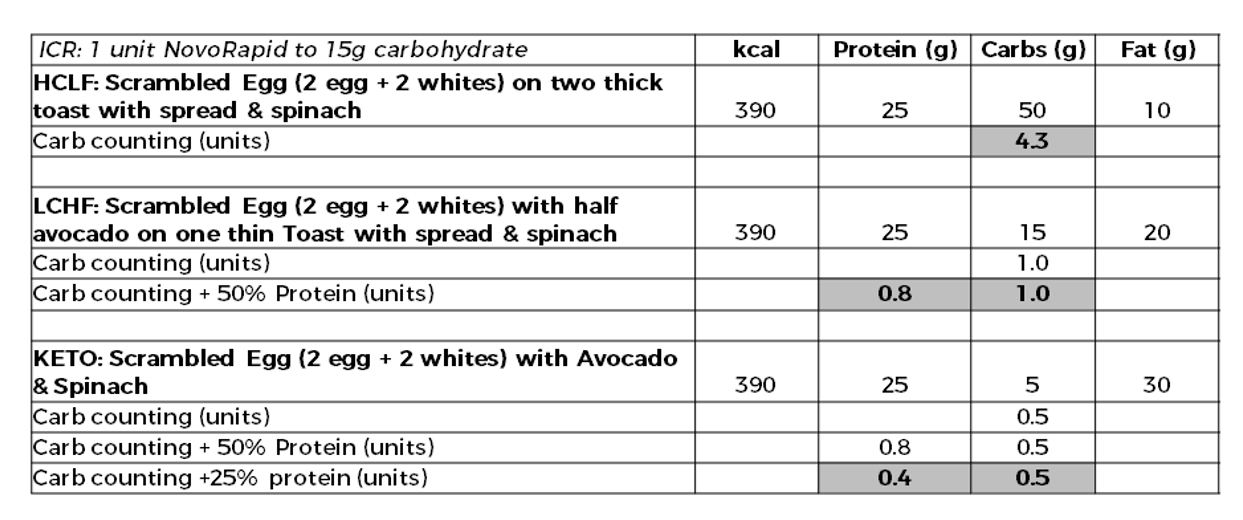
To bring this into real-life, see the HCLF, LCHF, and KETO breakfasts below.
The grey shaded areas show the strategies that are backed by science depending on the diet type you choose. They certainly worked well for me during the 120 days. More importantly, they now allow me to have ultimate flexibility from day to day. I can switch from HCLF to LCHF to KETO when needed, without an impact on my glucose control.
But if you are keeping to one insulin dosing method you should take away one BIG thing:
To achieve in target glucose control after meals, you need the three C’s when it comes to macronutrient profile:
Consistency
Consistency
Consistency
Insulin regimen, daily diabetes management and how I felt.
HCLF – first 40 days:
The meal plans
- No forbidden foods, this was great for flexibility. It was nice to be able to have the occasional bit of chocolate, ice-cream and other junk, as long as within 2,500kcal.
- This diet required the greatest amount of discipline to prevent overeating. With no strict rules in place to forbid foods, it required a lot of conscious effort to keep to a kcal restriction. Most humans do not do moderation well, I am no different.
- To keep my glucose levels in target, I had to specifically engineer every meal to be 45-55% carbohydrate, 30-35% protein, 15-25% fat. I created three go-to meals for each meal time, this kept decision fatigue down! This also meant when I applied my insulin to carbohydrate ratio it worked consistently well.
- For example, a meal of 50g carbs, 30g protein, 15g fat was easily managed by just counting the carbs, applying my 1u:15g ratio and giving 3.3 units.
- If I changed the macro profile to say 80% carbohydrate, 10% protein, 10% fat I would go hypo.
- For example, a meal of 80g carbs, 15g protein, 5g fat meant an insulin dose of 5.3units (1u:15g) – which led to hypo as was too much insulin for the meal.
- If I changed the macro profile of a meal to 30% carbohydrate, 50% protein, 20% fat I would go high.
- For example, a meal of 30g carbs, 50g protein, 10g fat meant an insulin dose of 2.0units (1u:15g) – which led to high readings as not enough insulin for the meal.
- This is because your insulin to carb ratio covers your usual protein and fat of meals, and if you change them significantly, it no longer works.
- I had to be on point with my diabetes behaviours to get tight post-meal glucose control. Things that became essential for me were:
- Bolus 20-30 minutes before meals
- Use a Super Bolus at most meals (I am on a pump)
- 10- 20 min walk after eating to insulin sensitize quicker.
- Had to do corrections between meals reasonably often due to slight carb counting errors, or unsure of exact carb amounts when eating out (This was before I started Dynamic Glucose Management, if only I had discovered short bursts of exercise)
- Had to make sure my food environment was a low-fat one, to help keep to 2,500kcal and 20% fat.
- Did not require any supplements above my usual stack already shown in the table.
- Bowles worked well, felt good the majority of the time, but did get the occasional bit of water retention in the abs area – but this is very subjective. Got a good pump in the gym, and psychologically this gave me a nice boost!
The Exercise
- I had to make sure I had my meals at least three hours prior to training so there was little active insulin on board. Having lots of bolus insulin on board makes the blood glucose response to exercise much more erratic.
- I had to apply significant changes to bolus amounts before and after exercise to prevent hypos and hypers.
- Great for cricket teas because they are always high carb. Having good glycogen stores gave me the quick burst of energy needed when fielding.
The Social Impact
- Easy to manage social occasions as no forbidden foods, I just had to adjust other meals to keep to the fat and kcal restriction.
LCHF – 40-80 days:
The meal plans
- I implemented a blanket rule of no starchy foods (bread, rice, pasta, noodles, crackers, cereals, etc). I got my carbs from fruit, dairy, and starchy vegetables such as peas, sweetcorn and squash. It was amazing how quickly you can rack up 100-150g per day of carbs just from these alone.
- I had to banish things such as chocolate and ice-cream, which was a challenge in social situations.
- Having set of foods restrictions made it easy to follow. My brain works well with black and white rules.
- Keeping my meal macronutrient consistency was much easier than a low fat approach. The vast majority of meals comprised of a big portion of meat, some vegetables or salad, added olive oil, and finished with a bit of fruit. This almost always worked out 30-35% protein, 50% fat and 15-25% carbohydrate. I designed three meals for each meal time that were kcal controlled and macro consistent.
- I had to count 50% of the protein for my insulin doses otherwise I would not cover the effect of protein that was usually covered by a high carb amount on HCLF.
- For example, a meal of 20g carbs, 30g protein, 25g fat meant an insulin dose of only 1.3units (1u:15g) for the carbs – which led to high readings. So by counting 50% of protein, I had the 1.3units for the carbs and 1.0unit for the protein (counted 50% so 15g). So a total of 2.3 units. Counting 50% of protein was needed for good control.
- I could be much more relaxed with diabetes behaviours
- I could often get away with not giving insulin 20 mins before meals.
- Never needed a 20 min walk.
- Rarely had to do corrections between meals.
- Making sure my shopping was on point was very important, a ‘no starches or junk food’ policy was implemented.
- Did not require any vitamin or mineral supplements above my usual stack.
- Bowles worked well, felt good the majority of the time, and liked the tight feel on my abs of little perceived water retention – but this is very subjective. Only ever go an average pump in the gym, so not as impressive to look at in the mirror (we are all vein).
The Exercise
- Exercise management was less intensive as there was never as much active insulin around, so the three hour rule was not as vital to adhere to.
- Cricket teas were a challenge, not much LCHF on offer.
- Towards the end of HITT sessions I started to drop off. I did not feel I had the glycogen stores to push through at the end.
The Social Impact
- Was manageable at social occasions, just went for the salad style options and went for cheese and grapes for the dessert.
- I could get the food I wanted from most places without a lot of looking. No real dramas.
KETO – 80-120 days:
The meal plans
- These were simple to make and very easy to follow because the list of banned foods meant my choice was very restricted. No starches, no fruit, no yoghurt, no “junk”, no starchy vegetables.
- Having an extremely limiting set of food rules made it easy to keep to 2,500kcal. In fact I struggled to eat that amount due to the very limited selection of food I could eat. This is usually the reason most people have success with this type of diet. It’s simple to follow and hard to overeat, unless you fall for the marketing of fat bomb coffees that is!
- Keeping my meal macronutrient consistency was so easy because the limited food options just fell perfectly into the macros of 30-35% protein, 60-70% fat, and 5% carbs. Every meal was a big portion of meat, some non-starchy vegetables and salad, lots of added olive oil, and some kind of artificially sweetened fat based dessert. I designed myself three meals for each meal time that were kcal controlled and macro consistent.
- Insulin doses at meal times were very small. I only had to count 25% of the protein and apply my ratio. When protein is eaten in the absence of carbs it does not require the same amount of insulin.
- For example, a meal of 5g carbs, 30g protein, 35g fat meant an insulin dose of only 5g for carbs, 7.5g (25% of protein) =12.5g = 0.8 units (1u:15g ratio).
- My meal time management was super easy.
- I sometimes had to give insulin just after I had eaten to stop myself going hypo.
- Never needed a walk after eating.
- Never needed to think about corrections in between meals.
- Had to make sure my food cupboards were stocked with the meat, low carb veg, and plenty of olive oil and macadamia nuts.
- Required lots extra electrolytes to prevent deficiency and the so called “KETO FLU” when drop carbohydrate down to very little! See the nutrition table for the magnesium, potassium, sodium, and calcium intake. If you are considering a KETO approach, you must do your homework before starting, or get some professional advice!
- Had some slight constipation due to reduction of fibre and slight dehydration. Felt good the majority of the time, and really liked the very tight feel on my abs, not a hint of water anywhere. Also by this point I was lean so showing off the 6-pack at every chance! You would too right?Never got a pump in the gym, which I did not like at all! Vein but true!
The Exercise
- Exercise management was very easy as there was hardly ever any active insulin from previous meals.
- My metabolism changed to burn more fat than glucose for fuel, so there was a lower requirement for supplemental carbohydrate during exercise. Remember, I was eating a lot more fat, so the extra fat burned was not from sub-cutaneous fat, it was from the fat I was eating!
- Cricket teas were impossible!
- The HITT sessions were so tough! My usual hardcore sessions were down to a labored grind.
The Social Impact
- Was very tough eating out, always going for the salads with extra olive oil, followed by cheese only for dessert.
- I had to take food with me everywhere as most eating places do not cater for this type of macro split.
KETO and blood ketone measurements:
Although the last 40 days were called KETO, it is actually misleading. I measured my blood ketone levels every day,they never went above 0.2mmol/l. Only when I dropped my protein intake from 1.9g/kg to 1.0-1.2g/kg(100-120g) did I get ketones in the nutritional ketosis range of 0.6-3.0mmol/l.
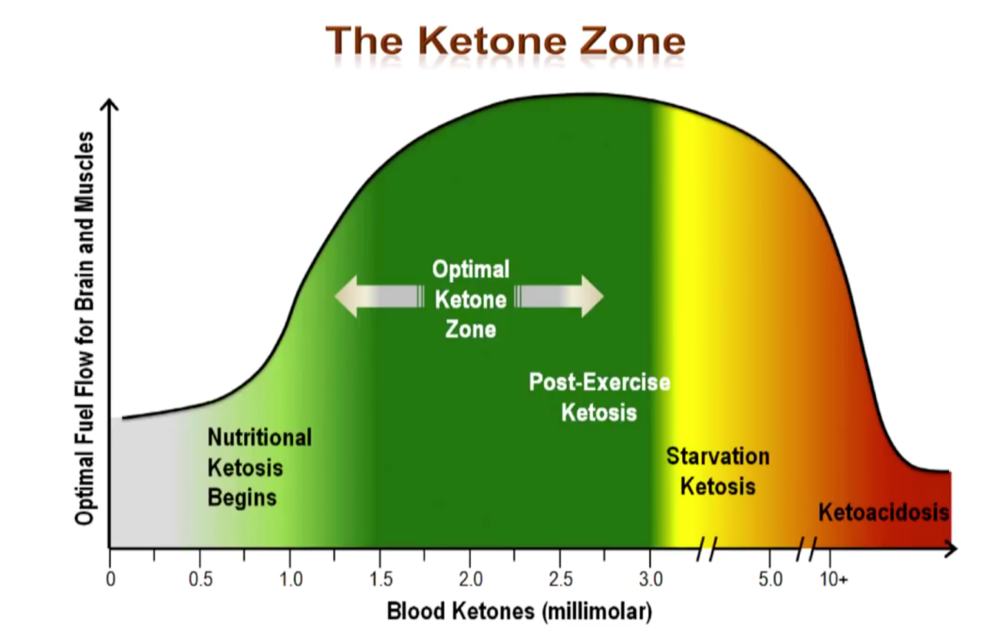
The suggested benefits of having blood ketones levels of 0.6 – 3.0mmol/l are:
- Reduced hunger.
- Anti-inflammatory effect in the brain by using ketones rather than glucose as fuel.
- Providing the brain with 30% of its fuel, therefore, increasing cognitive sharpness.
- Plus much more.
Ketones are only made in the liver and kidneys, so for the brain to be getting a consistent supply, the blood levels should be consistently 0.6-3.0mmol/l. I was not getting any of this proposed benefit.
There is one main reason why my ketone levels were not getting 0.6-3.0mmol/l. But first we need to look at how a healthy pancreas operates.
Amino acids from protein digestion cause the alpha-cells in the pancreas to release glucagon. To prevent too much glucagon from being released and liberating glucose from the liver, the “healthy” pancreas also releases insulin from the beta-cells in response to protein ingestion. The insulindirectly inhibits the alpha-cells from releasing too muchglucagon. This works effectively for people with a healthy pancreas if protein intake is kept to a limit of:
- For non-active people: 1.2g/kg (0.5g/lb)
- For very active people 2.0g/kg (0.9g/lb)
If protein intake goes above this, Glucagon is released in large amounts and more insulin is released from the beta-cells. The high level of insulin makes it way to the liver and kidneys where it turns off ketone production. Therefore if protein intake is too high, nutritional ketosis of 0.6-3.0mmol/l is not possible, and the proposed benefits cannot be enjoyed.
This issue is even more challenging for the person with Type 1 diabetes. This is because the person with type 1 diabetes infuses insulin into the peripheral tissues, it is not secreted directly from the beta-cells of the pancreas. This means the direct inhibition of glucagon releasefrom the alpha-cells is not as effective. Therefore, an even higher insulin level is needed to achieve the same result of stopping liver glycogen liberation. This higher level of circulating insulin is even more effective at stopping the liver and kidneys producing ketones.
Therefore, the protein level cut offs need to be lower for people with type 1 diabetes wanting to achieve nutritional ketosis, blood ketones of 0.6-3.0mmol/l, are:
- For non-active people: 0.8-1.0g/kg (0.3-4g/lb)
- For very active people 1.2-1.5g/kg (0.5-.7g/lb)
The diagram summarizes this:
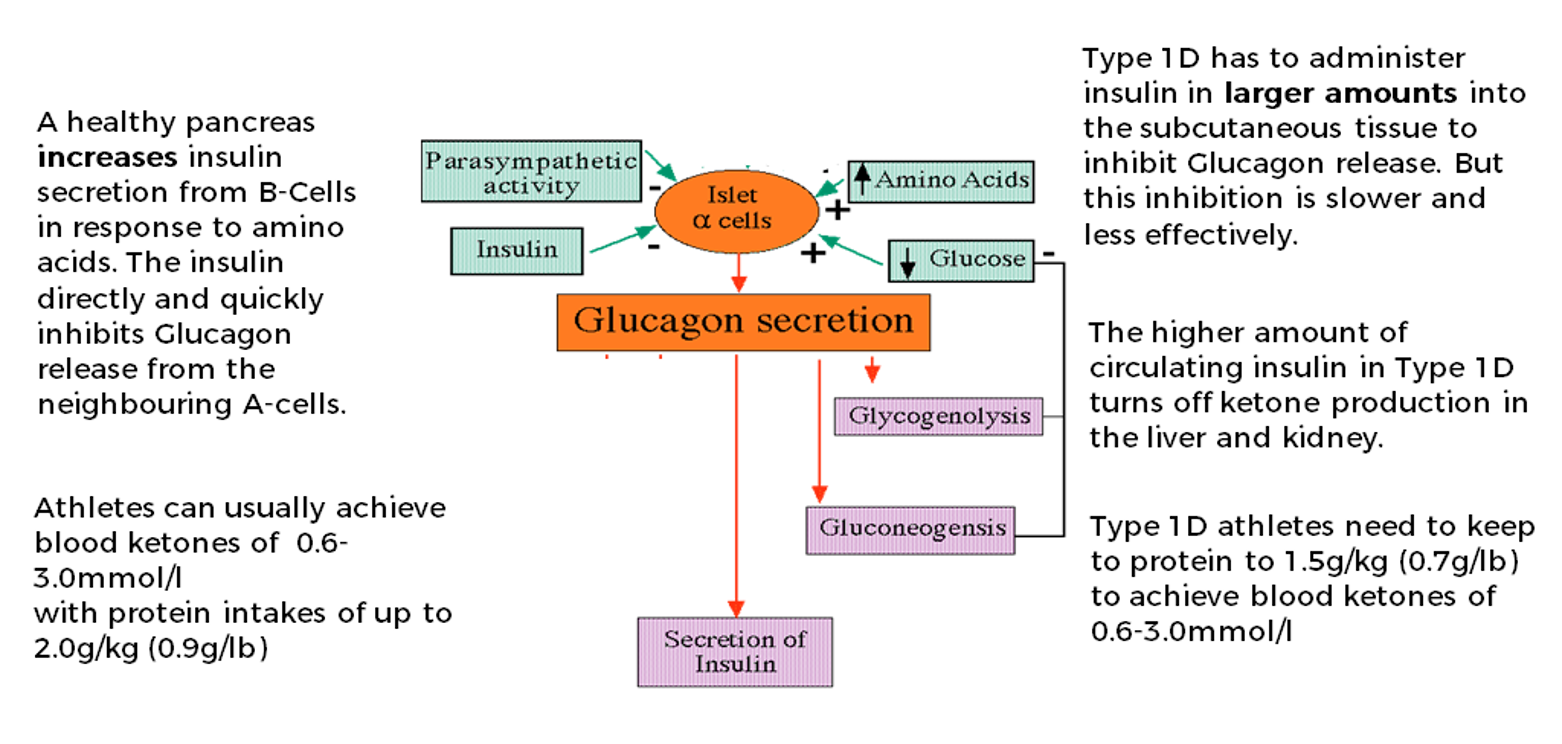
So in simple terms, if a person with type 1 diabetes wants to get into nutritional ketosis, they need a lower protein intake and higher fat intake. This may not be ideal for maintaining lean muscle mass in an energy-restricted phase.
The above is the reason I smile when I see nutritional regimens or programs being sold as KETO. If they have a protein recommendation of more than 2.0g/kg (0.9g/lb), blood ketones of 0.6-3.0mmol/l will not be achieved by the vast majority. They will certainly not for anyone with type 1 diabetes.
Will these type regimens work for weight loss?
YES, because it’s a high protein low carb energy-restricted diet that’s been proven to work since year dot. Marketing it as KETO is very clever (I salute the business acumen) because it’s on trend, but it’s not actually KETO for the vast majority of people. The diet will not lead to blood ketones of 0.6-3.0mmol/l. This makes it very confusing to the people following.
Bottom line is, if you want a true ketogenic diet that gets blood ketones of 0.6-3.0mmol/l consistently. You would need to keep protein at less than 1.5g/kg (0.7g/lb) and have a fat intake that is at least 75% of total energy intake. You also need to test your blood ketones!
Is Nutritional Ketosis ok for Children?
No. The research on children who follow a truly ketogenic diet, getting blood ketones of 0.6-3.0, shows impaired growth and awful blood lipids. Read more in the Ultimate Guide to Insulin dosing.
Metabolic markers
The table below shows the changes in metabolic markers across the 120 days. My blood pressure dropped progressively and finished in the optimal range, which is what would be expected with improved body composition. The blood lipid profile is a confusing situation:
| Before | After HCLF 0-40 days | After LCHF 40-80 days | After KETO 80-120 days | |
| Blood pressure (systolic/diastolic) | 140/80 | 135/75 | 130/70 | 123/70 |
| Triglycerides (TG) Ideal <1.7mmol/l | 1.3mmol/l | 1.0mmol/l | 1.0mmol/l | 1.0mmol/l |
| Total cholesterol (TC) Ideal <5.0mmol/l | 5.9mmol/l | 4.8mmol/l | 7.3mmol/l | 8.6mmol/l |
| Low Density Lipoprotein (LDL) Ideal<3.0mmol/l | 4.1mmol/l | 3.2mmol/l | 4.6mmol/l | 5.4mmol/l |
| High Density Lipoprotein (HDL) Ideal>1.0mmol/l | 1.3mmol/l | 1.5mmol/l | 2.2mmol/l | 2.7mmol/l |
| TC:HDL (Risk: low <3.5, medium 0.5, high >0.7) | 4.5 Medium | 3.2 Low | 3.3 Low | 3.2 Low |
| HDL:LDL (Risk: low >0.4, medium 0.3, high <0.2) | 0.3 Medium | 0.4 Low | 0.47 Low | 0.5 Low |
| TG:HDL (Risk: low <0.87, medium 1.74, high >2.62) | 0.77 Low | 0.66 Low | 0.45 Low | 0.37 Low |
The highlights from the lipid results:
- The positive changes in lipid profile:
- TG remained stable and at low risk level.
- HDL increased progressively with energy restriction and body fat loss.
- There was a big increase in HDL when carbohydrate decreased, which is in line with the evidence showing insulin reduces HDL production by the liver.
- All the risk ratios (TC:HDL, HDL:LDL,TG:HDL) improved as energy was restricted and body fat lost.
- TG:HDL reduced significantly with energy restriction and fat loss. TG:HDL has been shown to be the strongest predictor of coronary heart disease in large cohort studies (3,4).
- The concerns:
- TC at 5.9mmol/l before the experiment. My paternal grandad died of cardiovascular disease and my dad had a recent TC of 9.0mmol/l. So there are some genetic elements at play here (I was later diagnosed with Familial Hypercholesterolemia, and now take Rosuvastatin 10mg per day)! TC did drop with weight loss and energy restriction in the first 40 days of HCLF. Then increased as carbohydrate decreased and fat increased to a potentially concerning 8.6mmol/l by day 120.
- LDL cholesterol increased consistently as carbohydrate intake decreased and fat increased. (This may be due to me having Familial hypercholesterolemia even though I did not know it at the time.)
Exercise Performance
I kept track of a few performance indicators in the table below. I was certainly not breaking any weightlifting records, but the measurements allowed observation of the effects of lowering carbohydrate on my performance.
| Before change | After HCLF 0-40 days | After LCHF 40-80 days | After KETO 80-120 days | |
| Back squat x 8 Reps | 140kg | 140kg | 135kg | 130kg |
| Dumbbell Chest Press x 8 Reps | 100kg | 100kg | 95kg | 90kg |
| Pull ups – strict form | 12 | 11 | 10 | 9 |
| HITT Session Using before experiment performance as 100% | 100% | 95% | 85% | 70% |
Highlights and discussion:
- A progressive drop in strength across the dieting phase. This is to be expected with prolonged dietary restriction. Nothing concerning me here. But I did feel the drop in carbohydrate when following KETO in the third and fourth sets of compound lifts, such as deadlifts and squats. I felt completely gassed with nothing in the tank. Not a feeling I enjoyed, at all!
- The High Intensity Interval Training (HIIT) is where the most interesting results were seen. By the end of the 120-days, I could only complete 70% of my usual work. Some of this will have been due to prolonged dieting, and some of this may have been due to the lack of glycogen storage in my muscle to create the quick energy needed. The only way to know for sure would be to re-run the experiment and do KETO first, the LCHF, the HCLF. If my performance was greater than 70% at the end, then it would be clear for me that the carbohydrate was a major factor. If I had to state what I believe, it would be the lower carb almost certainly impacted way above just energy restriction alone. But I could be biased.
- It was also my cricket season during the LCHF and KETO periods. During the LCHF 40 days I felt ok in the field for three hours, but when I dropped to KETO, I felt very lethargic and it seriously impacted my performance. Some of this will have been due to prolonged energy restriction, but in my opinion again, it was mainly due to carbohydrate restriction.
Body composition
| Before change | After HCLF 0-40 days | After LCHF 40-80 days | After KETO 80-120 days | |
| Weight (kg) Average morning weight from at least 3 measurements | 100kg | 97kg | 95.5kg | 91.8kg |
| Body fat from 7-site Skin Callipers in mm &percentage drop from previous 40 days (%) | 98 | 72 (27%) | 50 (30%) | 37 (26%) |
| Body Fat % – estimated from 7 site calliper measurements | 15% | 11% | 8% | 5.7% |
| Fat mass (kg) & percentage drop from previous 40 days (%) | 15kg | 11kg (27%) | 8kg (28%) | 5.4kg (33%) |
| Fat Free Mass (kg) | 85kg | 86kg | 87.5kg | 86.4kg |
| Waist circumference(cm)& percentage drop from previous 40 days (%) | 98cm | 92cm (7%) | 86cm (7%) | 84cm (3%) |
Some of the highlights from the results above:
- There was a progressive loss in body fat across the 120 days.
- The absolute rate of fat loss in total mm did slow over the 120 days. I lost 28mm in the first 40 days and only 13mm in the last 40. This was expected as the starting kcal deficit was 1000kcal, and by the and probably closer to 500kcal. But the relative percentage of total fat in mm lost remained constant over the 40 days periods at 25-30%.
- The pattern shown for bodyfat in mm loss was mirrored in absolute amounts, and relative percentage loss compared to previous 40 days, for:
- Body fat %, moving from 15% to 5.7% over the 120 days.
- Absolute fat mass in kg, dropping from 15kg to 4.8kg.
- Waist circumference in cm, slimming from 98cm to 84cm
- Fat free mass remained relatively constant over the 120 days. This shows the importance of resistance training for maintaining muscle mass when in a prolonged energy deficit.
Reviewing the body composition results solidified a few key principles:
- Energy balance is the most important element when it comes to body composition change. In the first 40 days the rate of fat mass loss was constant at 1% (1kg or 2.2lb) every 10 days. The rate of fat loss slowed slightly during the next 80 days. This was most likely due to me not making adjustments to the energy restriction as weight was lost, to keep it at 1000kcal deficit. After the experiment I factored in the metabolic rate and NEAT reduction to show I was only achieving about a 500kcal per day deficit by the end of the 120 days.
- It does not matter if it’s low carb, high carb, KETO or anything else. If you consistently achieve an energy deficit, you will lose fat! There is no metabolic advantage of low carb. This has been proven time and again in laboratories, for example in Kevin Hall’s metabolic ward studies of KETO vs. high carb (2). If you need more convincing go and review all the important evidence in the ISSN body composition consensus statement (3).
- Be clear, energy restriction is the driver of body composition change, not macronutrient breakdown! How easy the energy restriction is to keep for different diet types to is another matter entirely. Keeping to a restriction depends on a person’s psychology, response to restriction, taste preferences, peer groups, food environment and much more.
Conclusion: Final thoughts
My top takeaways from this experiment are:
- You need macronutrient consistency if you want good diabetes control for any type of dietary strategy. This is best achieved by creating three meal choices for each meal time that have consistency in macronutrient splits. Make sure these meals cover as many of the nutritional bases as possible e.g. five a day, high in fibre, based on monounsaturated fat etc. If you cannot create these due to time, skill, or knowledge, consideroutsourcing to someone with the skill and time.
- You need to change your insulin dosing regimen as your carbohydrate intake reduces.
- You need to start considering counting 50% of the protein as carbohydrate intake goes lower than 150g per day.
- You only need to count 25% of protein when carbohydrate intake is negligible.
- Managing blood glucose during exercise becomes easier as carbohydrate intake reduces. But performance, especially high-intensity exercise suffers.
- If you want to be true KETO as an adult (not good for children!), you need to keep protein to less than 1.5g/kg (0.7g/lb) and increase fat up to 75% of energy intake. If blood ketones are not 0.6-3.0mmol/l, you are not getting the proposed benefit of nutritional ketosis.
- Reducing carbs and increasing fat may change your lipid profile. You need to get a detailed lipid breakdown to understand if it’s a positive or negative change. Ideally, you want to get your LDL-Particle number measured before and after any change.
- It’s energy restriction that drives fat loss, not macro-nutrient composition.
References
1. https://jissn.biomedcentral.com/articles/10.1186/1550-2783-11-20
1.http://ajcn.nutrition.org/content/early/2016/07/05/ajcn.116.133561
2. hthttps://jissn.biomedcentral.com/articles/10.1186/s12970-017-0174-y
3. https://www.ncbi.nlm.nih.gov/pubmed/16360350
4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664115/
5. http://www.ajconline.org/article/S0002-9149(04)00517-X/abstract
Do you want to know when a new section of blog is added, click here.