Exercise and Type 1 Diabetes
The 20 by 2 Rule: Activity Snacking
Post-meal glucose rises are one of the most persistent challenges in type 1 diabetes. Even with rapid insulin and advanced closed-loop systems, glucose often rises steeply before settling. Short bursts of physical activity, “activity snacking”, represent one of the most accessible and evidence-backed tools for working with insulin rather than against it.
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
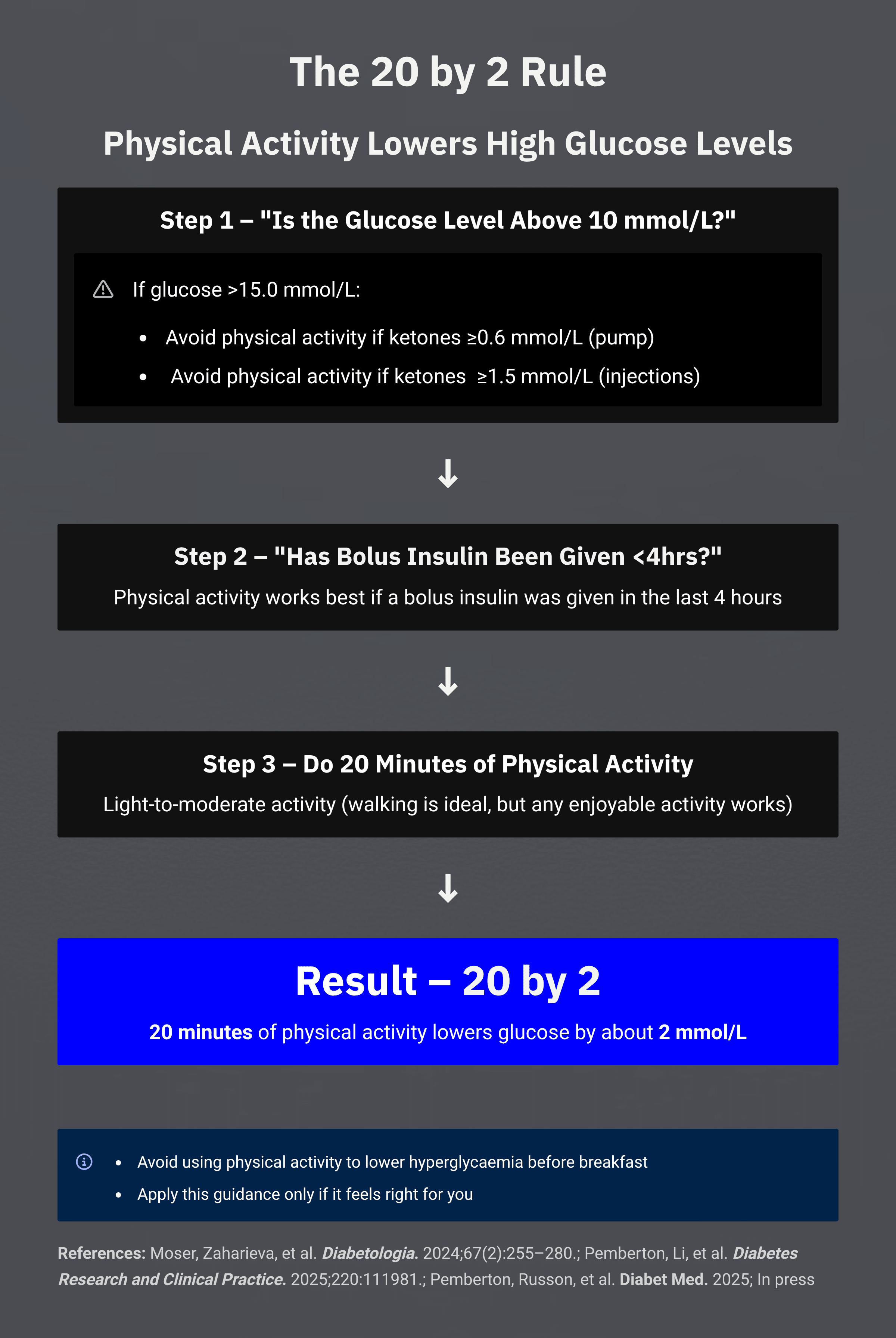
The 20 by 2 rule
The core principle is simple:
20 by 2: 20 minutes of movement tends to lower glucose by around 2 mmol/L on average in people with type 1 diabetes.
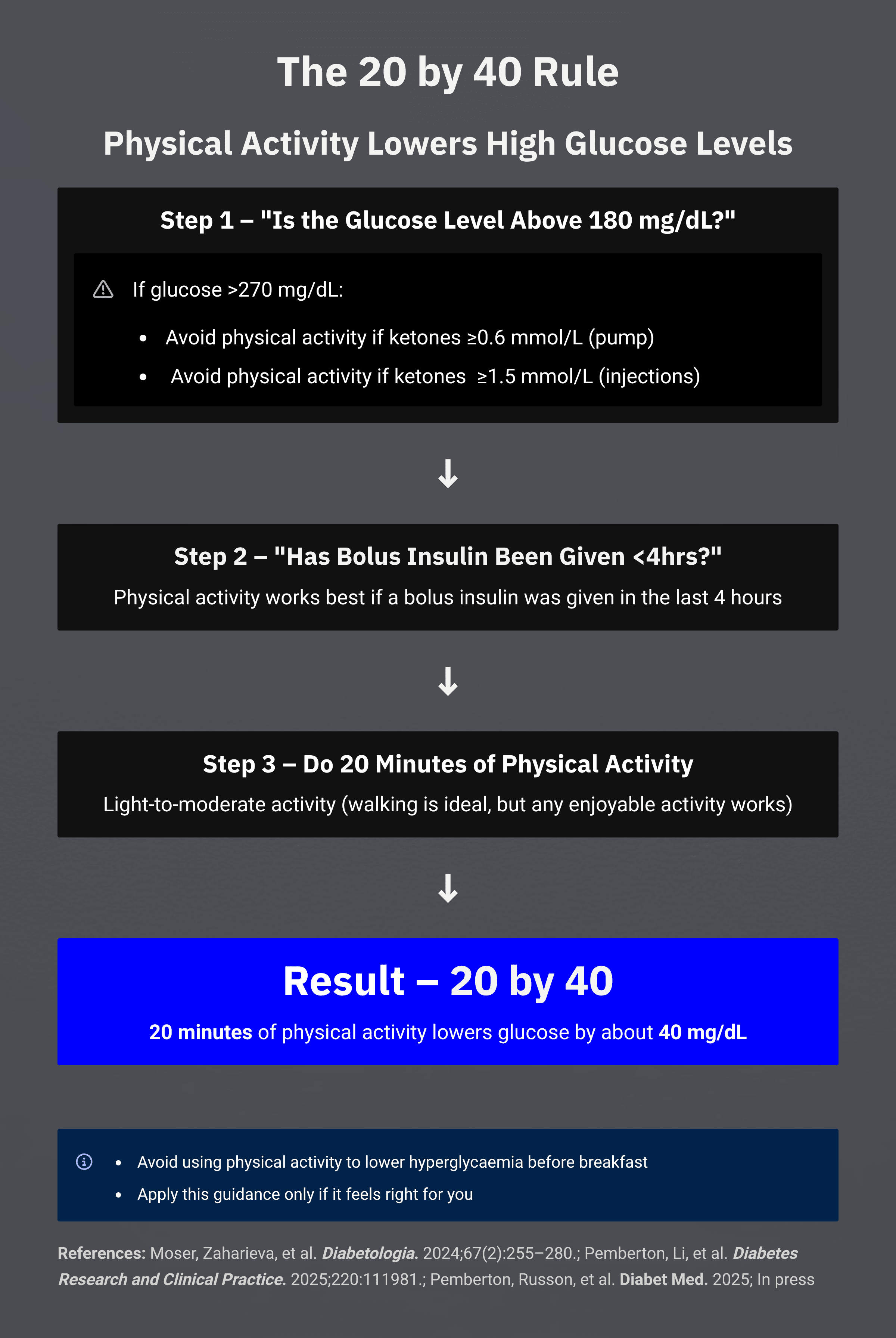
For those using US units, the same principle expressed in mg/dL is:
20 by 40: 20 minutes of movement tends to lower glucose by around 40 mg/dL on average.
Two ways of expressing the same average response. What varies considerably between individuals, and even within the same individual from day to day, is the magnitude and timing of that response. Your own CGM data is the best guide to how this plays out for you.
Why it tends to work: the mechanism
The reason post-meal glucose rises in type 1 diabetes is largely a timing problem. Subcutaneous insulin, even the fastest modern analogues, cannot absorb and act as quickly as glucose enters the bloodstream from a meal.
Physical activity changes that equation. The mechanism here is insulin sensitisation and enhanced glucose uptake by working muscle. When muscles contract, they take up glucose more readily, independently of insulin, through GLUT4 transporter activation, and the insulin already on board becomes more effective at driving glucose into cells.
In other words, movement amplifies the insulin already circulating. It is not replacing insulin action; it is enhancing it.
This matched-pair causal analysis of more than 1,500 activity bouts, accepted for publication in Diabetic Medicine (Pemberton & Russon et al, 2025, in press), moved this from observational data and small paediatric studies into robust causal inference evidence.
Crucially, the analysis showed consistency across:
- All activity types, walking, cycling, household tasks, sport
- All therapy types, MDI, pump, hybrid closed loop
- All ages and genders
That breadth matters. It suggests that the mechanism is widely applicable, regardless of treatment modality, though individual responses will still vary considerably.
Supporting evidence
- Pemberton & Russon et al, 2025, in press, Diabetic Medicine: 20 minutes of activity reduced glucose by 2.2 mmol/L on average (approximately 40 mg/dL), eight times more effective than matched rest.
- Pemberton et al, 2025: Duration of physical activity required to ameliorate hyperglycaemia without causing hypoglycaemia in type 1 diabetes, T1DEXI adults and paediatric cohort analyses.
- Turner & Riddell, 2024: Pre-meal walks improved time in range compared with walking after meals.
- Campbell et al, 2023, SIT LESS trial: Breaking up sitting with light activity reduced hyperglycaemia without extra hypoglycaemia.
- Manohar et al, 2012: Even gentle walking halved post-meal spikes on average.
Exploring this for yourself
The average response, a drop of around 2 mmol/L (40 mg/dL) over 20 minutes, is a useful starting framework. Many people find that it holds broadly true for them. Others find the response is smaller, larger, or varies significantly depending on timing, intensity, and what else is happening physiologically.
The conditions where this tends to be most relevant:
- Glucose is elevated above a comfortable threshold and insulin has been given in the preceding few hours
- There is no concern about ketones
- Activity is of moderate intensity, walking, cycling, light household tasks all count
Important considerations:
- The response is amplified by insulin on board. More active insulin tends to mean a larger glucose-lowering effect, which also means the risk of overshooting is worth being aware of.
- At glucose levels above 15 mmol/L (approximately 270 mg/dL) with ketones present, exercise is generally not appropriate until the ketones and elevated glucose are addressed.
- High-intensity or anaerobic exercise can have the opposite initial effect, a transient glucose rise driven by adrenaline, before a later drop.
The best way to understand your own response is to observe it systematically. Use CGM to watch what happens before, during, and after a 20-minute walk under different conditions, starting glucose, insulin on board, timing relative to meals. Over time, patterns emerge that are specific to you.
This is worth exploring with your diabetes care team, particularly if you want to build a personalised activity snacking strategy into your management.
Background and evidence base: EASD 2025 presentation
The full evidence base and analysis were presented at EASD 2025. Presentation slides are available for download below.
See also the related EASD 2025 presentation: download EASD 2025 slides (PowerPoint).
Download and share: educational toolkit
Take-home 20 by 2 / 20 by 40 guides are available in both mmol/L and mg/dL formats, for clinics, teaching, and personal use. These are free to use for education.
Further listening
Explore this theme on The Glucose Never Lies® Podcast:
Why it matters
Every 20-minute bout of movement is a chance to bend the glucose curve back towards range. More time in range tends to mean better energy, clearer thinking, and a physiology where insulin and activity work together rather than against each other.
That is the principle behind 20 by 2, or 20 by 40. What it means in practice, and how much it changes things for you, is something your own CGM data will reveal over time.