The GNL Podcast, Partying with T1D
Episode 25, Partying with T1D: Alcohol Edition
A festival on its third day, the music still going, a phone screen glanced at somewhere between one round and the next. The night before went fine, so tonight feels safer; in fact the body has been quietly changing the whole time. This is the conversation about drinking that most people with type 1 diabetes have already had with themselves, alone, in the dark, and rarely with anyone who studies it.
Ask Grace
Want to understand why alcohol blocks the liver’s glucose release, and why that risk can arrive late and overnight rather than while you are still drinking?
Part 1 of the Partying with T1D 3-part series, a run of episodes on nightlife, festivals and real-world harm reduction with type 1 diabetes. Podcast hub
Listen or watch
Released 1 December 2025. Available on Buzzsprout, Apple Podcasts, Spotify, and YouTube. Guest: Professor Dessi Zaharieva. Host: John Pemberton. Director of Creativity: Anjanee Kohli.
Why this episode exists
If you live with type 1 diabetes, you have probably already worked out a private set of rules for drinking: what to eat first, what to set the pump to, which friend to tell. You did that quietly, because the official conversation about alcohol and diabetes has too often been silence, or a warning, rather than usable physiology. People with T1D encounter these situations whether anyone talks about them or not.
Alcohol is one of the most widely used psychoactive substances in the world, yet one of the most misunderstood when it comes to type 1 diabetes. So in this episode John and Dessi break the silence around drinking, nightlife, festivals and real-world harm reduction. It is practical physiology combined with lived experience, because the goal is not to moralise but to make a chosen night safer.
In this episode
John and Dessi explore why alcohol affects blood glucose so unpredictably, why glucagon often becomes less effective after drinking, why memory consolidation is disrupted, how liver metabolism changes across multi-day events, and how people with T1D can plan, prepare and stay safer if they choose to drink.
This is the opening episode of the Partying with T1D series, and it sets the physiological foundation the later episodes build on: understand what alcohol does under the hood first, then the harm-reduction strategy makes sense rather than feeling like a list of restrictions.
Watch or listen
Key themes
Alcohol and T1D, what tends to happen
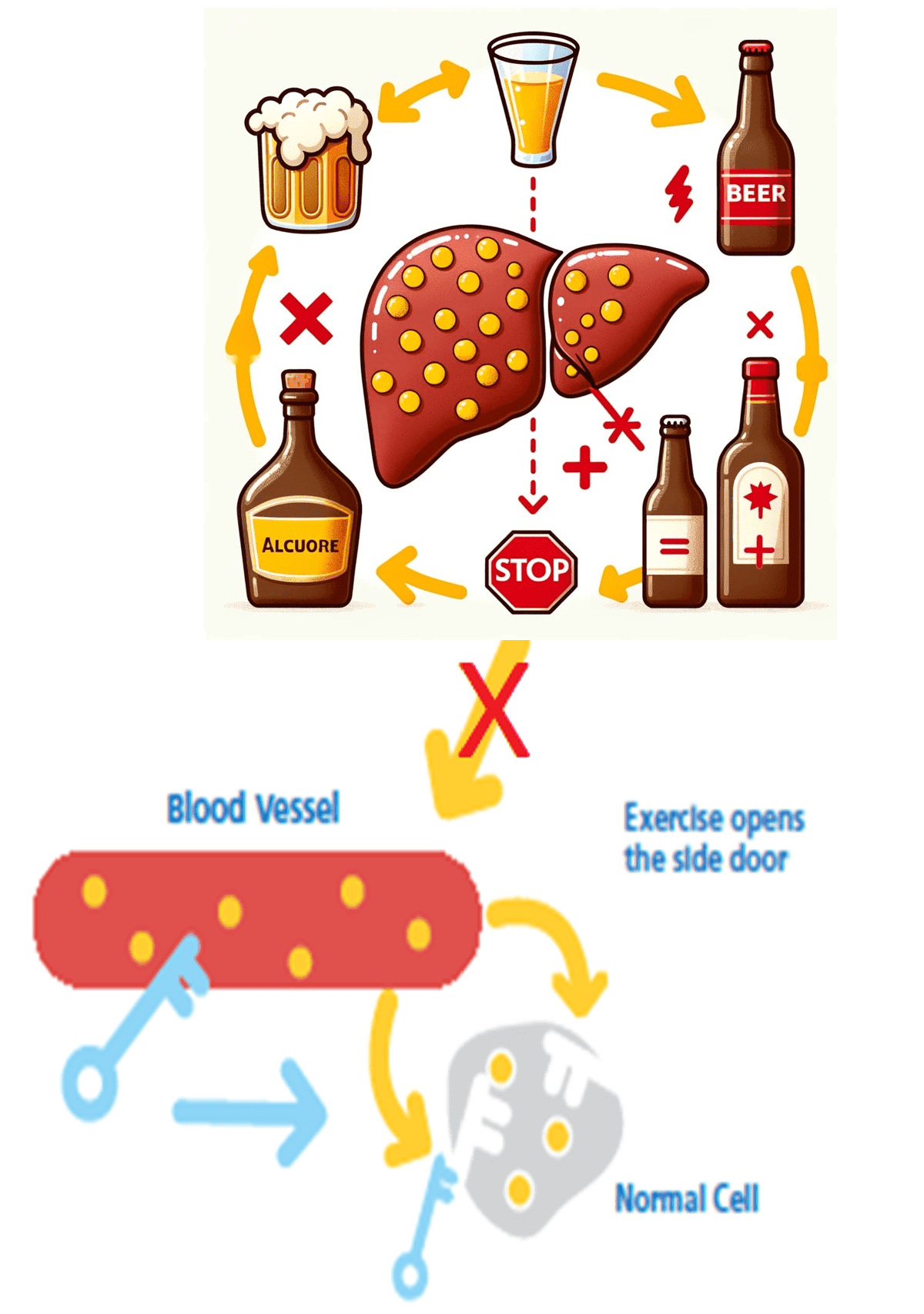
Alcohol suppresses hepatic glucose output, the liver’s ability to release glucose into the bloodstream. When combined with circulating insulin, this tends to increase the risk of hypoglycaemia, particularly overnight. Glucagon becomes less reliable in this setting because little stored glucose remains for the liver to release, so hypoglycaemia can appear late and more severely than expected. The metabolic response varies widely between individuals, and multi-day drinking changes physiology and extends hypoglycaemia risk.
Why memory is disrupted
Part of why the next morning is a blank is physiological rather than simply “too much”. Alcohol shuts down REM sleep, and no REM sleep means no memory consolidation. Wearables often show near-zero REM after drinking, which is a useful objective marker that the night was not restorative even when sleep felt long.
Why the first night tends to be the most difficult
On the first night of a multi-day event the alcohol-metabolising enzymes (ADH) are not yet upregulated. The same intake therefore produces higher intoxication, higher hypoglycaemia risk, and less predictable glucose patterns than later nights, which is the opposite of how most people instinctively rank the danger.
Insulin strategy, approaches people explore
There is no single correct setting, but the conversation names the levers people discuss with their care teams: scaled basal reductions (25-75%) based on units consumed, worth discussing with your care team to find what works for you; using Activity Mode on AID systems; and switching to MDI or manual mode for festivals. One practical safety point recurs: awareness of double-basal risk when reconnecting pumps after long-acting insulin.
Harm reduction principles
The episode’s harm-reduction frame is deliberately pragmatic rather than moralising: CGM plus a hypo plan plus a buddy system; eating before drinking; predictability over perfection; and pragmatic strategies over moralising. The aim is a night that is plannable, not perfect.
For parents and clinicians
Silence around alcohol tends to increase risk rather than reduce it. Young people need support, not shame, and open, honest conversation is the antidote to secrecy and preventable harm. The same point lands for clinicians who want pragmatic guidance rather than a blanket warning that gets ignored.
Predictability over perfection. The trade-off the episode keeps returning to is that you cannot make a night with alcohol behave perfectly, but you can make it predictable. Eating before drinking, a CGM with a hypo plan, a buddy who knows what to do, and an insulin strategy agreed with your care team do not remove the risk; they shift it from a surprise into something you have planned around.
Practical exploration
For people living with type 1 diabetes and their families
If you are going to drink, the episode’s strongest theme is that planning beats avoidance, and that the risk is loaded towards the hours after you stop rather than while you are out.
- Alcohol blocks liver glucose release and can drive hypoglycaemia that appears late and overnight; a CGM, a hypo plan, and a buddy system are the harm-reduction basics worth having in place before the night, not during it.
- Eating before drinking and aiming for predictability over perfection are the principles the episode foregrounds; the goal is a plannable night, not a flawless glucose trace.
- On the first night of a festival or multi-day event, the same intake tends to hit harder, because the alcohol-metabolising enzymes are not yet upregulated; allow for that rather than assuming the second night’s experience.
- Scaled basal reductions (25-75%) based on units consumed are one of the approaches people explore; this is a conversation to have with your care team to find what works for you, not a fixed instruction.
- If you use a pump and reconnect after long-acting insulin, be aware of the double-basal risk the episode flags.
For clinicians and educators
The episode is an argument that the way to reduce alcohol-related harm in T1D is to talk about it openly, with physiology and pragmatism, rather than to warn it away.
- Silence around alcohol tends to increase risk rather than reduce it; young people need support, not shame, and open, honest conversation is the antidote to secrecy and preventable harm.
- The first-night ADH point and the late, overnight timing of hypoglycaemia risk are worth teaching explicitly, because they run counter to most people’s intuition.
- AID-era options (Activity Mode, switching to MDI or manual mode for festivals, scaled basal reductions) give a concrete menu to discuss, alongside the double-basal reconnection caution.
- REM suppression and the near-zero REM often seen on wearables after drinking give an objective way to explain why the night was not restorative.
About the guest
Professor Dessi Zaharieva is an exercise physiologist, instructor at Stanford, and diabetes researcher. She has lived with type 1 diabetes for almost 30 years and focuses her scientific work on exercise, physiology and real-world T1D challenges. Dessi serves as a Scientific Advisor to The Glucose Never Lies.
Related reading on GNL
Episode 25 of the GNL Podcast
Partying with T1D: Alcohol Edition
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.