The GNL Podcast
Episode 18, exercise without fear
It is hour two of a long walk, the legs feel good, and then the phone shows a number falling with two arrows pointing down. The reflex is to stop, to reach for the gel, to wonder whether the next session is worth the worry at all. This episode is about the moment before that reflex, the moment when a plan you trust lets the walk carry on.
Listen and watch
Available on Buzzsprout, Apple Podcasts, Spotify, and YouTube. Guest: Professor Othmar Moser, exercise physiologist, guideline author (CGM and AID), lives with type 1 diabetes. Host: John Pemberton, The Glucose Never Lies. Length: approximately 60 minutes.
Why this episode exists
If you live with type 1 diabetes, you have probably learned to be wary of exercise in a way other people never have to be. A walk, a swim, a five-a-side game: each one carries the quiet arithmetic of how low you might go and how late the drop might land. Plenty of people scale back the very movement that would help them most, not because they do not want to move, but because the unpredictability feels like more trouble than it is worth.
Prof. Othmar Moser sits in an unusual place to answer that. He is an exercise physiologist and a guideline author in diabetes technology, and he lives with type 1 diabetes himself, so he brings lab-grade evidence into real-world routines, from weekend walks to elite sport. His starting point is blunt: he would prefer someone with 70% time in range who exercises every day over someone with 100% time in range doing no exercise, because exercise is, as he puts it, a multipotent drug. An exercise and activity FAQ was built on the back of this episode and is kept continuously updated.
In this episode
John and Othmar walk through how movement and insulin can coexist safely, starting from why general daily activity is low hypo-risk and hugely beneficial, and building towards a before, during and after framework that works across multiple daily injections, pumps, and automated insulin delivery (AID) systems including CamAPS. The conversation is honest about where consensus guidelines are practical rather than perfect, and about where individual response means there is no single right answer.
The single thread running through it is timing: insulin on board is one of the main drivers of hypoglycaemia, so much of safe exercise comes down to what you do before you start, how you read the signal while you move, and how you protect the hours afterwards, including the night.
Episode chapters
- 00:00, Intro and why the show exists
- 01:30, Meet Prof. Othmar Moser
- 06:00, How consensus guidelines are made, and why they’re practical, not perfect
- 11:00, The exercise discs: planned vs unplanned; insulin and carb logic
- 17:00, Before exercise: temp targets, prandial reductions, timing your meals
- 25:00, During exercise: ranges, carb top-ups, CGM vs fingerstick
- 35:00, After exercise: the first hour, evening drops, protein strategy
- 45:00, AID nuance: manual mode for consistency; hybrid solutions for athletes
- 52:00, Future: faster insulins, fully closed loop, glucagon co-hormone systems
- 57:00, Q&A highlights, wrap-up and key messages
Watch or listen
Key themes
Movement first, before any clever protocol
Before any of the technical detail, Othmar’s central claim is that general movement is low hypo-risk and hugely beneficial. The simplest version is a ten-minute walk after each meal, which tends to flatten the post-meal peak and, just as importantly, builds confidence over time. His framing puts this above any individual glucose target: as he says it, he would rather see someone with 70% time in range who exercises every day than someone with 100% time in range doing no exercise, because exercise is a multipotent drug. The older people living with type 1 he sees thriving in their eighties are, on his account, the ones who stayed physically active their whole lives.
Before exercise, insulin on board is the lever
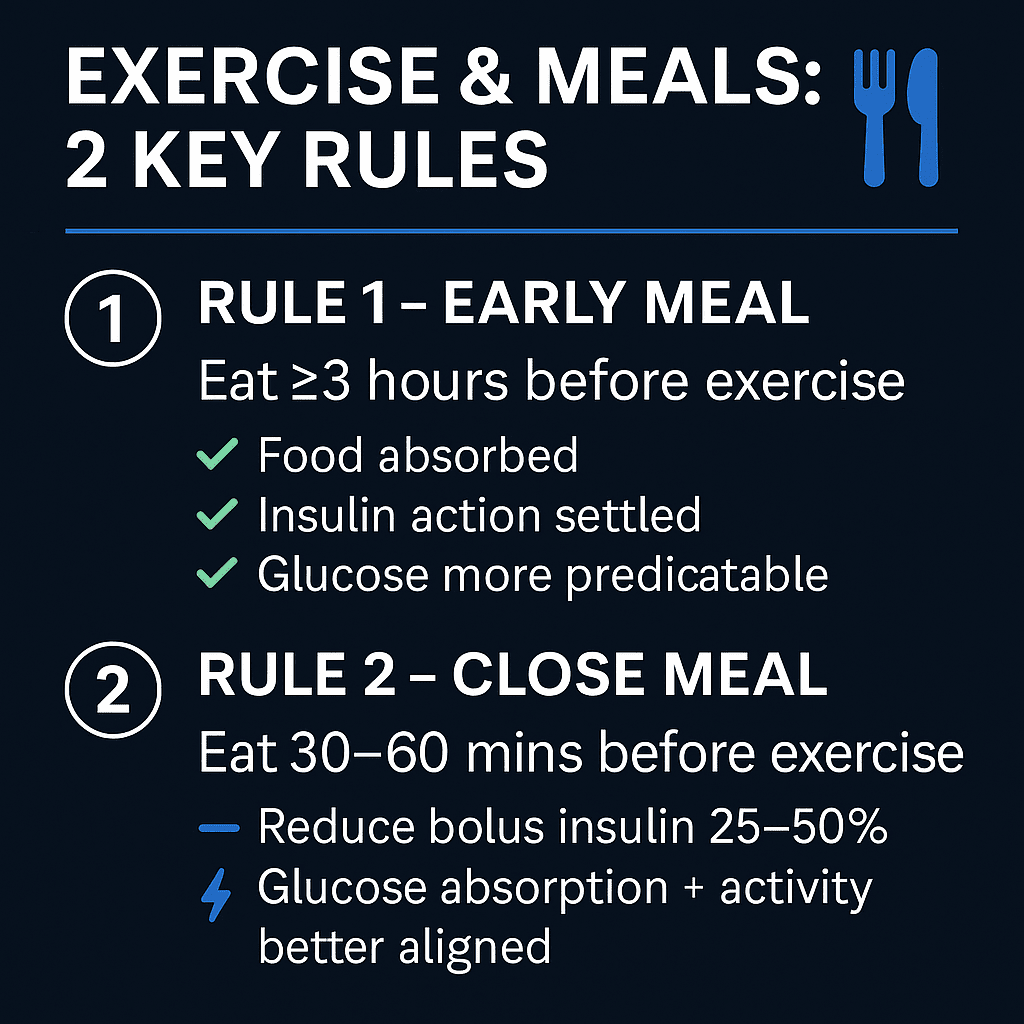
Most of the hypo risk is set before the session starts. Insulin on board is one of the main drivers of hypoglycaemia, so starting an AID system’s exercise mode early matters: around two hours before helps most, and one hour still makes a difference. If you are eating within two hours of exercise, a starting point of around a 25% bolus reduction is often explored, then fine-tuned with CGM data. Keeping the meal within one hour before exercise tends to reduce glucose spikes. None of these are fixed rules; they are starting points to adjust against your own response, and the 1-hour and 3-hour timing diagram above is a way to picture them.
During exercise, when the trend arrow stops being enough
While moving, many people aim for 7 to 10 mmol/L (126 to 180 mg/dL), with carbohydrate top-ups of 3 to 20 g depending on trend, therapy, and individual response, and a check every 20 to 30 minutes as a common starting point. The harder lesson is about the sensor itself. CGMs are extremely accurate when you are lying still in bed, but during exercise, with insulin on board and arrows pointing down, the reading can be 10 mmol/L off. That is the moment a fingerstick matters, in particular when double-down arrows appear below 7 mmol/L, because exercise increases the lag risk in the sensor.
After exercise, the night is the part people miss
Most people do not go low during the exercise itself. The highest risk tends to fall in the first hour afterwards, and then again around 2 a.m. if the session was late in the evening. For evening activity, the strategies discussed include temporary targets, basal adjustments, and a 20 g protein snack before bed for a gentle overnight glucose rise; modest carbohydrate may suit those not using an AID system. The point is that the plan does not end when the session does.
Where consistency beats automation
The framework holds across MDI, pump, and AID systems including CamAPS, but the conversation does not pretend automation always wins. Some people in competitive sport prefer manual mode for the consistency it gives them, and hybrid solutions have a place for athletes. The episode also looks ahead to faster insulins, fully closed loop systems, and glucagon co-hormone systems, while keeping the focus on what is workable now.
Time in range is not the whole story. The trade-off the episode keeps naming is between a tidy glucose number and a life lived in motion. On Othmar’s account, 70% time in range combined with daily activity often supports long-term health better than 100% time in range with no physical activity, based on what the evidence tends to show. Glucose control is important, but it is not everything.
Practical exploration
For people living with type 1 diabetes and their families
The most useful takeaway is that small, regular movement is the foundation, and the technical adjustments sit on top of it rather than replace it.
- A ten-minute walk after each meal is a low-risk way to flatten the post-meal peak and build confidence over time.
- Insulin on board is a key driver of hypos on average, so on an AID system, starting exercise mode around two hours before helps most; one hour still makes a difference.
- If eating less than two hours before exercise, a starting point of around a 25% bolus reduction is often explored, then fine-tuned with CGM data; keeping the meal within one hour before exercise tends to reduce glucose spikes.
- During exercise, many people aim for 7 to 10 mmol/L (126 to 180 mg/dL), with carbohydrate top-ups of 3 to 20 g depending on trend, therapy, and individual response, checking every 20 to 30 minutes as a starting point.
- Double-down arrows below 7 mmol/L are worth considering a fingerstick, because exercise increases the risk of CGM lag.
- The highest hypo risk tends to fall in the first hour after exercise, and evening sessions can cause drops around 2 a.m. on average; a 20 g protein snack before bed is one strategy explored for a gentle overnight rise, with modest carbohydrate sometimes suiting those not using an AID system.
For clinicians and educators
The episode reframes exercise advice from a list of fixed numbers into a before, during and after conversation that adapts to therapy and individual response.
- Lead with the case for general movement before any protocol detail; 70% time in range with daily activity often supports long-term health better than 100% time in range with none, based on what the evidence tends to show.
- Teach insulin on board as the main lever before exercise, and the timing of exercise mode (around two hours ahead where possible) as the practical handle on AID systems.
- Set expectations on CGM reliability during activity: accuracy can drift by up to 10 mmol/L with insulin on board and falling arrows, so a fingerstick is the safe move on double-down arrows below 7 mmol/L.
- Carry the plan into the night: the first hour and the 2 a.m. window after evening activity are where the risk concentrates, and a protein-based overnight strategy is one option to explore with the person.
- For competitive sport, manual mode for consistency is a legitimate choice for some people, and hybrid solutions have a role.
The consensus guidelines this conversation draws on, and the AID exercise discs adapted for clinic use, are listed below.
About the guest
Professor Othmar Moser is an exercise physiologist and guideline author in diabetes technology (CGM and AID). Living with type 1 diabetes, he brings lab-grade evidence into real-world routines, from weekend walks to elite sport.
Related reading on GNL
Episode 18 of the GNL Podcast
Exercise without fear
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.