The GNL Podcast, Inspiring Stories
Episode 27, T1D Looping Blind
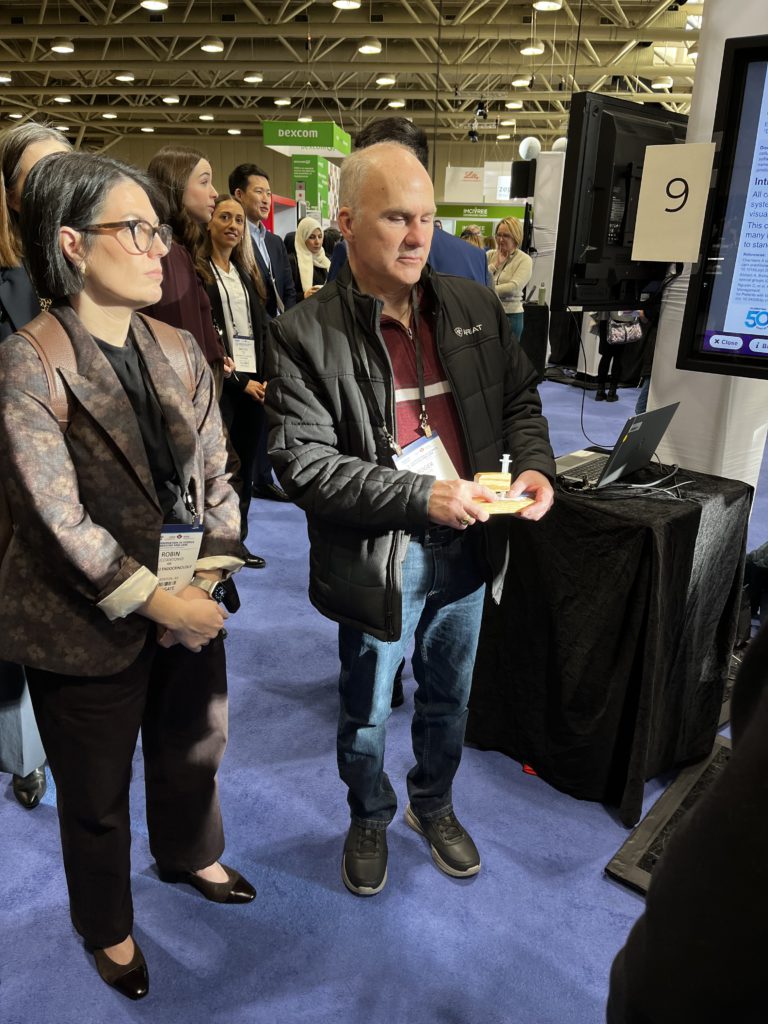
A pod has to be filled the same way, every time, by feel alone. So Roger Moore carved wells into a block of wood that hold the pod and the insulin vial in fixed positions, and now the whole thing aligns by touch. Modern automated insulin delivery had promised him safety. The problem was that none of it had been built for a person who cannot see the screen.
Ask Grace
Want to understand how open-source Loop differs from a commercial automated insulin delivery system, and what a stepwise simulator-to-saline-to-insulin rollout actually involves?
Part of GNL Inspiring Stories, the strand of the GNL Podcast that follows what people living with type 1 diabetes build when the system in front of them does not fit. Podcast hub
Listen or watch
Available on Spotify, Apple Podcasts, Buzzsprout, and YouTube. Guests: Roger Moore and Robin Lucciantonio, diabetes educator. This is an Inspiring Stories episode describing the independent experiences of the people featured.
Why this episode exists
If you have lived with type 1 diabetes for a long time, you already know the difference between a tool that exists and a tool you can actually use. You have probably worked around a menu that buries the thing you need, an alarm you cannot hear, a screen you have to squint at in the dark. Roger Moore has spent decades on the far end of that spectrum: diagnosed with type 1 diabetes at age two, long before blood glucose meters were commonplace, and totally blind for more than 35 years. He managed for years through touch, routine, and workarounds.
When continuous glucose monitoring and automated insulin delivery (AID) arrived, they promised safety and reduced burden. For Roger they brought a new problem instead: much of the interface and onboarding assumes sight, with graphs, sub-menus, unlabelled UI elements, and touchscreen workflows that offer no tactile landmarks. The safety upgrade became a locked door. This episode exists because Roger and diabetes educator Robin Lucciantonio refused to accept that exclusion, and built around it.
In this episode
Building accessible automated insulin delivery through ingenuity, stepwise safety, and a team that refused “impossible”.
Roger has lived with type 1 diabetes since age two and has been totally blind for more than 35 years. Modern automated insulin delivery promised safety and reduced burden, but commercial systems were effectively inaccessible without sight.
Roger and Robin walk through how they used the open-source Loop app with iPhone VoiceOver, a stepwise rollout (simulator, then saline, then insulin), and a handcrafted tactile pod-filling station to make AID genuinely autonomous. They describe how they identified and ironed out accessibility challenges, and why they progressed in controlled steps rather than leaps of faith.
The result was not just better numbers: it was independence, reduced hypoglycaemia, and a blueprint for what accessibility should mean in diabetes technology.
Read the full Inspiring Story with extra detail: Roger’s T1D journey toward freedom
Episode timestamps
- 00:10, Why this podcast exists
- 01:11, Introducing Roger and Robin: why this story matters
- 03:10, Diagnosed at age two; diabetes tools before modern meters
- 03:58, Losing sight: what changed, what became harder
- 04:18, Tactile insulin delivery: Count-a-Dose, routine, and risk management
- 06:15, Talking meters and workarounds: necessity as engineering
- 10:45, CGM: what VoiceOver did and did not reveal
- 13:51, Why commercial AID systems were not viable for independent use
- 15:19, The genesis: “What about Loop?”
- 18:54, Simulator and accessibility testing: learning the interface safely
- 22:11, Saline trial and staged rollout: building competence, not gambling
- 23:12, The tactile pod-filling station: Mark 1 to Mark 2
- 28:01, VoiceOver in action: what the system actually reads out
- 31:19, Outcomes: HbA1c, time in range, and hypoglycaemia
- 37:22, Clinical lessons: hand-over-hand teaching and landmarking
- 41:27, Closing reflections: survival to thriving, and what should change next
Watch or listen
You can also see, on YouTube, one of the most practical pieces of accessibility engineering in diabetes care: a custom wooden tactile pod-filling station designed to prevent misalignment and make pod filling reliable by feel alone.
Key themes
Living with T1D without visual feedback
Roger was diagnosed with type 1 diabetes at age two, long before blood glucose meters were commonplace, and in his twenties he lost his sight. For decades he managed diabetes through touch, routine, and workarounds: tactile insulin delivery with Count-a-Dose, talking meters, and the kind of necessity-driven engineering that turns a daily task into a reliable system. The thread that runs through the whole conversation is that independence in diabetes is not motivational; it is safety-critical.
Accessibility failures in mainstream diabetes technology
When CGM and AID arrived, much of the interface and onboarding assumed sight. CGM and app interfaces did not expose key information to screen readers; pumps carried complex menu structures with no practical non-visual navigation; touchscreen workflows offered no tactile landmarks. The episode keeps returning to a single distinction: “it exists” is not the same as “it is usable”. For Roger, the safety upgrade became a locked door.
The build: Loop, VoiceOver, and stepwise safety
Rather than accept exclusion, Roger and Robin built a solution around first principles: autonomy, repeatability, and safety. Open-source Loop became the viable doorway for AID, and iPhone VoiceOver made it usable non-visually. Algorithm build and maintenance support meant the burden did not fall on the person living with diabetes. The transition was de-risked in controlled steps rather than leaps of faith: simulator first, then a prolonged saline trial, then going live with insulin.
Practical accessibility engineering: the tactile pod-filling station
Pod filling is a safety problem without tactile alignment. Roger’s answer was a handcrafted wooden station with carved wells that hold the pod and insulin vial in fixed positions, so the fill aligns by feel alone. He describes the design evolution from Mark 1 to Mark 2, and how repeatability, error-proofing, and building confidence by touch turned an anxious task into a dependable one.

Outcomes that matter: numbers, burden, and autonomy
The outcomes were not only improved glucose stability and reduced hypoglycaemia, though those were real. They were also less time spent managing highs and lows, and a kind of freedom that Roger frames as restored dignity rather than convenience. The chapter on outcomes covers HbA1c, time in range, and hypoglycaemia together, because the point of the build was never a single statistic.
What clinicians can learn: hand-over-hand training and real inclusion
Robin’s contribution is the clinical translation. Tactile orientation and landmarking cannot be skipped. A visual workflow has to be turned into a non-visual one safely, step by step, rather than assumed to carry across. And open-minded teams turn out to be a determinant of access in their own right: the willingness to think from first principles is part of the clinical skill, not separate from it.
Safety upgrade, locked door. The trade-off this episode names is the one at the centre of the whole story: a therapy that meaningfully reduces risk is only an upgrade for the people who can actually operate it. When CGM and AID assume sight, the very people who could gain most from reduced hypoglycaemia are the ones shut out. Accessibility is not a feature; it is a safety requirement, and excluding people who cannot use a touchscreen or read a graph is not a neutral limitation, it is a preventable harm.
Practical exploration
For people living with type 1 diabetes and their families
Roger’s story is not a template to copy step for step; it is evidence that autonomy is possible, and a set of questions worth carrying into your own care.
- If a device exists but you cannot operate it independently, that is a reason to ask for support, not a reason to assume the door is closed. “It exists” is not the same as “it is usable”, and that gap is something your care team can help work on.
- A staged rollout (simulator, then saline, then insulin) is how Roger and Robin de-risked the move to AID. Building competence in steps, rather than gambling on a single leap, is a pattern worth discussing with your team.
- Tactile landmarking and repeatable routines turn an anxious task into a reliable one. The pod-filling station is one example; the principle is general.
- Open-source Loop with VoiceOver was the doorway here, with algorithm build and maintenance support so the burden did not fall on the person alone. If you are exploring options, the support around the tool matters as much as the tool.
For clinicians and educators
Robin’s experience is a quiet argument that accessibility is a clinical skill, and that real inclusion changes what a service can deliver.
- Tactile orientation and landmarking cannot be skipped. Hand-over-hand teaching is how a non-visual workflow gets learned safely.
- Translate the visual workflow into a non-visual one deliberately, rather than assuming it carries across. The steps that are invisible to a sighted user are often the ones that matter most.
- Staged implementation (simulator, saline, then insulin) maintains safety while building confidence. The progression is the safeguard.
- Open-minded teams are a determinant of access. Building around the human in front of you, not the default user you imagined, is what made this work.
About our guests
Roger Moore
Roger has lived with type 1 diabetes since early childhood and has been totally blind for more than 35 years. Through necessity-driven problem-solving and a refusal to accept exclusion, he developed a fully tactile workflow to use automated insulin delivery independently, including a handcrafted pod-filling station to make the process reliable and safe.
Robin Lucciantonio
Robin is a diabetes educator based in Edmonton, Alberta, working in a general endocrinology clinic. In this episode she shares the practical realities of translating diabetes technology into accessible workflows, including the importance of tactile landmarking, hand-over-hand teaching, and staged implementation to maintain safety.
Related reading on GNL
Episode 27 of the GNL Podcast
T1D Looping Blind
This content is for educational exploration only. It describes the independent experiences of the people featured and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.