
Overview
This page explains how to manage exercise when you use an Automated Insulin Delivery (AID) system (closed loop / hybrid closed loop).
AID systems are brilliant for day-to-day glucose management. During exercise they can feel less predictable, because the algorithm is constantly changing insulin delivery in the background. That means you can start two “identical” sessions with different insulin conditions — even if your starting glucose is the same.
This page follows the GNL rule: major in the majors. For exercise with AID, the dominant drivers are still insulin on board, then starting glucose, then trend arrows. Device modes and exercise type come after.
This page is educational information, not individual medical advice. If you change settings or strategies, discuss it with your own diabetes team.
The detail
New international guidance is available on exercise with AID systems: the EASD–ISPAD consensus statement.
Supplementary graphics from the paper:
System-specific one-page TL;DR guides:
Major 1: Insulin on board (still the main driver)
AID does not remove the core problem of exercise in type 1 diabetes: exercise amplifies insulin action. Whether you’re on injections, pump, or AID, exercise hypos are still usually a problem of too much active insulin for the session you’re about to do.
The practical implication is blunt: the safest exercise sessions (and the most reproducible learning) usually happen when insulin on board is low. A pragmatic anchor is the Three-Hour Rule: avoid starting planned exercise within ~3 hours of your last significant bolus where possible, or intentionally reduce that bolus if activity is unavoidable.
AID can help if you give it time: increasing glucose targets or enabling activity features 1–2 hours before planned exercise can reduce insulin delivery and lower insulin on board at the start.
Major 2: Starting glucose value
Starting glucose is your buffer. If you start low-normal, you have less room for aerobic phases and delayed drops. If you start high, the algorithm may respond with extra insulin, which can increase hypoglycaemia risk once you begin moving.
With AID, this “pre-exercise rise then algorithm response” pattern is common: glucose creeps up pre-session (stress, warm-up, carbs), the system increases insulin, then the session begins and the drop arrives with more force than expected.
Major 3: Trend arrows (direction and speed)
Trend arrows matter more than any single number during exercise. A stable 7.0 mmol/L is not the same as 7.0 mmol/L with a downward trend. During exercise, make decisions using value + direction.
A useful starting heuristic from clinical practice is to begin supplementing with carbohydrate below about 7.0 mmol/L (126 mg/dL) if trending down, using small amounts regularly (often 3–20 g every 20–30 minutes). The correct dose depends on intensity, duration, and your trend arrows.
Why AID can make exercise feel less predictable
AID systems adjust insulin frequently in the background. That’s exactly why they work so well overnight and day-to-day.
During exercise, the downside is reproducibility: you rarely start two sessions with the same insulin conditions. The algorithm may have been more aggressive (or less) for hours before you even begin. That makes trial-and-error harder, because “same session” doesn’t mean “same starting physiology”.
When manual (open-loop) can be more predictable
One pragmatic strategy used in clinical practice is to temporarily step out of full automation to increase repeatability.
- Set a manual basal rate appropriate for your planned exercise.
- Switch to open-loop (or a less automated mode) around ~2 hours before the session so insulin conditions stabilise.
- Run that stable basal into and during the activity, then use small carbohydrate adjustments based on glucose value and trend arrows.
- After exercise, switch back to closed loop to regain the benefits of automation, especially overnight.
This is not a “better” way to live — it’s a way to make learning more scientific: stable starting conditions → clearer pattern recognition → better personal playbook.
Where exercise type fits (secondary)
Exercise type matters, but it comes after insulin on board, starting glucose, and trend arrows.
- Aerobic tends to lower glucose.
- High-intensity / sprint work may raise glucose first (adrenaline), with a later drop once hormones settle.
- Resistance training can be variable: smaller immediate drops but meaningful delayed effects on insulin sensitivity.
The art with AID is layering device tools (targets/modes) on top of these fundamentals, rather than trusting the algorithm to “figure it out”.
System-specific considerations (what the features actually do)
Each system has its own constraints. The goal is the same: reduce insulin on board at the start of activity, then manage glucose using trend-informed carbohydrate and sensible targets/modes.
Beta Bionics iLet: limited ability to adjust glucose targets pre-exercise, so carbohydrate planning and real-time carb supplementation become especially important.

CamAPS FX: “Ease-off” mode raises targets / reduces aggressiveness. Best used in advance so insulin on board is lower when activity starts.

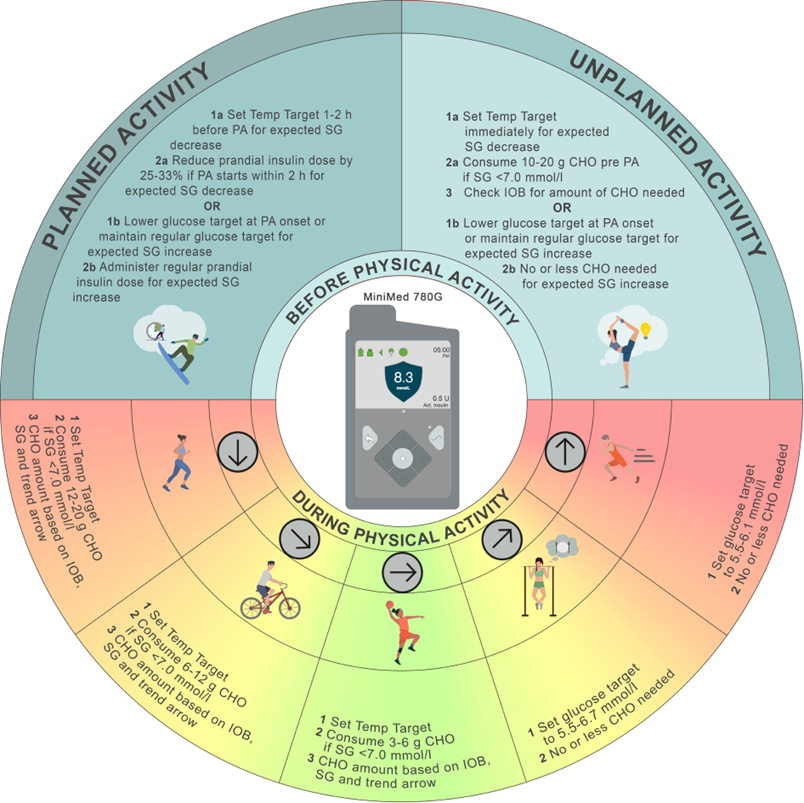
MiniMed 780G: “Temp Target” raises the target and stops automated correction boluses during exercise, which can help prevent repeated lows once you start moving.
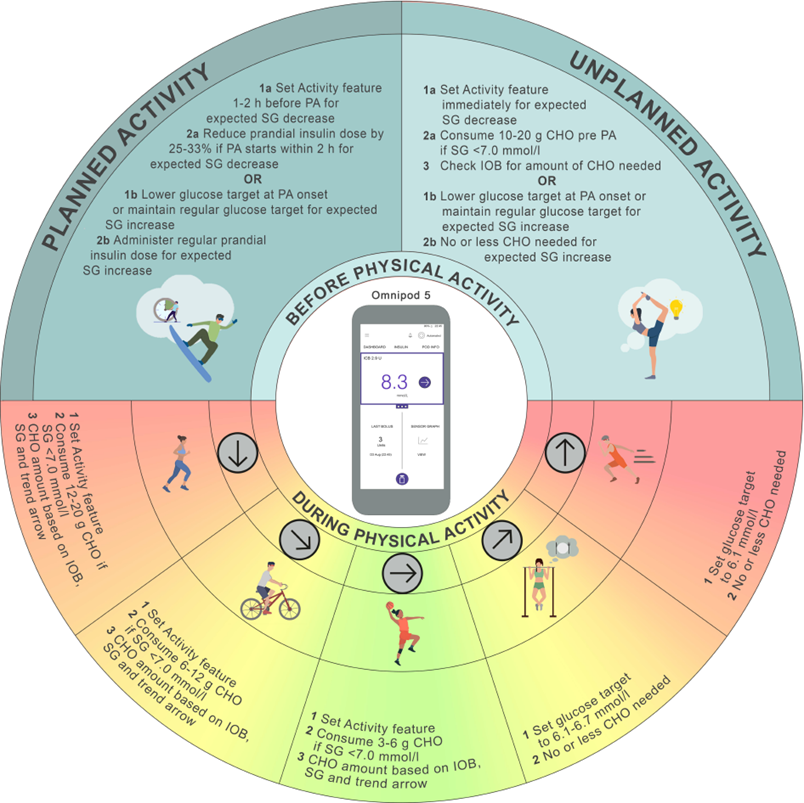
Omnipod 5: “Activity” feature sets a higher target and makes the algorithm less aggressive. Used early enough, it reduces insulin on board before the session.
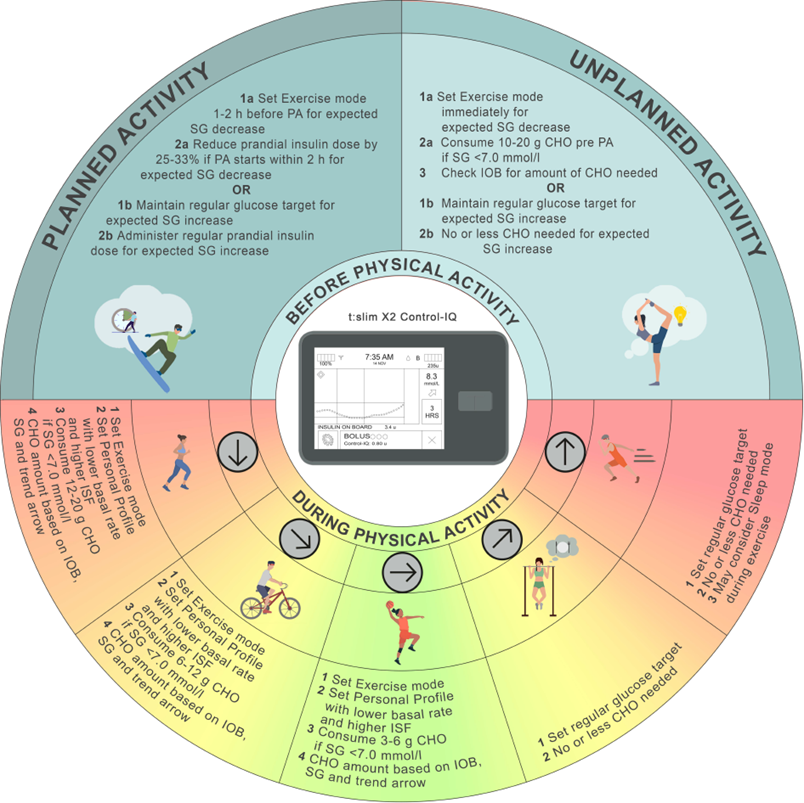
Tandem t:slim X2 Control-IQ: “Exercise Mode” shifts targets upward and moderates insulin delivery; useful when enabled in advance for sessions that usually drop glucose.
DBLG1: “Physical Activity” mode for exercise; “ZEN” mode can raise the protective target for long or unpredictable sessions.

Practical
Use this as a practical starting framework to discuss with your team and experiment with safely.
- Planned exercise: use your system’s activity mode / higher target 1–2 hours before the session to reduce insulin on board at the start.
- If exercise is within ~2 hours of a meal: reduce the carbohydrate amount you enter into the system by ~25–33% (a practical way to reduce bolus insulin). The algorithm cannot “recreate” insulin you never gave.
- Unplanned exercise: set a higher target immediately and use small amounts of fast-acting carbohydrate if glucose is <7.0 mmol/L and trending down.
- During exercise: favour small, repeated carb doses guided by value + trend arrows over large reactive corrections.
- If exercise feels chaotic: consider a reproducibility block using manual/open-loop for planned sessions (stable basal → clearer learning), then return to closed loop afterwards.
- After exercise: expect delayed risk (especially after longer sessions). Be cautious with late corrections; consider whether you need a less aggressive insulin strategy overnight.
- CGM lag still applies: if symptoms don’t match the sensor, confirm with a meter.
If you want the one-page versions, use the system-specific TL;DR guides above and keep the consensus graphics to hand.
What’s next
Next step: Exercise and T1D FAQ or Podcast episode: Prof. Othmar Moser on exercise and Type 1 diabetes