
Continuous Glucose Monitoring (CGM) has transformed life with type 1 diabetes (T1D). Real-time data, trend arrows, alerts, and pattern recognition now make it possible to improve time in range (TIR) in ways that were simply not feasible a decade ago.
But before we talk about optimisation, tips, or performance, two foundations matter more than everything that follows.
Foundation 1: Blood glucose testing still matters
CGM is extraordinary — but it is not infallible.
When a CGM reading does not match symptoms, context, alarms, or common sense, accurate finger-prick blood glucose (BG) testing remains the user’s gold-standard reference. That only works if:
- you have an ISO-standard meter,
- your strips are in date, and
- you still know how to perform a proper finger-prick test.
As CGM use has become widespread, this skill has quietly eroded. That erosion matters most precisely in high-risk situations — alarms, unexpected readings, illness, or insulin dosing decisions — where the downside risk is asymmetric.
Foundation 2: “70% time in range” does not mean the same thing on every CGM
Not all CGM systems measure or report glucose in the same way.
Some CGMs are calibrated closer to capillary glucose, others closer to venous glucose, and some read below venous levels by design. The practical consequence is simple but widely misunderstood:
- The same headline 70% TIR can represent different true glucose exposure depending on the CGM.
- Some systems require roughly 5–10% higher TIR targets to mean the same physiological reality.
If you do not understand how your CGM is calibrated, it is easy to misinterpret performance, chase “inaccuracy” that is actually physiology, or judge yourself unfairly.
Once those two foundations are in place — how to verify and how to interpret — optimisation finally makes sense.
10 Top Tips to Optimise time-in-range
Should you follow them?
I don’t know. I don’t know your physiology, your lifestyle, or your constraints — and I don’t have skin in your game.
View this as education, not instruction, and discuss changes with your diabetes team.
Prefer a podcast? 🎧 Episode 6: Ten Tips to Optimise Time in Range
Here is the quick index with timestamps from the episode:
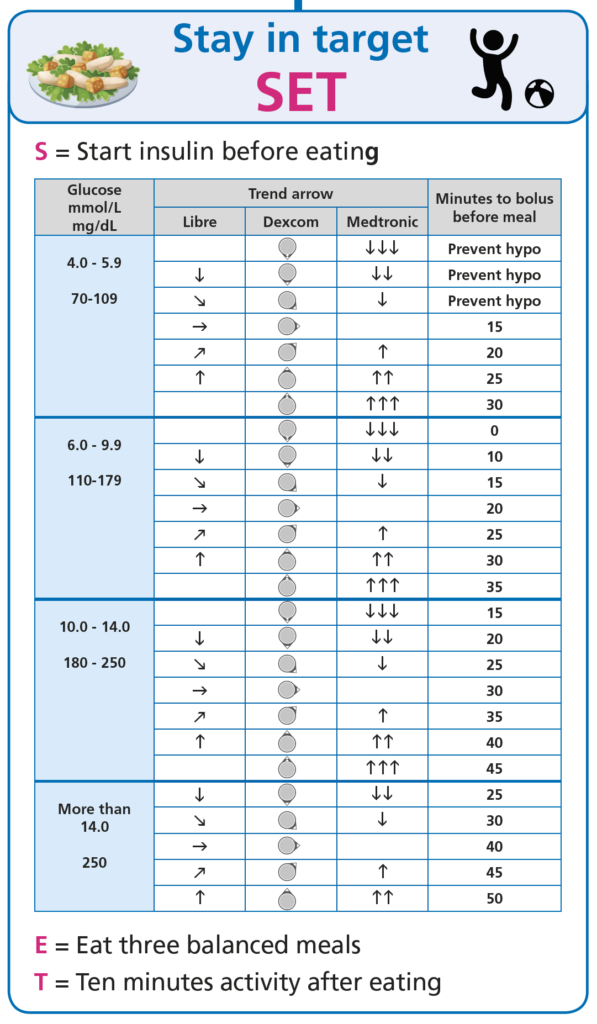
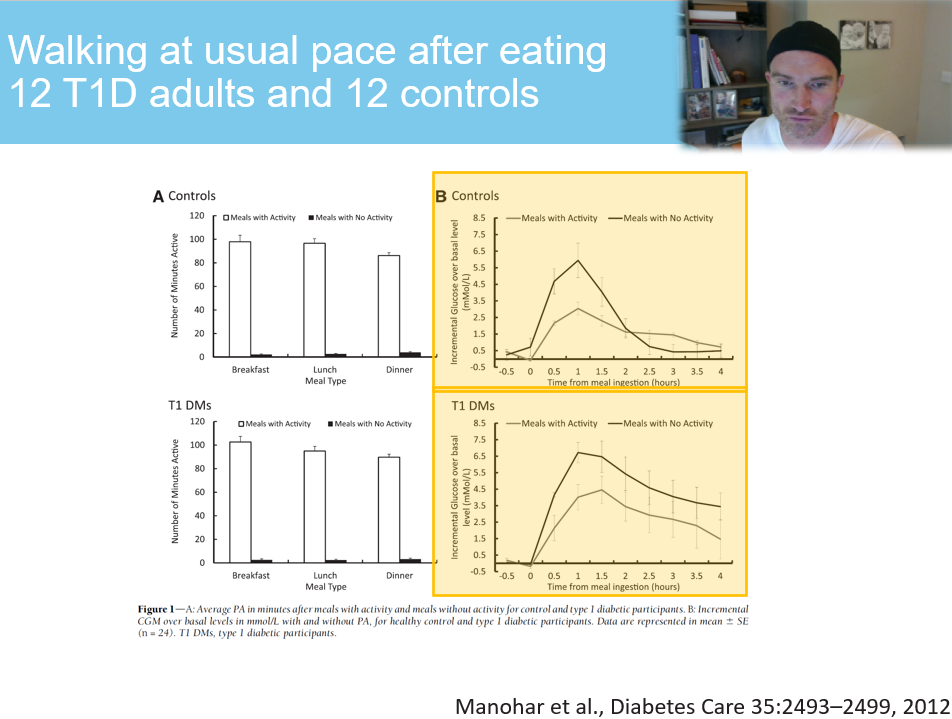
1. Food and insulin: 3 balanced meals with 10 minutes of activity after = (minutes 0–4)
2. High fat and protein meals: “Find out before you fiddle” then 25% extra insulin increments = (minutes 4–10)
3. After meal spikes: Insulin 15 minutes before in the abdomen or arm = (minutes 10–14)
4. 3 every 30: 3 minutes of movement every 30 minutes sitting = (minutes 14–16)
5. 10 by 2: 10 minutes of activity drops glucose by ~2 mmol/L (≈35–40 mg/dL) between meals = (minutes 16–22)
6. 50/50/20: Exercise insulin reductions for injections and standard pump therapy = (minutes 22–30)
7. T25/T25: Exercise insulin reductions for AID therapy = (minutes 30–38)
8. CGM: SLO ARSE: Slow and Low, Oil, Arm, Relax, Soft, Elevate = (minutes 38–40)
9. Site management: CAR – Change, Abdomen, Rotate = (minutes 40–41)
10. Does your CGM system need 70% or 75-80% time-in-range? = (minutes 41–50)
Here are the 10 tips summarised.
1. Food and insulin
- Strategy: Three balanced meals and 10 minutes of physical activity after each meal to enhance insulin effectiveness.
- Quote: “Putting in that 10 minutes of walking after eating really makes a huge difference on the glucose levels.”
- Details: The post-meal movement helps match the timing of peak rapid-acting insulin with glucose entering the bloodstream, smoothing out spikes.
- Extra tip: Consistency in meal timing and composition can stabilise glucose and make CGM patterns much easier to interpret.
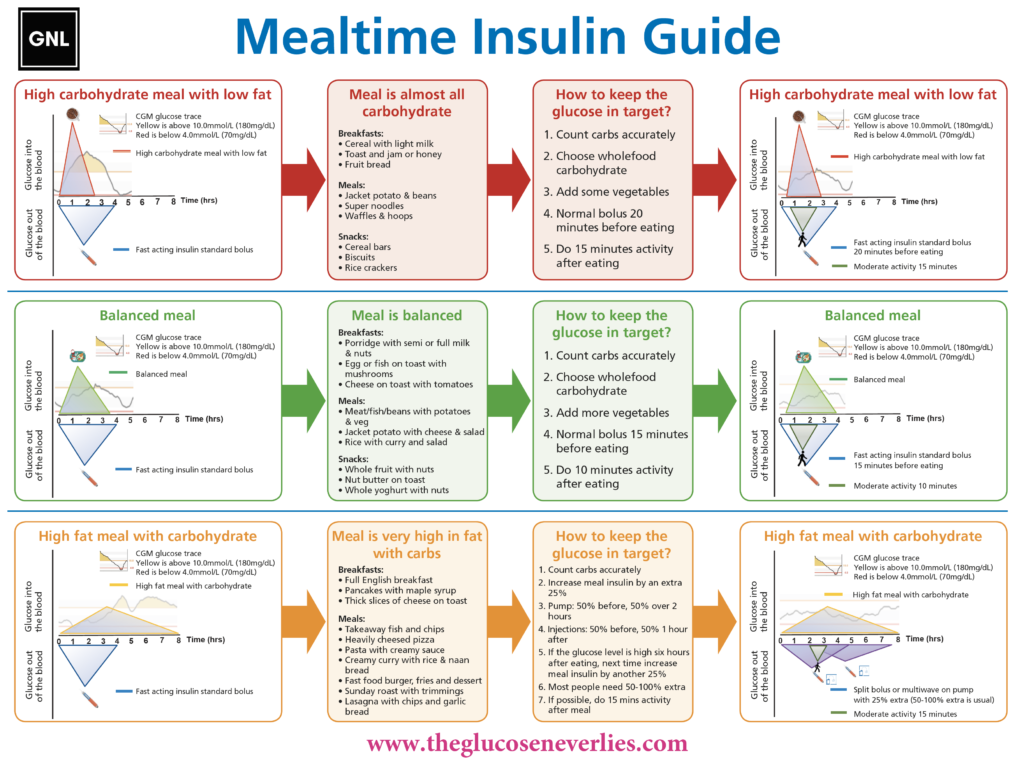
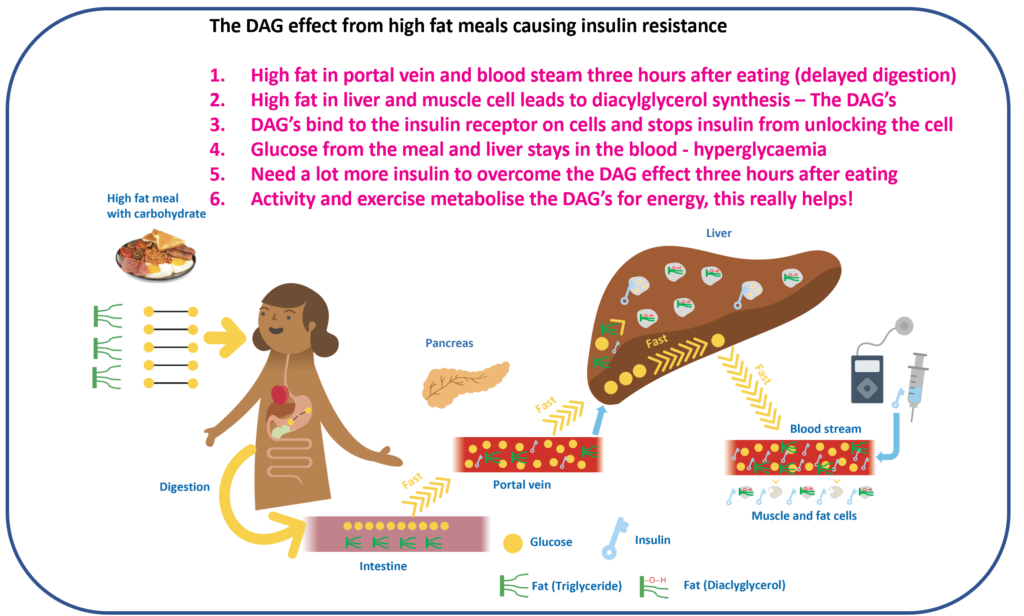
2. High fat and protein meals – “Find out before you fiddle”
Francesca Annan RD
- Strategy: Adjust insulin dosing for high-fat, high-protein meals.
- Quote: “Find out before you fiddle” – and consider ~25% extra insulin increments if needed.
- Details: Fat delays gastric emptying and can induce insulin resistance, often requiring more insulin over a longer period.
- Extra tip: Use your CGM to “learn your response”. Watch the 3–6 hour post-meal window and adjust future doses based on your own patterns.
3. After meal spikes
- Strategy: Take rapid-acting insulin about 15 minutes before eating to reduce post-meal spikes.
- Quote: “Where is the fastest place for absorption for your insulin? The belly… not far behind is the arm.”
- Details: Pre-bolusing and using faster-absorbing sites improve alignment between insulin action and glucose rise.
- Extra tip: Rotate injection / pump sites between abdomen and arm to maintain good absorption.
4. 3 every 30
- Strategy: Take 3 minutes of light movement every 30 minutes of sitting.
- Quote: “Every 30 minutes they got up to walk around at a normal pace for three minutes… Time in range improved by 14%.”
- Details: Regular breaks reduce insulin resistance and help CGM time in range without changing insulin doses.
- Extra tip: Set phone or watch reminders. This benefits everyone, not just those with T1D.
5. 10 by 2 mmol/L (or ~10 by 40 mg/dL)
- Strategy: Use brief activity to quickly lower glucose between meals.
- Quote: “Ten minutes will drop the glucose level by two… or 10 will drop you by about 40 milligrams per decilitre if you’re in those units.”
- Details: A short walk or similar light activity can reduce mild highs without extra insulin, particularly helpful if you still have insulin on board.
- Extra tip: Tailor intensity and timing to your fitness, medication, and hypo risk.
6. 50/50/20 – exercise adjustments for injections and standard pump therapy
- Strategy: Use a structured framework for insulin reductions around exercise when on MDI or standard pump therapy.
- Quote: “50/50/20… 50% insulin reductions for meals before (within 2 hours) and after, and 20% reductions of insulin overnight – or 20 g of carbs or 20 g protein.”
- Details: Exercise with rapid-acting insulin on board is a high-risk time for hypos. Planned dose reductions and snacks greatly reduce that risk.
- Extra tip: If you have had a bolus in the last 3 hours, assume glucose is likely to drop with moderate activity.
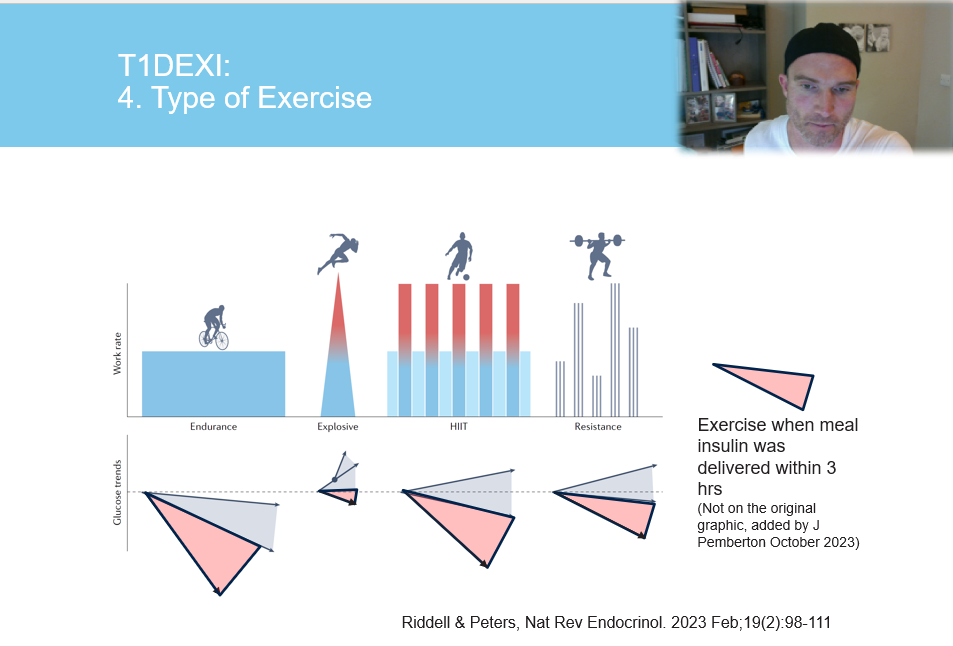
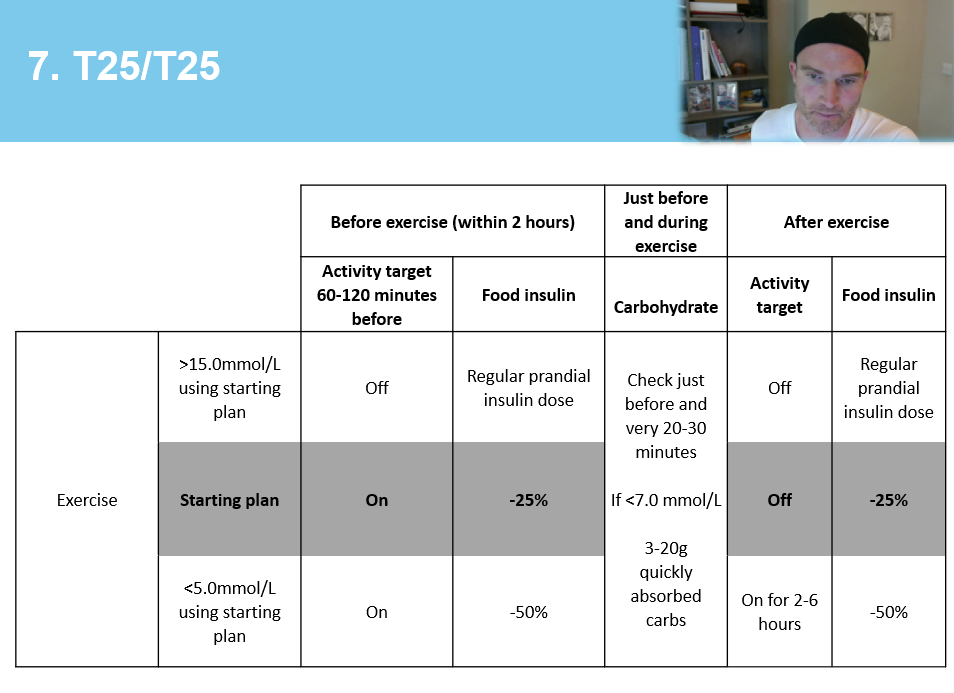
7. T25/T25 – exercise adjustments for AID therapy
- Strategy: For AID users, adjust insulin dosing and targets by 25% around exercise.
- Quote: “The first T25 is the two hours before exercise – aim for a 25% reduction for meals within two hours and start the exercise target 1–2 hours before. The second T25 is stopping the exercise target once you finish, and considering a 25% reduction for the meal after.”
- Details: Algorithms are powerful but not magic. They still need help around large changes like exercise.
- Extra tip: Use your CGM trend arrows aggressively here – and adjust future plans based on your patterns.
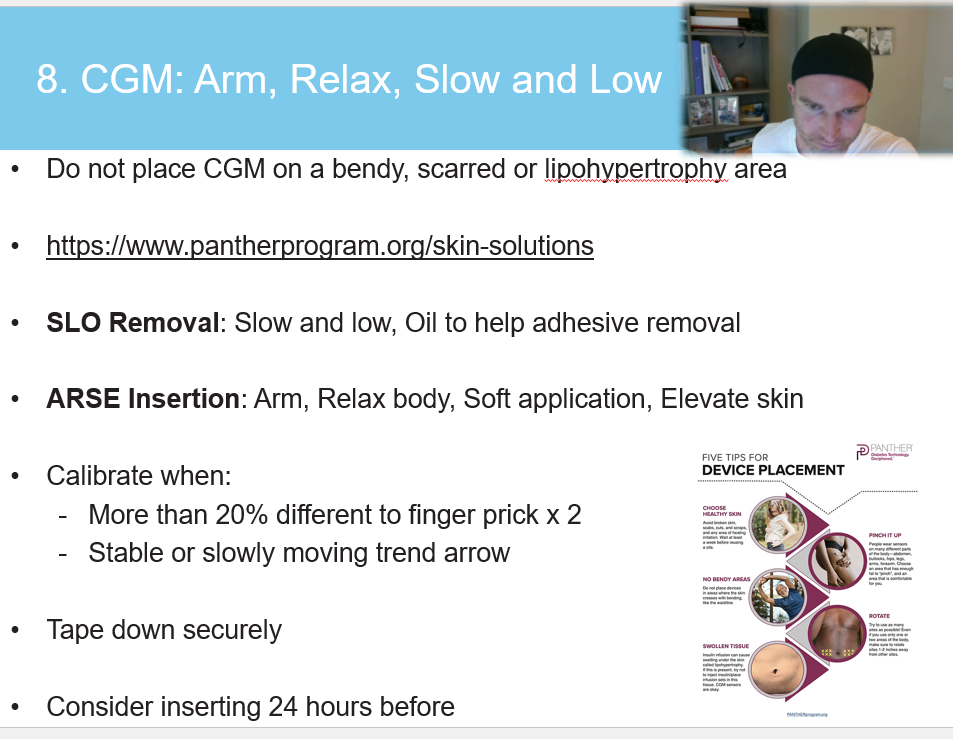
8. CGM management – SLO ARSE
- Strategy: Use the SLO ARSE approach for better sensor sites and fewer failures.
- Quote: “Slow and low is the key… Relax your arm, make sure it’s applied softly and elevate the skin off the muscle.”
- Details: Technique, skin prep, and site choice all affect accuracy and sensor life.
- Extra tip: If possible, insert the sensor a day before “going live” to improve first-day accuracy.
9. Site management
- Strategy: Rotate infusion / injection / sensor sites to maintain good absorption and skin health.
- Quote: “Change every two to three days and look after your skin as you go along. Rotate where you do the sites.”
- Details: Lipohypertrophy and scar tissue can significantly blunt insulin absorption and distort CGM readings.
- Extra tip: Use a simple rotation map or chart and actually tick off zones as you go.
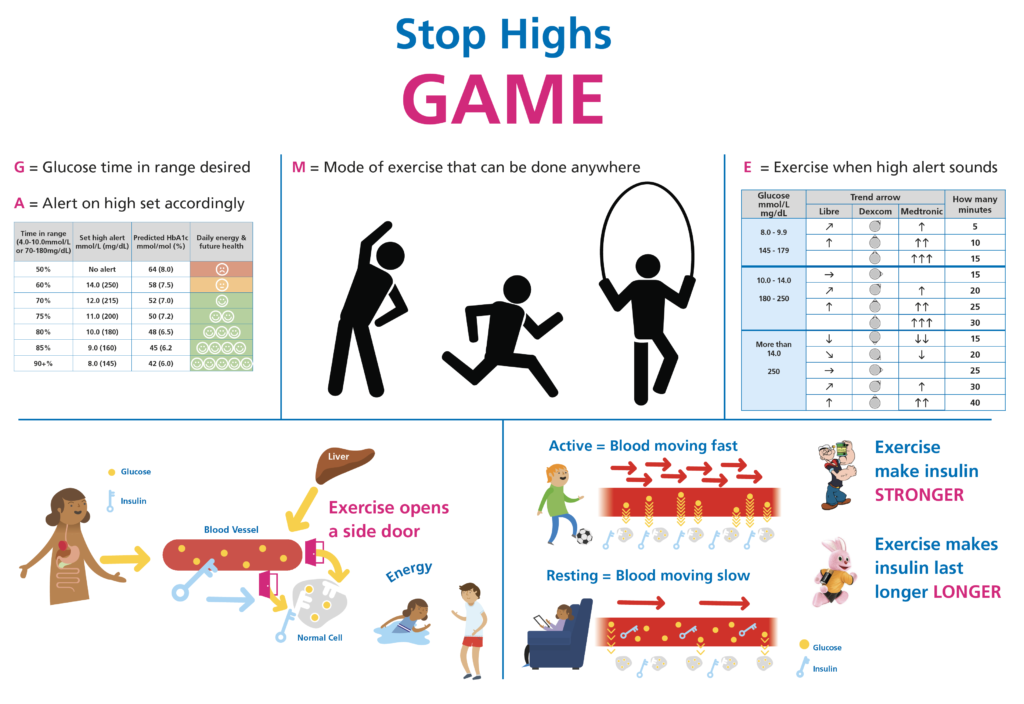
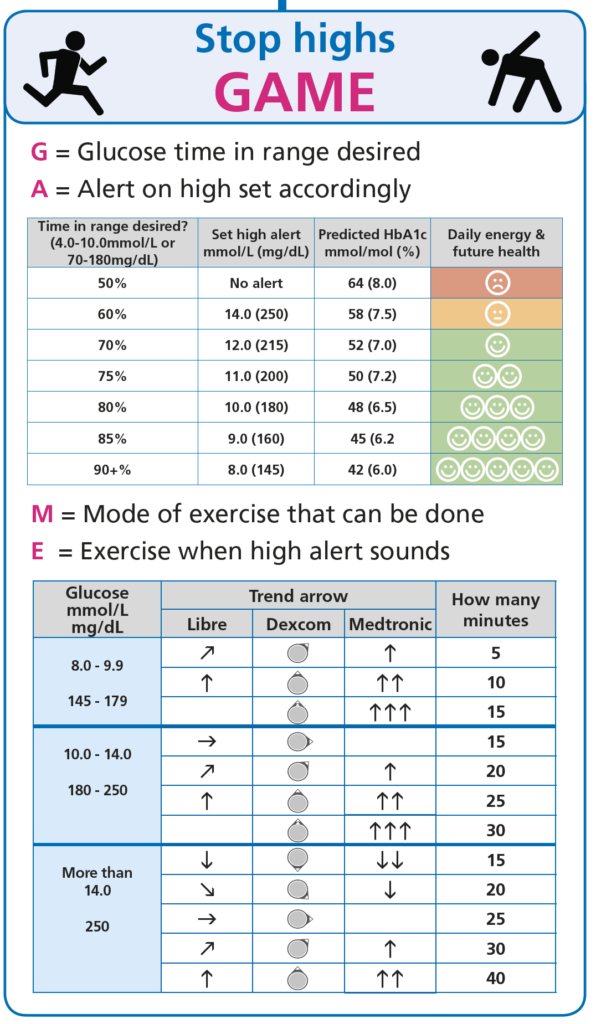
10. Does your CGM system need 70% or 75-80% time-in-range
Depends on which Zone your CGM system reads in.
CGM systems reading in Zone P
These systems, on average, read with physiological glucose exposure and for these, 70% TIR is the target.
| Device | Manufacturer | Bias to Venous Blood Glucose (when above 10.0 mmol/L or 180 mg/dL) | Comparator |
|---|---|---|---|
| FreeStyle Libre 2 / 2 Plus / 3 / 3 Plus | Abbott | +5% | Venous |
| Dexcom G7 / ONE+ | Dexcom | +5% | Arterialised Venous |
| Dexcom G6 / ONE | Dexcom | +2% | Arterialised Venous |
| Accu-Chek SmartGuide | ROCHE | +2% | Capillary |
CGM systems reading in Zone B
These systems, on average, read below venous glucose. This often results in higher TIR values that underreport true physiological glucose exposure. 75–80% TIR is the target.
| Device | Manufacturer | Bias to Venous Blood Glucose (when above 10.0 mmol/L or 180 mg/dL) | Comparator |
|---|---|---|---|
| Eversense E3 / 365 | Senseonics | −2% | Venous |
| MimMed Simplera / Guardian 4 | Medtronic | −10% | Venous |
Conclusion
Implementing these strategies can significantly improve glucose control for people using CGM systems. Each tip is a lever: some are behavioural (food, movement, exercise), some are technical (sites, sensors, meters), and some are about understanding how your CGM measures glucose in the first place.
Next up:
They are in order, but take your pick: