
Type 1 diabetes only. This is the Foundations hub. Start with this page, then work through the sequence below. The order is recommended — but you can jump to what you need.
Foundations sequence
- This page: What is Type 1 diabetes?
- Continuous glucose monitoring (CGM)
- Basal insulin
- Bolus insulin
- Correction insulin
- Carbohydrate counting
- Three balanced meals
- Hypoglycaemia
- Measuring success
What is Type 1 diabetes?
- Podcast: Episode 7: Fundamentals of The Glucose Never Lies
- YouTube: watch the video below.
- Or read on.
Before you got Type 1 diabetes
Here’s what glucose and insulin regulation looks like in people without diabetes:
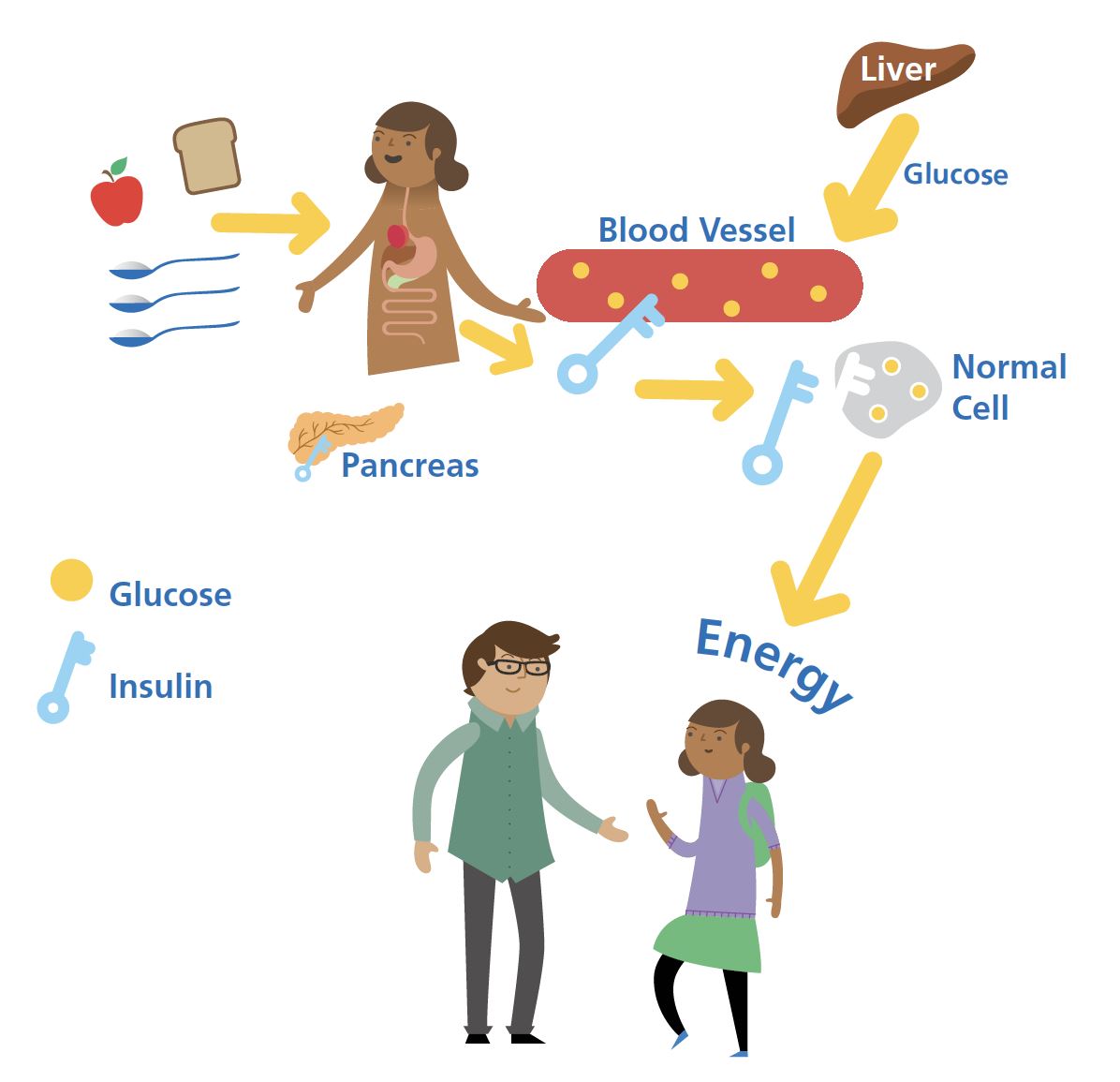
Key things:
- Glucose enters the bloodstream from food; carbohydrate has the biggest impact. (See: carbohydrate counting.)
- Glucose stored in the liver is steadily released into the bloodstream 24 hours a day.
- Insulin from the pancreas works like a key, opening the cell to let glucose in.
- Glucose in the cell is used to produce energy.
- Blood glucose is tightly regulated between 3.3–6.7 mmol/L (60–120 mg/dL).
- If glucose drops to ~3.3 mmol/L (60 mg/dL), insulin output slows.
- If glucose rises to ~6.7 mmol/L (120 mg/dL), insulin output increases.
What causes Type 1 diabetes, and what happens next
For reasons that are not entirely clear, your immune system attacks the insulin-producing beta cells in the pancreas. This is autoimmunity — friendly fire.
Very quickly, you go from producing enough insulin to regulate glucose to producing virtually none.
- It’s not your fault.
- There’s nothing you could have done to prevent it.
- The world is not conspiring against you.
- It’s the chaos of biology in an uncertain world.
Take time to grieve. Then we get to work.
Here are the consequences of no insulin:
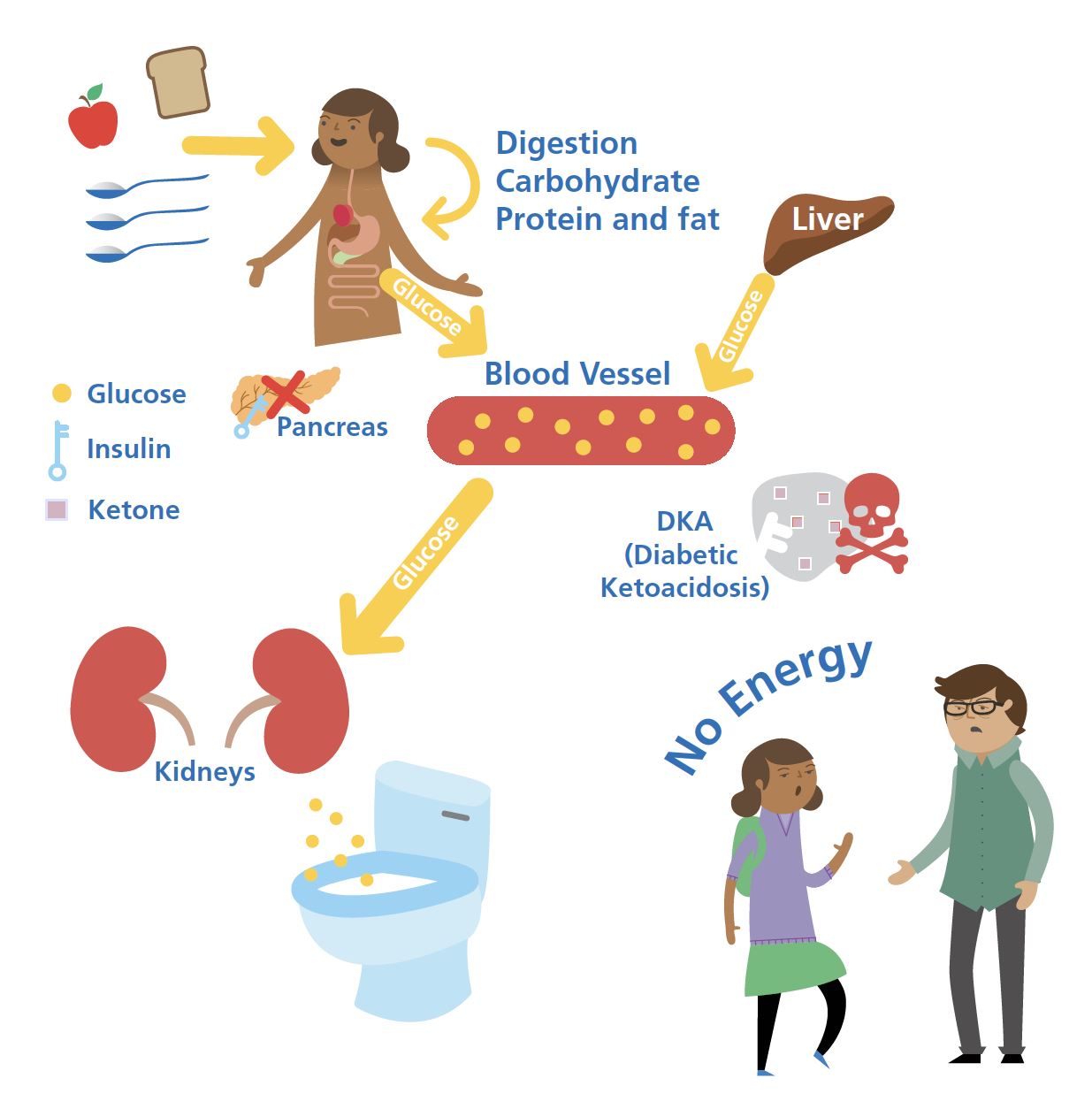
Key things:
- Glucose keeps entering the bloodstream from food and the liver.
- Without insulin, glucose rises well above 11.1 mmol/L (200 mg/dL).
- Cells switch to burning body fat for energy, causing weight loss.
- Fat burning produces ketones and acid build-up.
- Unchecked, acid levels can rise high enough to be fatal.
- The kidneys dump glucose into urine → frequent toilet trips.
- Fluid loss makes you thirsty.
- The “4 Ts” of new T1D: Toilet, Thirsty, Tired, Thinner.
Insulin to the rescue
Science keeps us alive. Insulin has given us the gift of life.
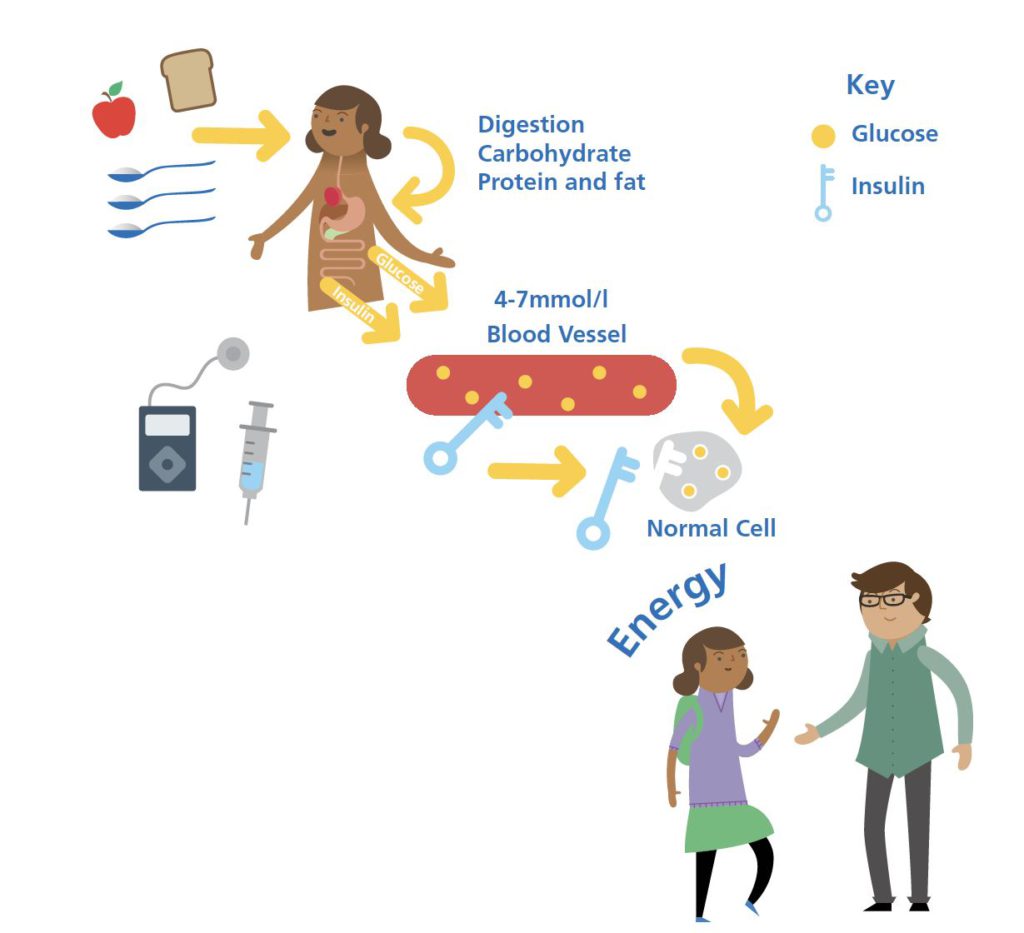
Key things:
- Injected or pumped insulin replaces what the pancreas can’t make. (Start here: basal insulin and bolus insulin.)
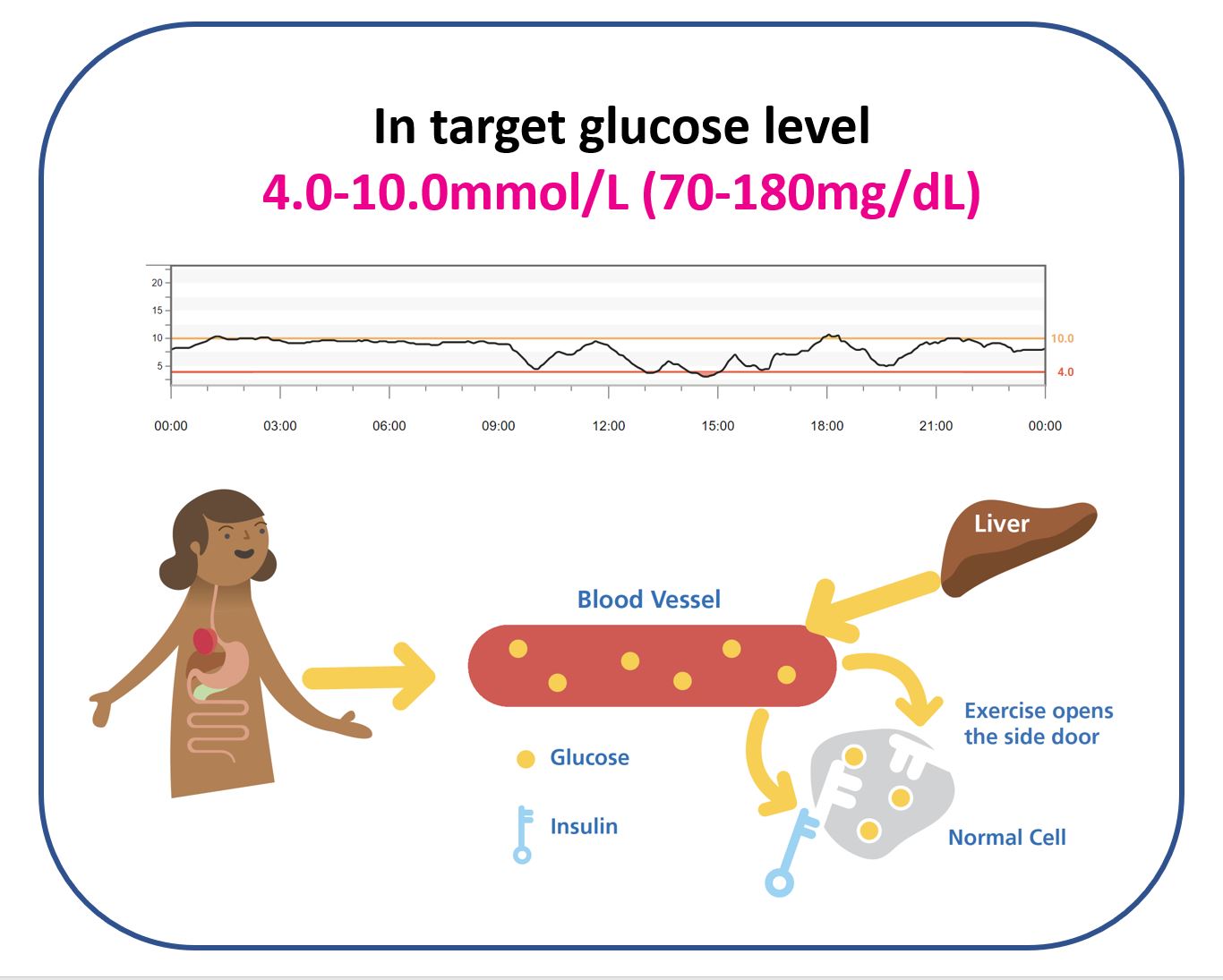
- The challenge is matching insulin to glucose from meals and the liver to stay roughly 3.9–10.0 mmol/L (70–180 mg/dL). (See: correction insulin.)
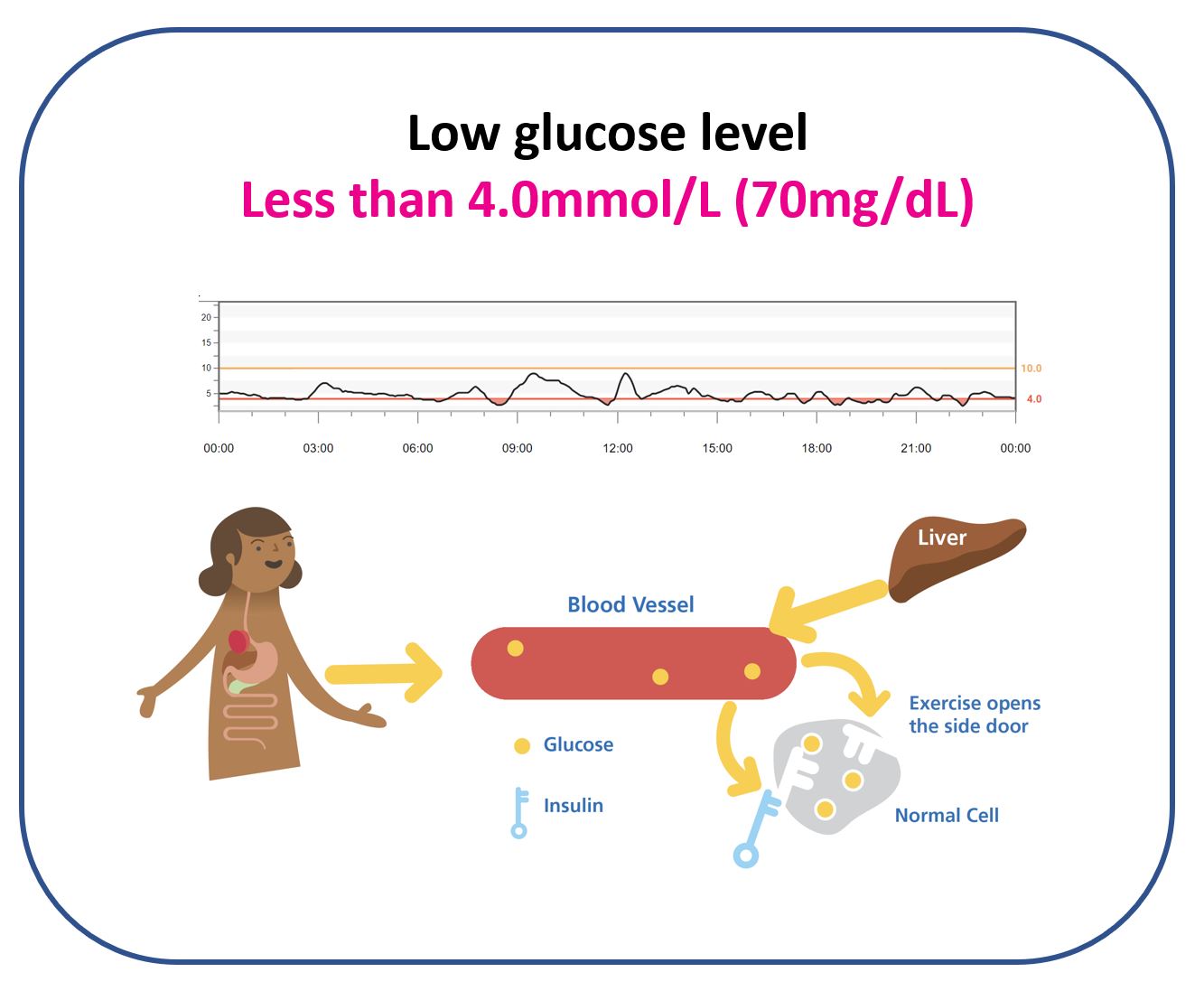
- Too much insulin or unplanned activity → glucose below 3.9 mmol/L (70 mg/dL): hypoglycaemia (a hypo).
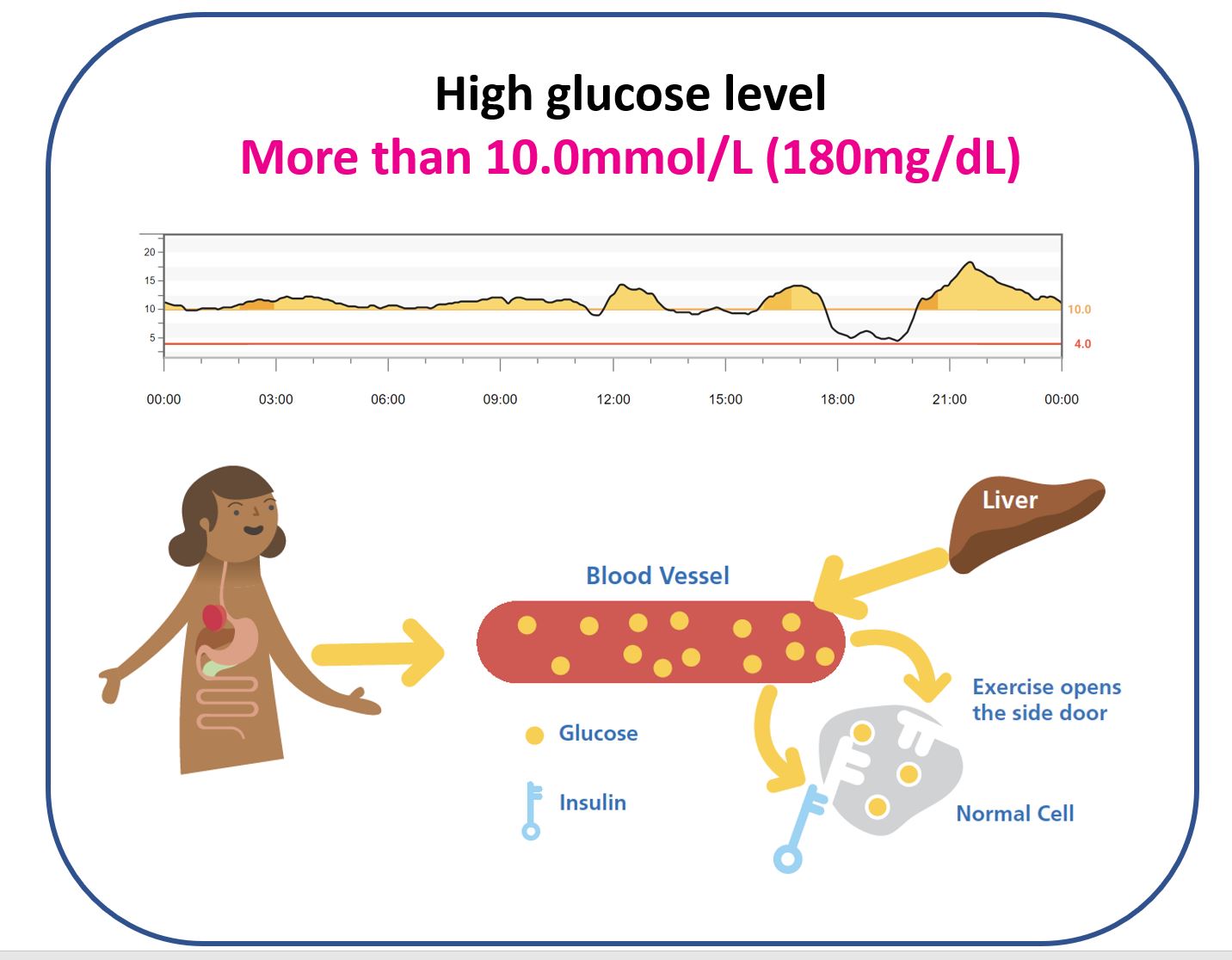
- Not enough insulin for food or liver output → glucose above 10.0 mmol/L (180 mg/dL): hyperglycaemia (a hyper).
- Counting carbohydrates and matching insulin to digestion is essential.
Practical
Read this section slowly. Then re-read it. The rest of the site assumes these ideas are already in your bones.
Next logical step: Continuous glucose monitoring (CGM)
Foundations / related content
The order shown below is recommended, but navigate as you see fit.