
It started as a passing observation. A child with white-coloured skin would come into clinic with a mean glucose of 10 mmol/L (180 mg/dL), a time in range (TIR, 3.9-10.0 mmol/L) of 50%, and their HbA1c would be around 64 mmol/mol (8.0%). Then the next child, this time with black-coloured skin, would come in with the exact same glucose metrics—mean glucose of 10 mmol/L (180 mg/dL), TIR of 50%—but their HbA1c would be 69 mmol/mol (8.5%).
At first, I brushed it off as natural variation. After all, HbA1c is an estimate, not an absolute. But then it kept happening. Again and again. Different kids, different families, same pattern. And the more I saw it, the more I got curious.
Then I caught myself. I was interacting with the families differently. When the white child’s HbA1c was 58 mmol/mol (7.5%) with a TIR of 60%, I never questioned the family and would congratulate them. But when the black child’s HbA1c was 64 mmol/mol (8.0%)—despite the same glucose data, a TIR of 60%—I found myself thinking, What are they doing wrong? What more do they need to do?
And there were consequences.
Because our clinic had an HbA1c cut-off of 69 mmol/mol (8.5%) for extra follow-up, the children with black coloured skin more often ended up in the high HbA1c clinic—meaning more appointments, more pressure, more time out of school, and more of that implicit message: you need to work harder.
But what if the issue wasn’t effort?
What if something else was at play?
Digging into the Data
That’s when I came across a paper by Professor Stuart Chalew and his team from Louisiana, and it was like reading a mirror image of what I was seeing in clinic. They described how, when controlling for mean blood glucose and TIR, people with black-coloured skin had HbA1c levels that were consistently about 4 mmol/mol (0.4%) higher than their white counterparts.
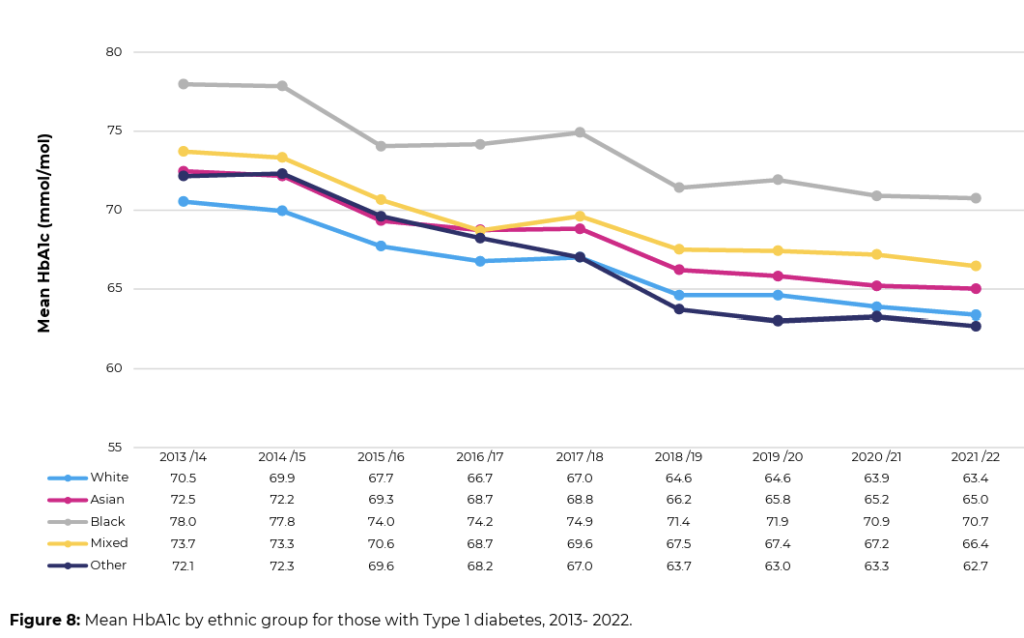
This wasn’t new. Research dating back nearly 20 years had pointed to this discrepancy, yet it had somehow never reached mainstream clinical practice. The UK’s national paediatric diabetes audit 2022/3 shows that children from black ethnic groups have, on average, an HbA1c 7 mmol/mol (0.7%) higher than the white group, that’s remained constant over 10 years, since the audit began.
The assumption?
The “poorer management” was due to reduced access to diabetes technology, lower socioeconomic status, or possibly differences in adherence.
Every study day I attended reported three causes!
Reduced access to diabetes technology, lower socioeconomic status, or possibly differences in adherence to treatment regimens, “not trying hard enough”.
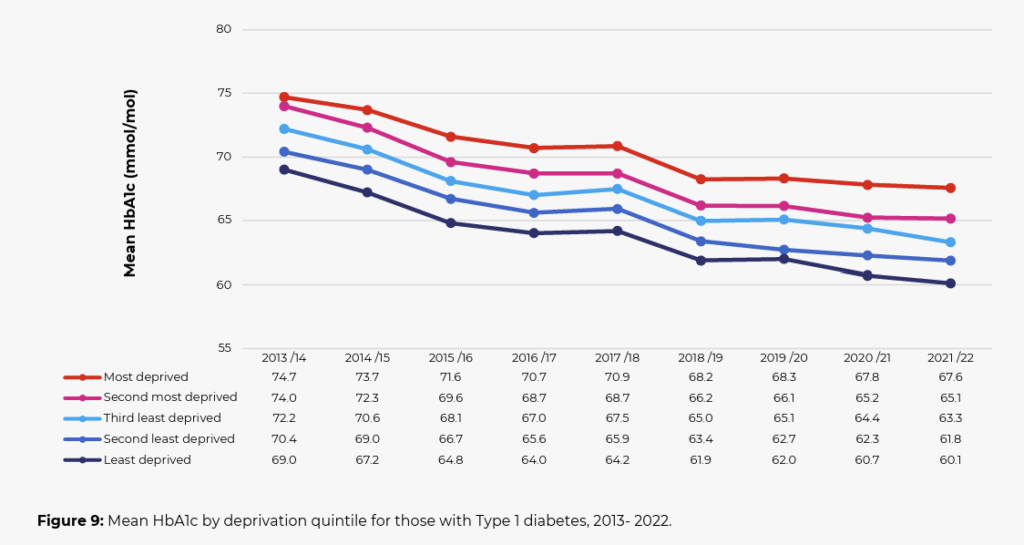
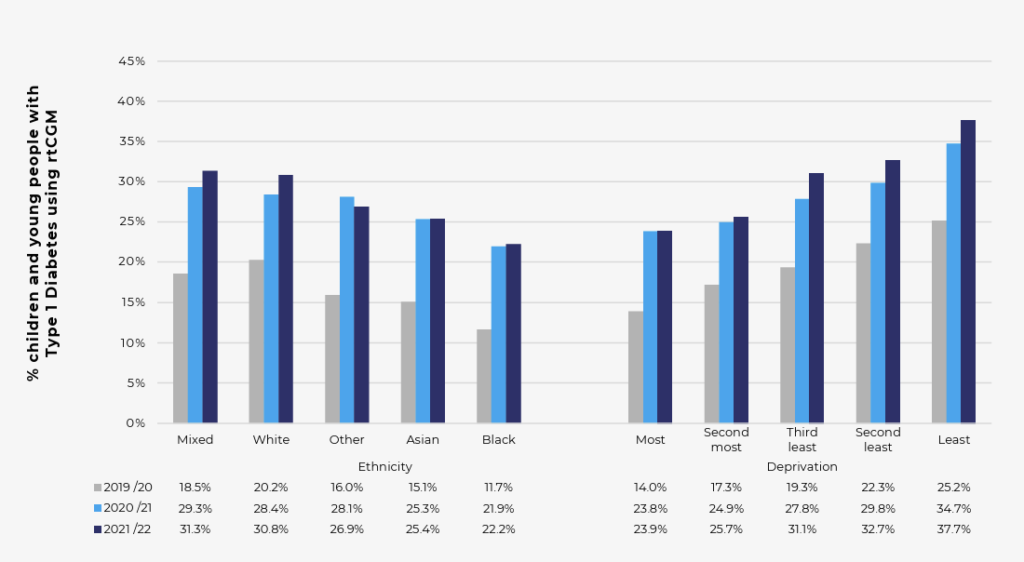
Two of these explanations appeared to have validity. Children from the Black ethnic group children, on average, live in the most deprived areas and are the last ones to get access to advanced diabetes technology such as CGM. Especially given that children from the most deprived backgrounds have, on average, an HbA1c 7 mmol/mol (0.7%) higher than those from the least deprived backgrounds. Additionally, both the most deprived groups and Black ethnic groups have the lowest rates of access to CGM, further reinforcing this assumption.
So the answer is clear, right?
But what if it wasn’t?
With our clinic data, we had an opportunity to test this. We looked at children and young people with type 1 diabetes, all of whom were using CGM and had been through our structured diabetes education programme, “The CGM Academy.” This was important because it levelled the playing field—everyone had access to the same technology, the same support, and had received the same education.
Then we compared their HbA1c to their glucose metrics in this 2025 publication.
The results were striking.
Mean glucose was still the strongest predictor of HbA1c—but only explained about 80-85% of the variation. The remaining 15-20%? That’s where ethnicity stood out like a sore thumb.
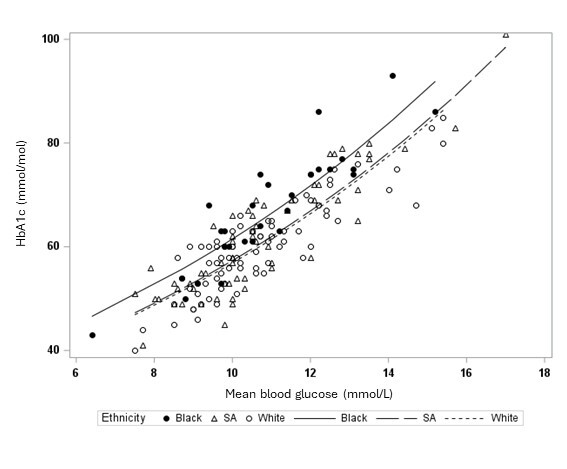
Children from Black ethnic groups had, on average, an HbA1c 5 mmol/mol (0.5%) higher than their White and South Asian peers—despite having the same glucose data. This difference was consistent across all glucose levels, as shown in the graph below.
We also investigated whether socioeconomic status played a role. It didn’t. It had absolutely no impact.
So, with equal access to technology and the same CGM glucose control, Black children still had a clinically significant higher HbA1c, at all glucose levels, as can be seen by the key graph!
What I was seeing in clinic wasn’t my imagination—it was real. And yes, this is deeply concerning.
And as if that wasn’t concerning enough, then we looked at hypoglycemia rates.
The Double Jeopardy Effect
If you see a child with an HbA1c of 69 mmol/mol (8.5%) in clinic, you’re going to push for tighter control. That’s what we’re trained to do.
Why, because the national diabetes audit measures diabetes teams performance by what?
You guessed it, HbA1c!
But what if HbA1c doesn’t truly reflect glucose levels?
What could the consequences be for those with higher HbA1cs for the same CGM glucose levels?
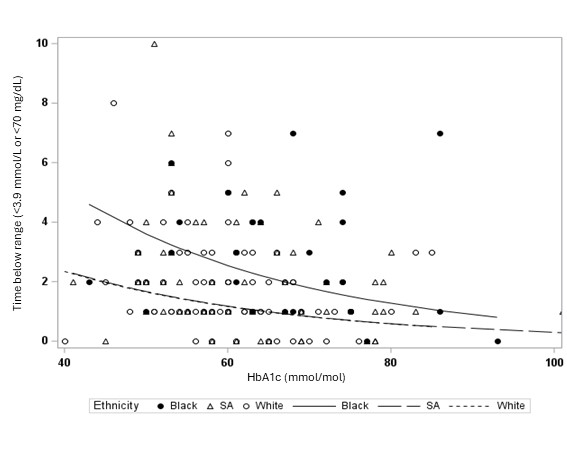
We found, for the same HbA1c, children from Black ethnic backgrounds experienced more hypoglycemia than their White and South Asian peers.
For example, at an HbA1c of 58 mmol/mol (7.5%), Black children spent ~4% of their time with glucose levels below 3.9 mmol/L (<70 mg/dL), whereas their White and South Asian counterparts spent less than 2% in that range with the exact same HbA1c. The increase hypo rates was evident at all HbA1c levels (see graph below)!
That means double the hypo rates—a clear case of double jeopardy.
Why?
Because it’s very likely our team—including myself—was pushing insulin doses harder for children with black-coloured skin, aiming to lower their HbA1c and improve clinic performance on the NPDA league tables. The goal was to reduce long-term complication risks, but in doing so, we may have been increasing their immediate risk of hypoglycemia.
Simply, it’s extremely likely the same child, with the same HbA1c, but black-coloured skin, was more likely to have their insulin doses increased, putting them at greater risk of hypos.
It’s a vicious cycle.
Higher HbA1c → More clinical pressure → More aggressive insulin adjustments → More hypoglycemia → More stress → More unpredictability.
And if you’ve ever had a severe hypo, you’ll know that they’re terrifying. It’s not just a number on a screen—it’s real. And it shakes confidence, not just for the child but for the whole family.
What Do We Do With This?
1. Stop Using HbA1c as the primary metric to drive insulin intensification. This study, alongside others, confirms that for children with black heritage, HbA1c overestimates their glucose levels. If we have CGM data available, we need to use it first before jumping to conclusions based on HbA1c alone.
2. Be Careful with HbA1c Cut-offs. If we set rigid HbA1c thresholds for intervention (like 64 or 69 mmol/mol for extra clinic visits), we risk unfairly penalising the children from the Black ethnic group. Again, use TIR cut-offs, <50% perhaps, as this is directly controllable, HbA1c is not! More importantly, avoid thinking higher HbA1c = “lack of adherence or effort” when the TIR is in a range that suggests effective management for the there they are using.
3. Prioritise Access to Advanced Diabetes Technologies. If children from black ethnic backgrounds are at greater risk of both high HbA1c and hypoglycemia, then they are precisely the group that should be prioritised for automated insulin delivery (AID) systems and emerging adjunct therapies like GLP-1 receptor agonists, which help stabilise glucose levels.
Oh yeah, the national audit, what to do?
Should we be using Time in Range (TIR) rather than HbA1c for the National Paediatric Diabetes Audit (NPDA) data? Or at the very least, alongside it?
Based on HbA1c differences, we would expect White children to have an average TIR of 60%, while Black children would be closer to 50%. However, in reality, Black children are likely closer to 57%—meaning their glucose control is better than their HbA1c suggests.
If technology access were equal, we’d likely see all groups at 60% TIR, but the HbA1c levels of the Black group would be 4-5 mmol/mol (0.4-0.5%) higher than the other ethnic groups! Consider, that while technology access accounts for about a third of the HbA1c gap, the vast majority is driven by ethnicity-related factors—completely beyond the control of children with Black skin.
Final Thoughts
For years, I have operated on the assumption that higher HbA1c means higher average glucose. Like many who work in the diabetes field!
But it’s not that simple.
For some children, particularly those from black ethnic backgrounds, HbA1c is systematically overestimating their glucose levels, leading to over-treatment, more hypos, more clinic burden, and more penalising of the family with extra visits – perhaps a triple jeopardy!
It’s time we do better.
This isn’t about preferential treatment. It’s about equitable treatment—understanding that the tools we use in diabetes care aren’t always perfect, and ensuring we don’t make things worse by applying them blindly.
HbA1c is useful—but it’s not gospel. And when it comes to treating children and young people fairly, the CGM glucose never lies.
Cheers
John
T1D since 2008
Dad of Grace and Jude who The Glucose Never Lies is written for!