Foundations, Part 6
Carbohydrate Counting
Carb counting is one of the core skills in type 1 diabetes. It helps you estimate the glucose load of a meal so you can calculate a bolus that gets you into the right ballpark. The real teaching lives in the interactive guide; this page gives you the overview, the practical tools, and an honest look at what counting can and cannot do.
Ask Grace
Want to ask how carb counting works for the meals you actually eat? Ask Grace.
The interactive carb counting guide
This might surprise you: despite being written by a diabetes dietitian, this is one of the shorter pages on the site. That is because the detailed teaching lives in the Interactive Carb Counting Guide (PDF).
Once you have worked through it, carb counting tends to become straightforward, and you can calculate your bolus insulin accurately enough to act, then refine using real-world CGM patterns.
The interactive guide is packed with videos, worked examples, and short tests. Complete it, and you will be able to:
- work out the carbohydrate content of any meal,
- calculate your meal bolus,
- then adjust intelligently using CGM trends and experience.
Prefer video? The carb counting video walkthrough is available on the GNL YouTube channel.
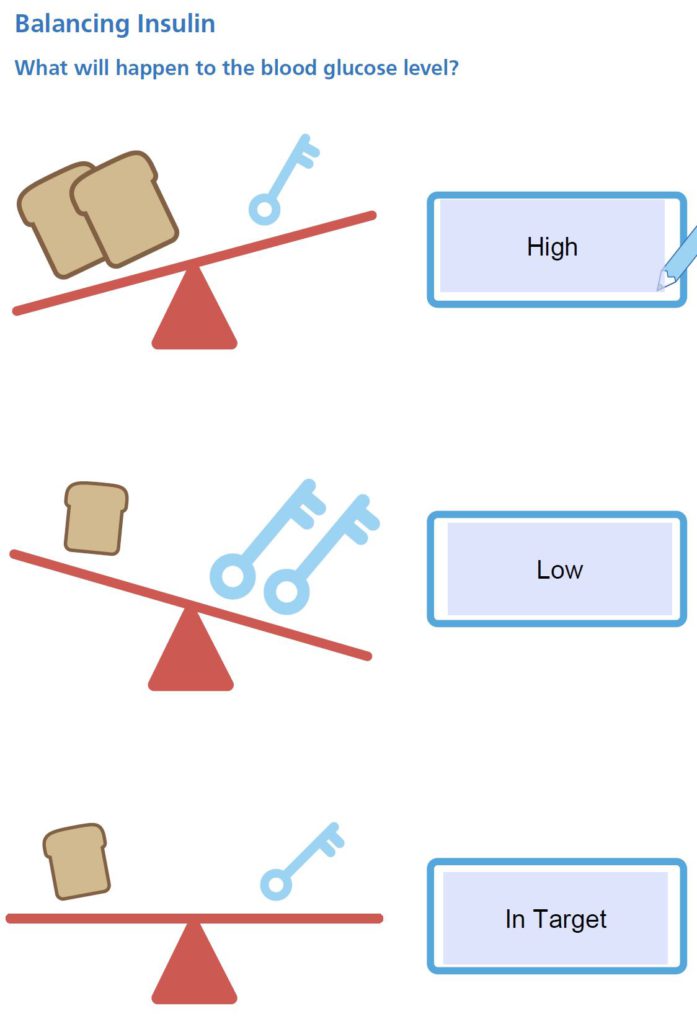
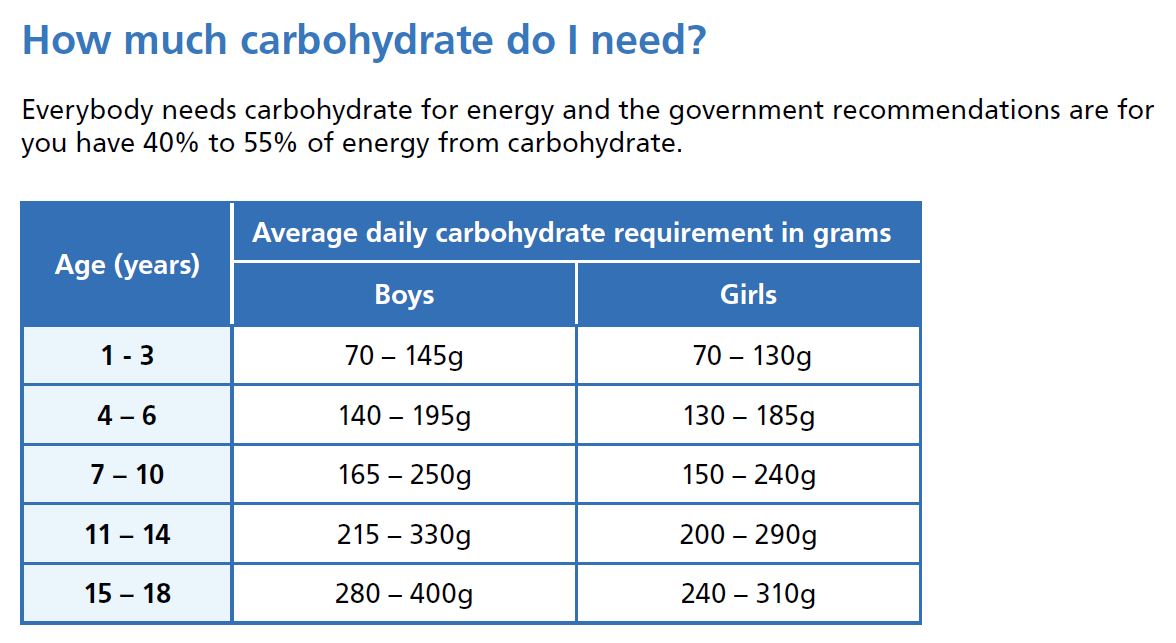
What to count, and how much
Here is a taster of what the interactive guide covers.
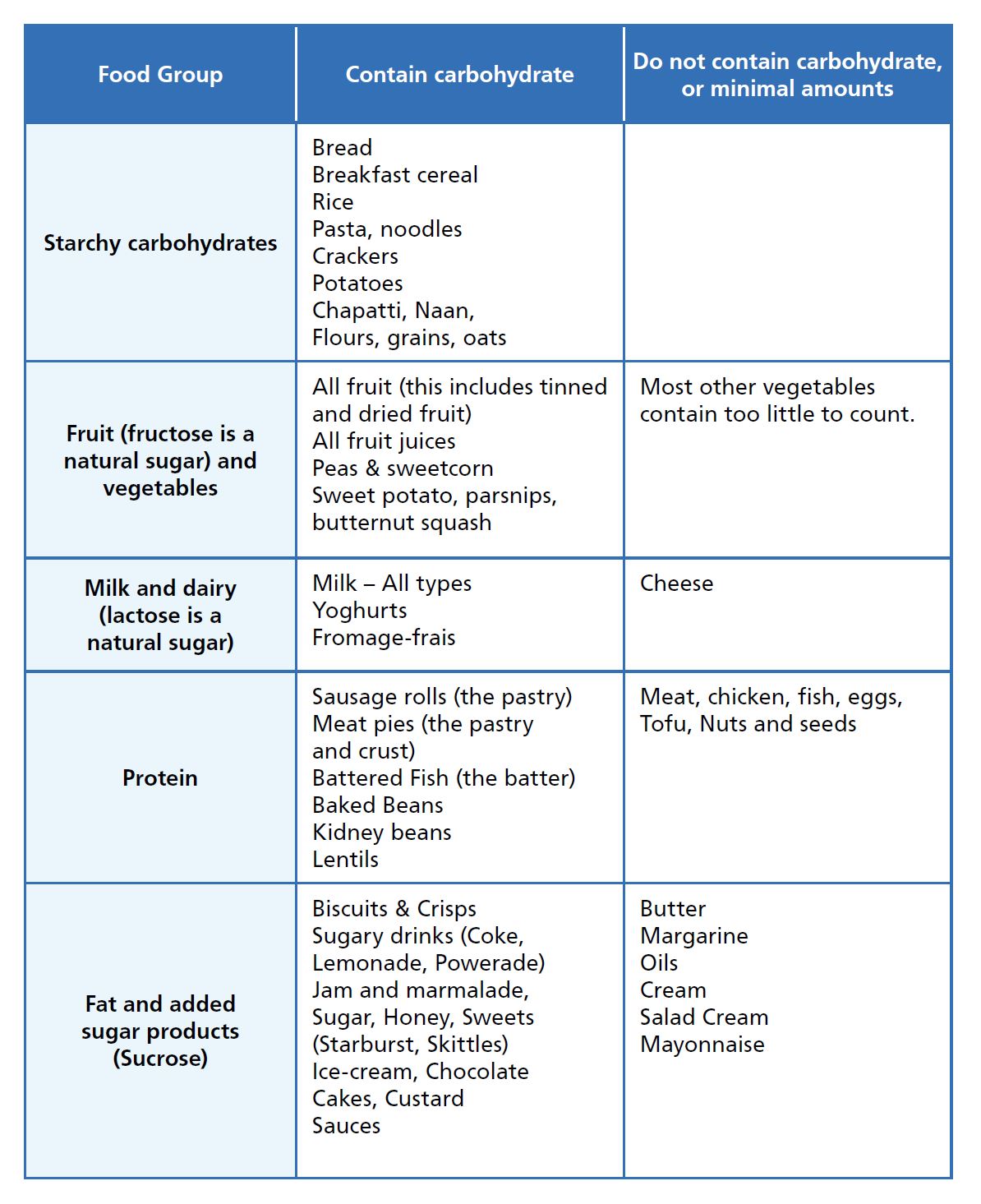
Working out carbs in real life
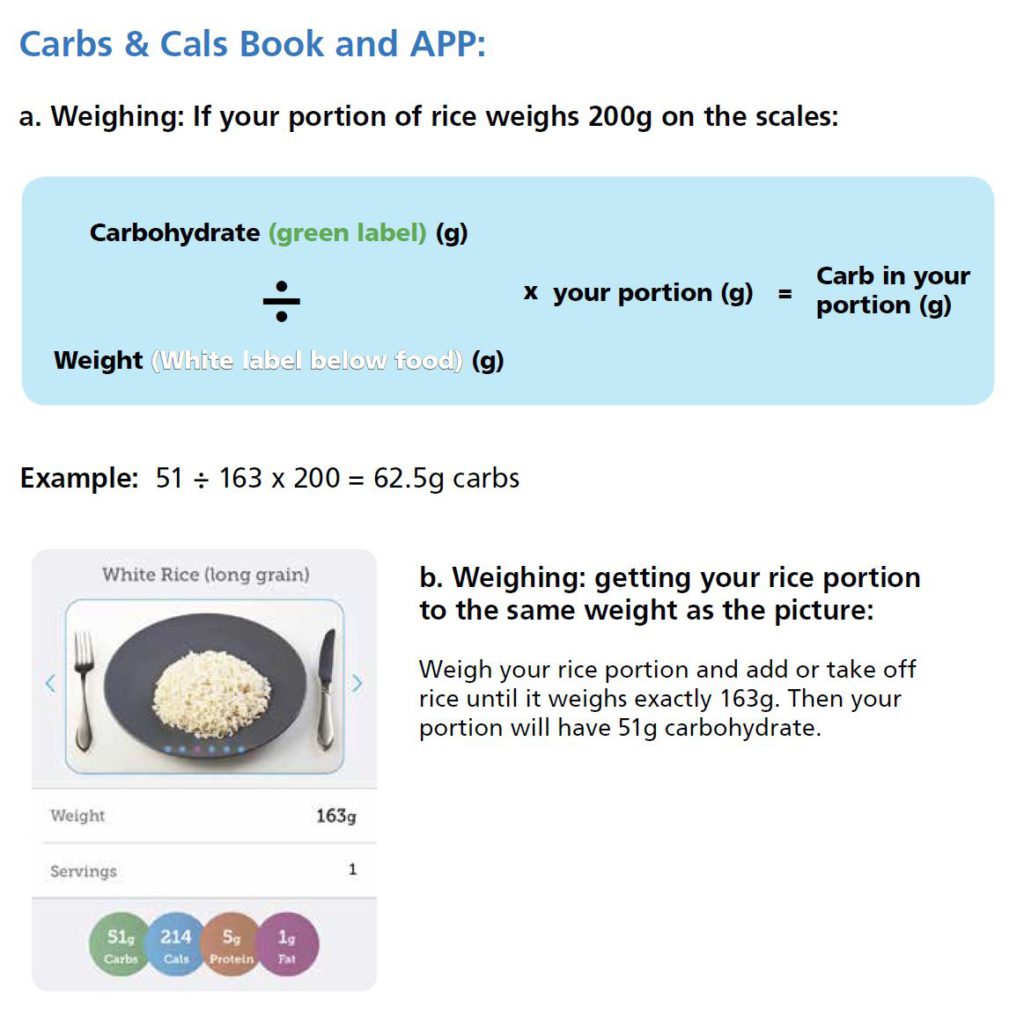
Using Carbs and Cals resources
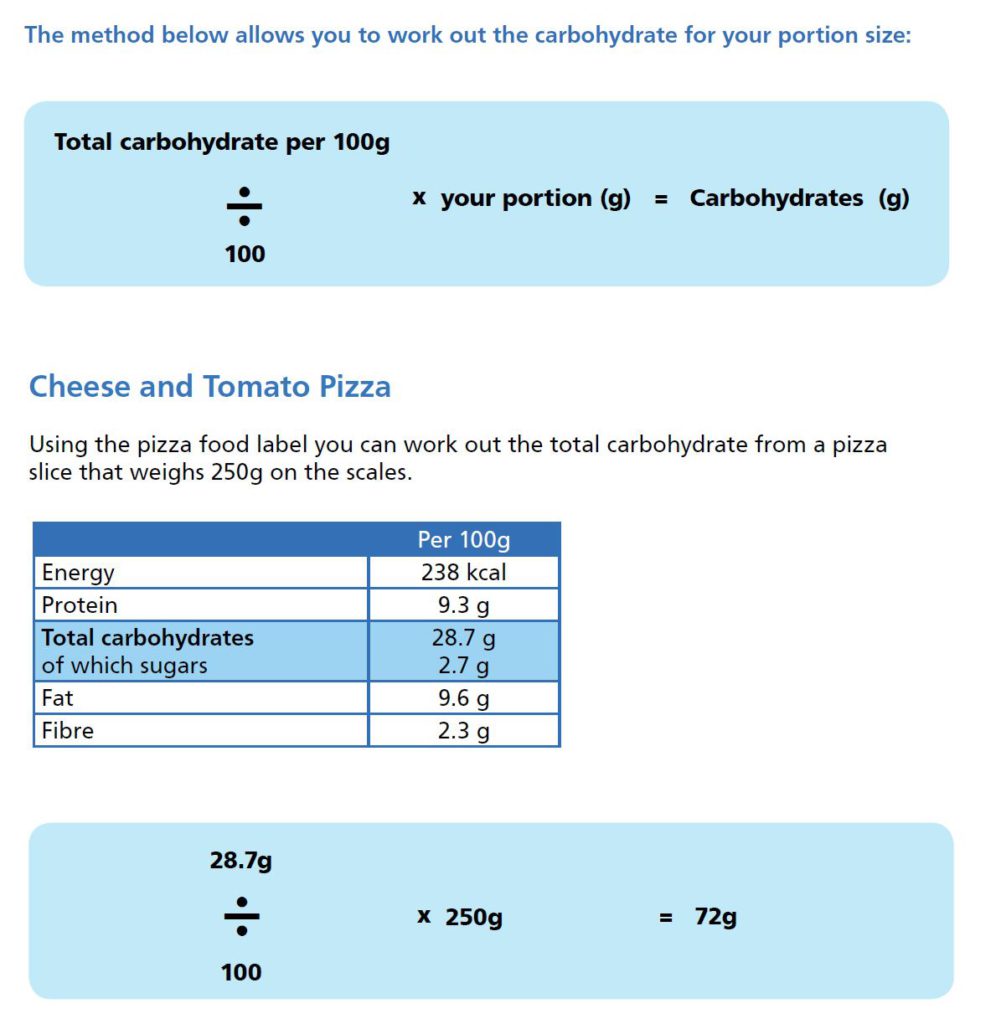
Reading a food label
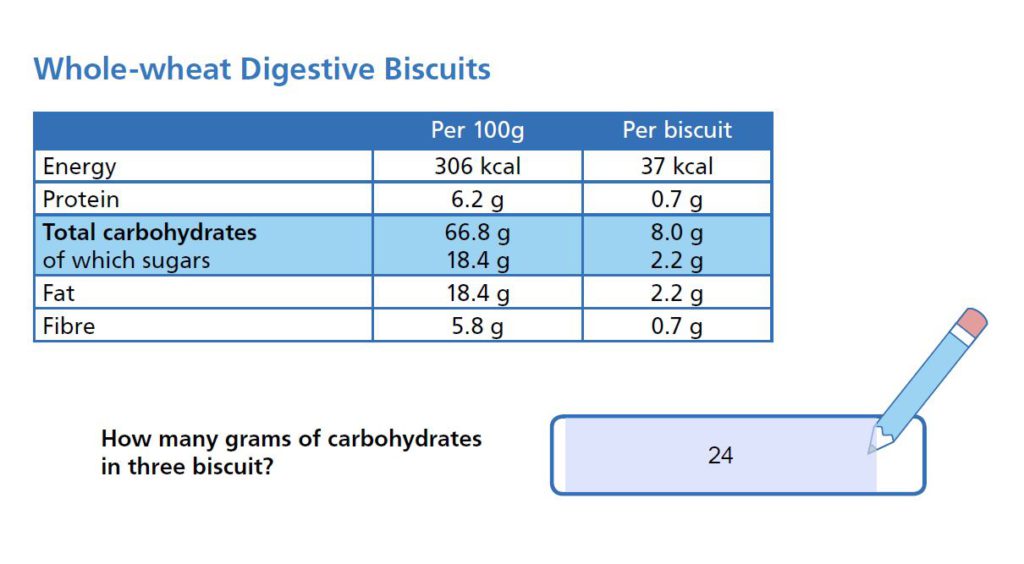
Using labels expressed per 100 g
An honest take on carb counting
The pros
- It helps you calculate a meal bolus that is close enough to the glucose you are about to absorb.
- It is simple and teachable to family members.
- Children can get involved in insulin decisions early, which tends to build skill and confidence over time.
The cons
- The key message of three balanced meals often gets replaced by “eat what you like, just count and dose”, which many people find is reductive and usually backfires.
- On its own, counting is too simplistic.
- It can create false certainty: you can count perfectly and still get it wrong.
- It ignores the insulin-resistance impact of high-fat meals and other factors covered in the Mealtime Insulin Guide.
- It tends to nudge people towards processed food because it is easy to count, not because it is good for them.
What this means in practice
Carb counting is a foundation skill; it works best when combined with a reliable meal structure, an understanding of fat and protein effects, and feedback from CGM. Counting alone rarely tells the whole story.
The mechanism is straightforward: the more repeatable the meal, the more predictable the glucose response, and the easier it becomes to refine over time. This is worth exploring with your care team if meals that “should work” on paper keep producing surprises on CGM.
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Want to go deeper? The evidence base behind the page
The carb counting principles here sit on a wider evidence base. The practical-rule layer for what to do at the meal lives in the Mealtime Insulin Guide. The trial spine that anchors it (DAFNE in adults, the Bell fat-and-protein work, the pre-bolus timing literature, the AID-era simplified meal announcement studies, the careful place for low-carb eating in adult T1D) sits behind Grace.
Ask Grace for the depth on any one strand. Open Grace and try: “What does the Pack 8 evidence say about pre-bolus timing?”, “What is the FPU method and how strong is the evidence?”, “What does Bell 2020 actually show for high-fat meal dosing?”. Every numerical figure on this page is a population-average estimate; your own carb-to-insulin ratios and correction factors should be agreed with your diabetes care team.
Carbohydrate Counting Knowledge Check
You have worked through carb counting, the skill that makes bolus insulin usable. A short assessment checks it has stuck, and 9 out of 10 earns your certificate.
Part 6 of 12
Carbohydrate Counting