Foundations, Part 4
Bolus Insulin
Lunch on the table, glucose 6.4 mmol/L with a flat arrow. You bolus, count to twenty, then start eating. Ninety minutes later the trace shows a spike anyway. The gap is two timings that do not match: glucose arrives in minutes, insulin from a pen or pump arrives in hours. The rest of this page is what to do about it.
Ask Grace
Want to ask about pre-meal timing, carb ratios, or why your post-meal still spikes? Ask Grace.
What bolus insulin covers
Bolus insulin means delivering fast-acting insulin to cover:
- Glucose from digested carbohydrate, a meal bolus.
- Bringing a high glucose level back towards target, a correction bolus.
- Or both combined.
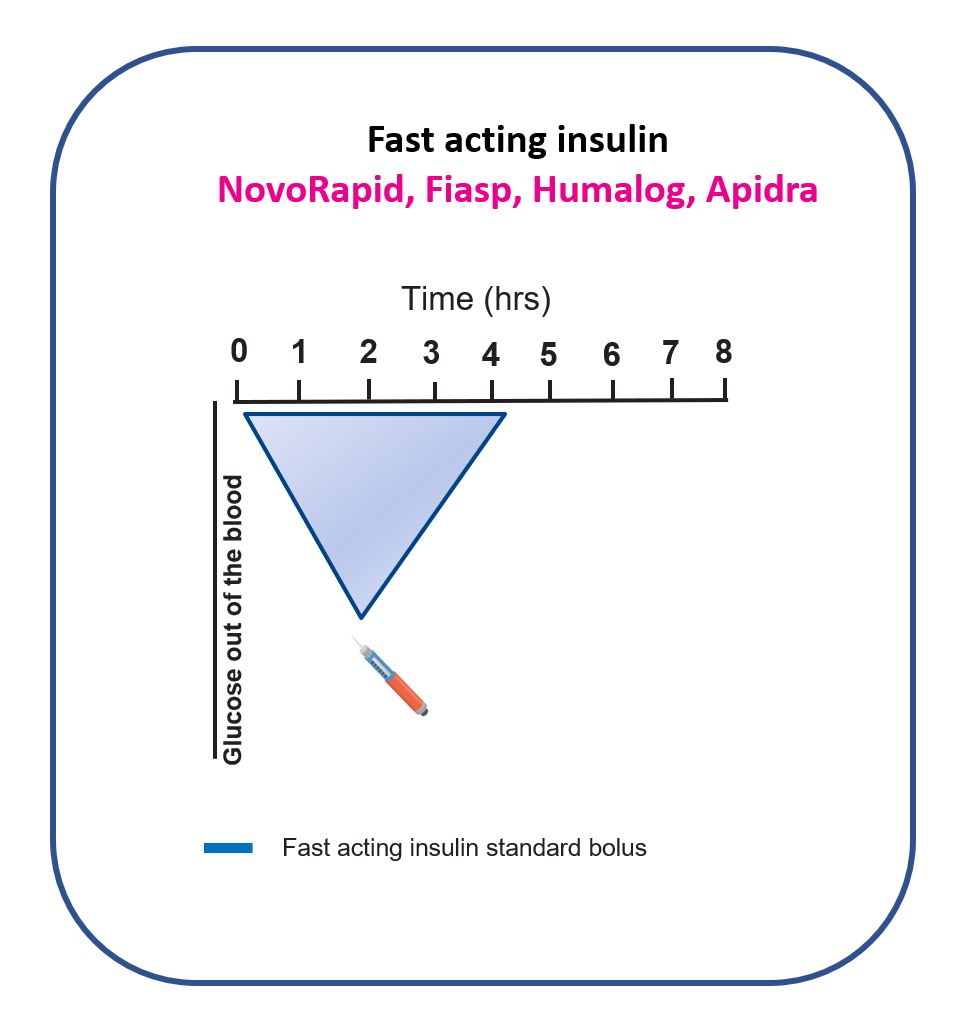
The diagram below shows why bolus insulin is fundamentally a timing problem. Fast-acting insulin starts slowly, often peaks around 2 hours after delivery, and can keep lowering glucose for around 4 hours.
Matching bolus insulin to meal carbohydrate
The starting point for meal bolusing is counting carbohydrates accurately. Your diabetes team should be able to teach this skill, it is also covered in the GNL carbohydrate counting guide.
You will then be given insulin-to-carbohydrate ratios (carb ratios) for different times of day. These vary between people and between mealtimes.
Example carb ratios (where u = units of fast-acting insulin and g = grams of carbohydrate):
- Breakfast: 1u : 15g
- Lunch: 1u : 25g
- Evening meal: 1u : 20g
For someone eating 50g carbohydrate at each of these meals:
Grams carbohydrate in meal ÷ grams in carb ratio = meal bolus units
- Breakfast: 50 ÷ 15 = 3.3 units
- Lunch: 50 ÷ 25 = 2.0 units
- Evening meal: 50 ÷ 20 = 2.5 units
Carb ratios vary considerably between people. One major driver is physical fitness and daily activity: the fitter and more active a person is, the less insulin they typically need for the same carbohydrate intake, so ratios often look “weaker”. Ratios also vary by time of day because insulin sensitivity changes through the day. Many people tend to be least sensitive in the morning and most sensitive at lunch. The point isn’t the pattern, it’s that different ratios by time of day are entirely normal.
How to test whether your carb ratios are well-matched
This test works best when life is reasonably stable, and is worth repeating more than once.
- No food or bolus insulin in the four hours before the test.
- Eat a balanced meal (carbs, protein, vegetables) with your usual carbohydrate amount for that mealtime; avoid a very high-fat meal (high-fat meals often need extra insulin later, covered in the Mealtime Insulin Guide).
- Count the carbs accurately and give the insulin before the meal.
- Do only your usual activity, and no corrections, in the four hours after eating.
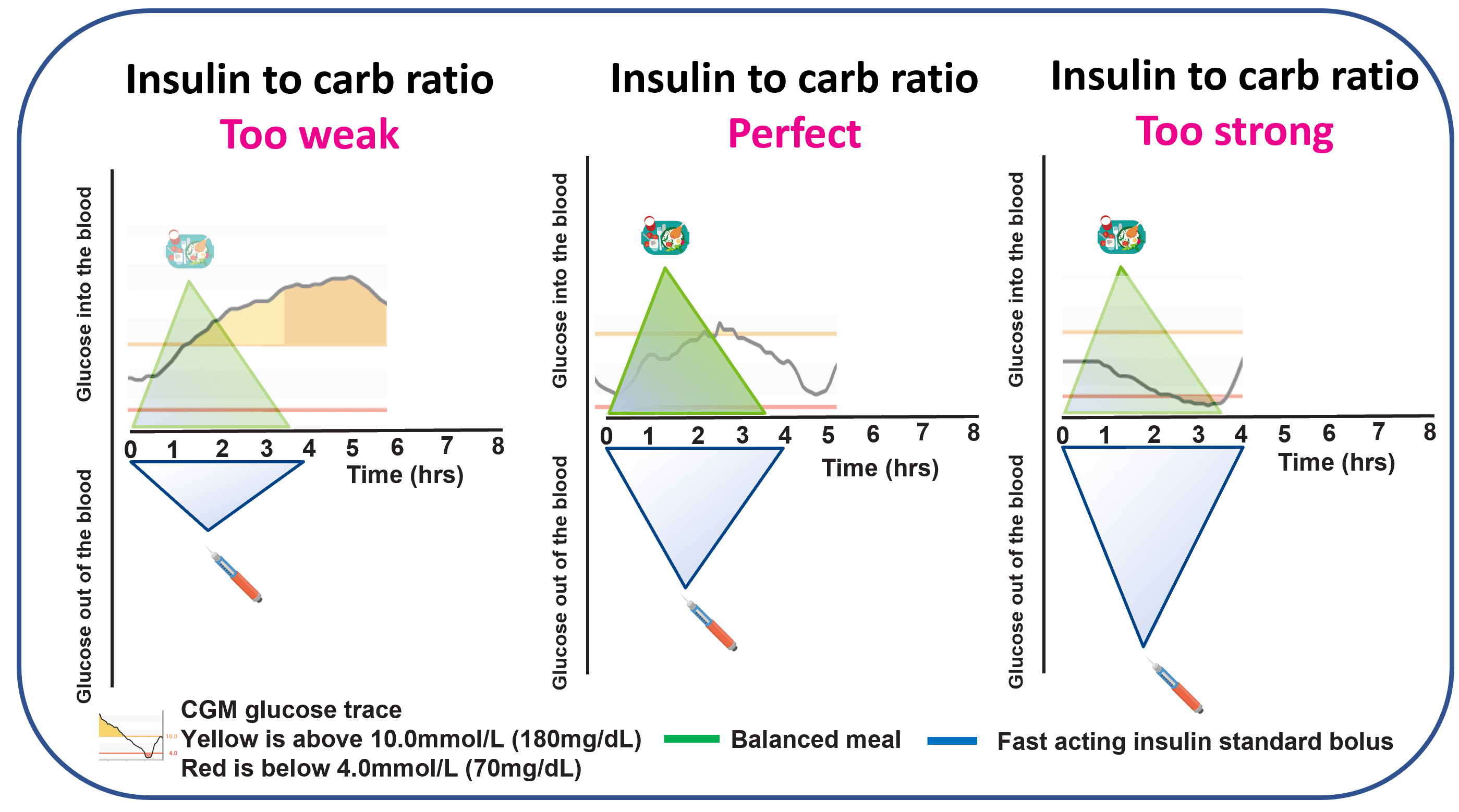
- Review the result: persistently high after the meal suggests the ratio is too weak (many people adjust by 10 to 20 per cent at a time); back to where it started suggests the ratio is close to right; dropping below where it started suggests the ratio is too strong.
Why glucose tends to rise after eating even with a perfect carb ratio
A perfect carb ratio does not prevent all post-meal rise, and that is not a failure. It is physiology.
Compared with glucose entering the bloodstream from a meal, injected or pumped insulin is slow. It is a tortoise-and-hare situation.

Giving insulin about 20 minutes before eating tends to keep the post-meal spike under better control for many meals. Studies support this as a practical approach for a wide range of meal types.
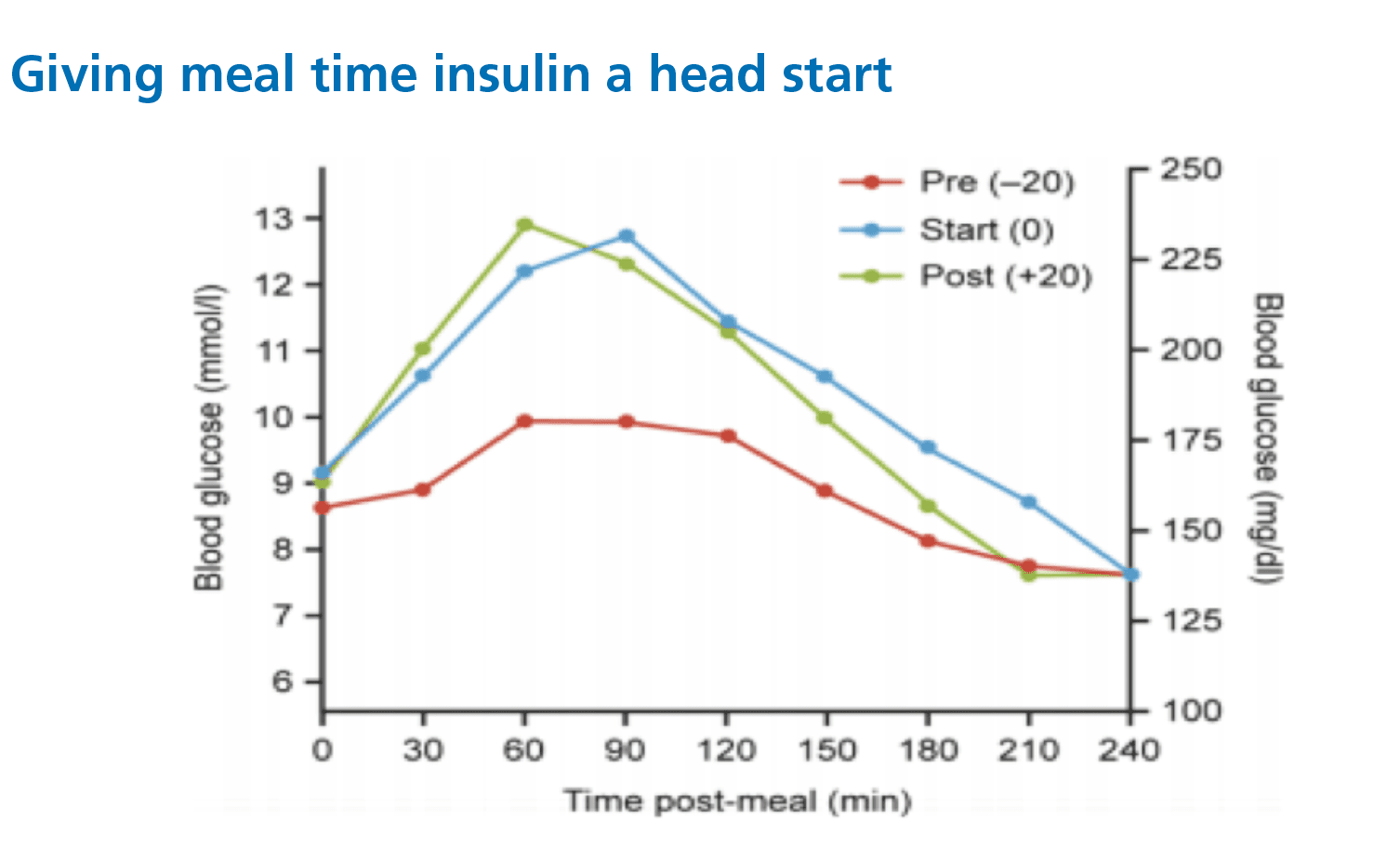
Even with this head start, a small spike often remains. Two mechanisms explain why.
1. The portal insulin problem
People without type 1 diabetes tend not to spike sharply after meals because insulin arrives in the portal vein at the same time as food, damping the liver’s glucose output. In type 1 diabetes, there is very little insulin in the portal vein and relatively more in the general bloodstream, so the liver’s mealtime glucose output is less effectively damped. The visual contrast (portal-rich vs portal-poor) is shown on the Hyperglycaemia page; the same diagram explains both why a meal spikes and why a high stays high.
2. The absorption speed problem
Insulin from injections or pumps absorbs from subcutaneous tissue much more slowly than insulin secreted directly into the portal system.
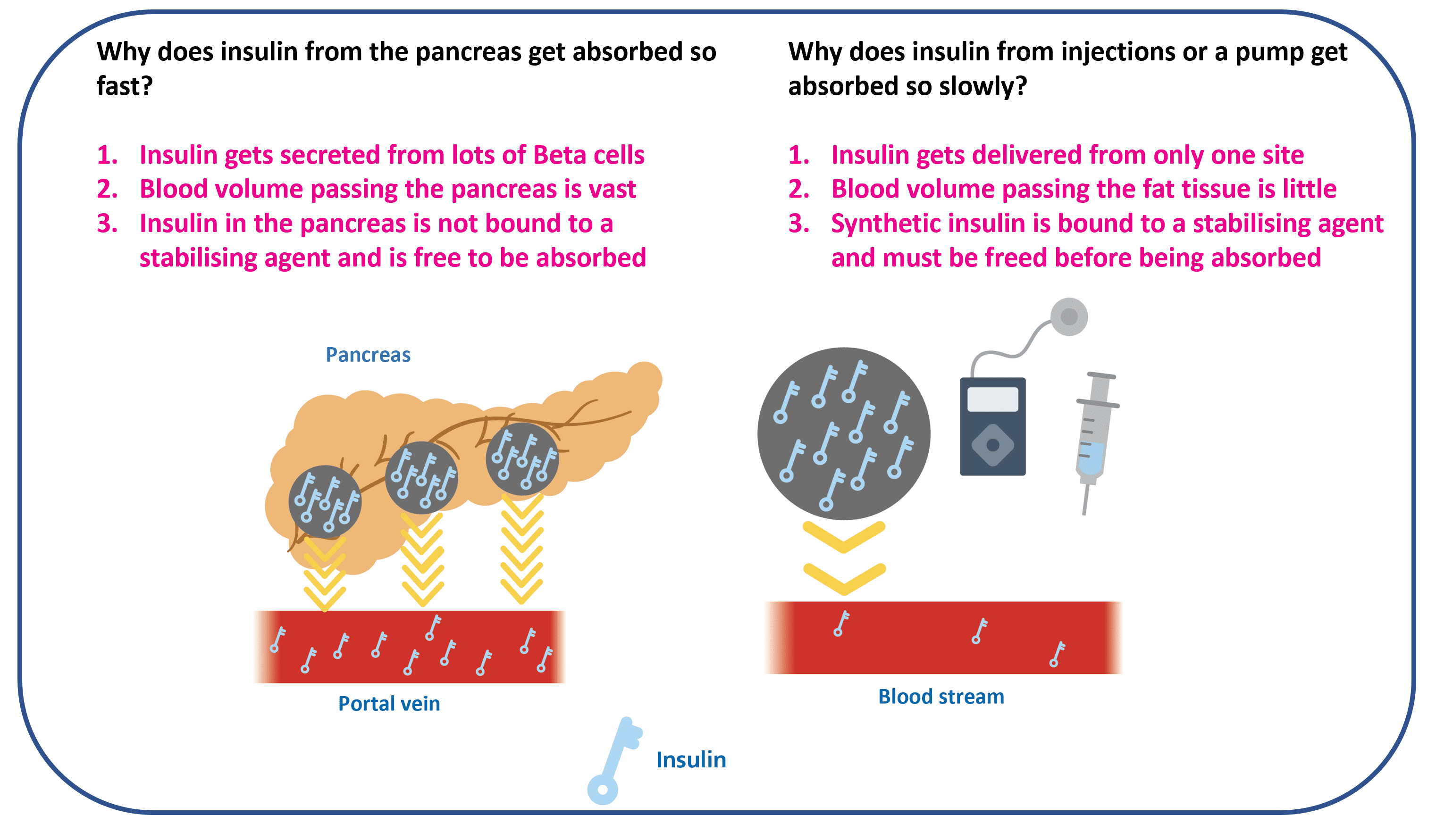
The combination, slow absorption plus low portal insulin, is the mechanism behind post-meal spikes. The good news is that it is addressable.
The SET framework from Dynamic Glucose Management covers how to vary pre-meal timing based on current glucose and trend arrows. The Mealtime Insulin Guide also covers practical spike-reduction approaches in detail, worth returning to after finishing Foundations.
Does injection site affect how quickly insulin works?
Yes. Fast-acting insulin tends to absorb fastest in the abdomen, second fastest in the upper arm, and slowest in the outer thigh.
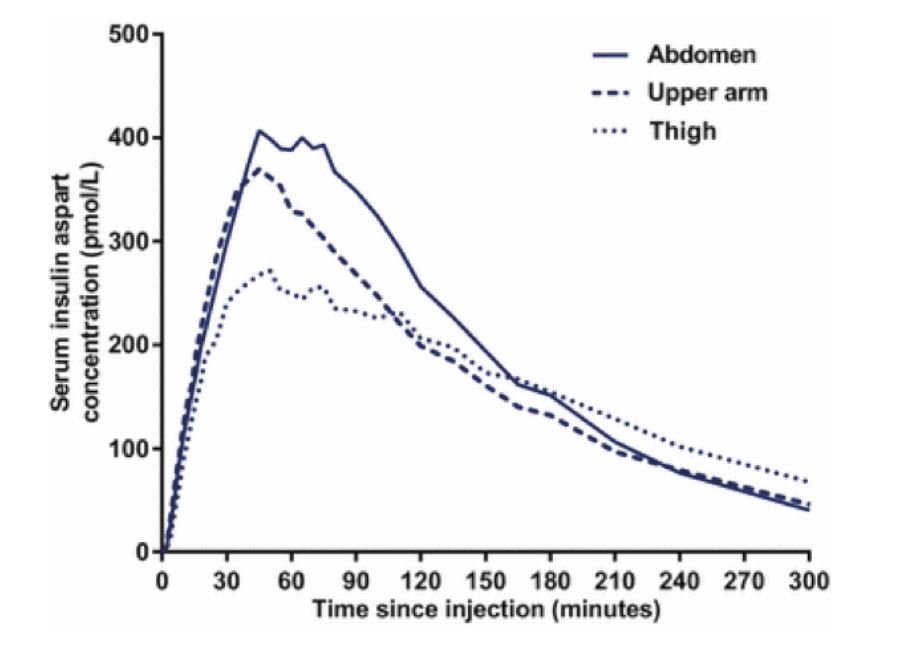
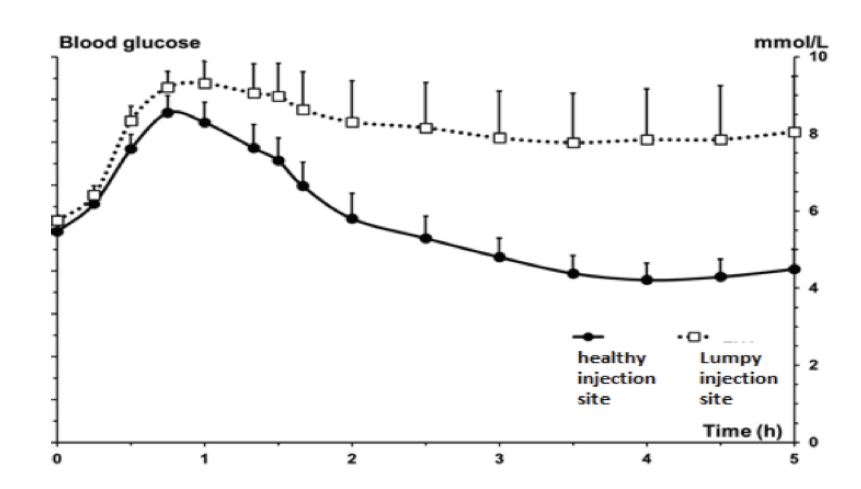
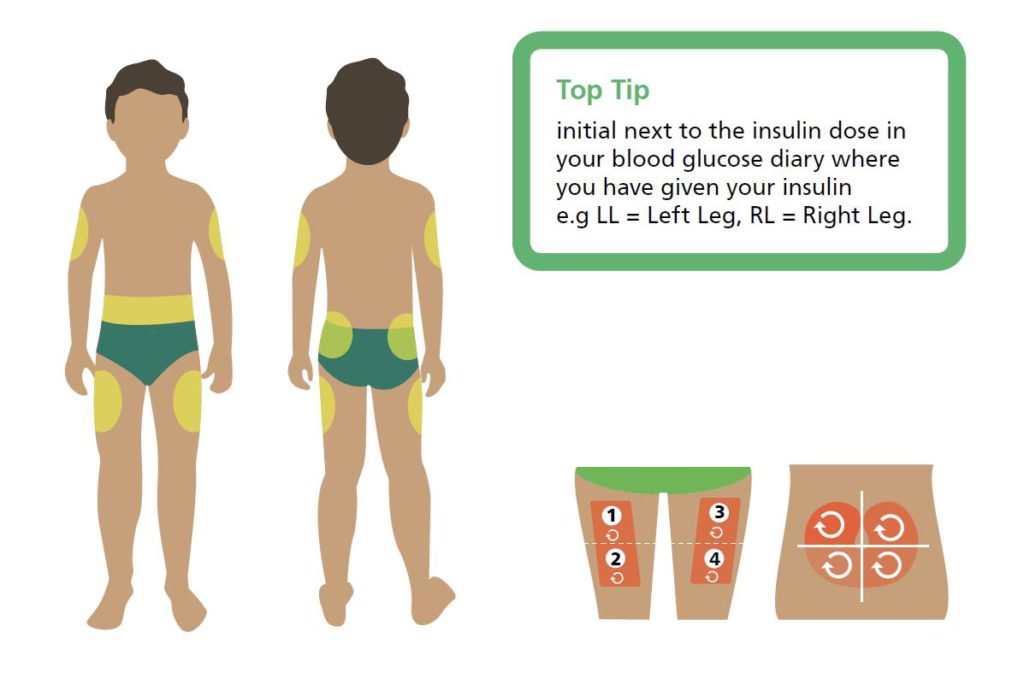
Worth exploring with your care team: pump users often do better keeping cannula sites to abdomen and upper arm, rotating regularly within those areas; switching between thigh and abdomen tends to create unpredictability because absorption speed changes. Pen users often find long-acting basal works well in the thigh or buttocks, with fast-acting in the abdomen or upper arm. Lumpy areas (lipohypertrophy) absorb insulin poorly and drive persistent highs; regular site rotation prevents the lumps developing.
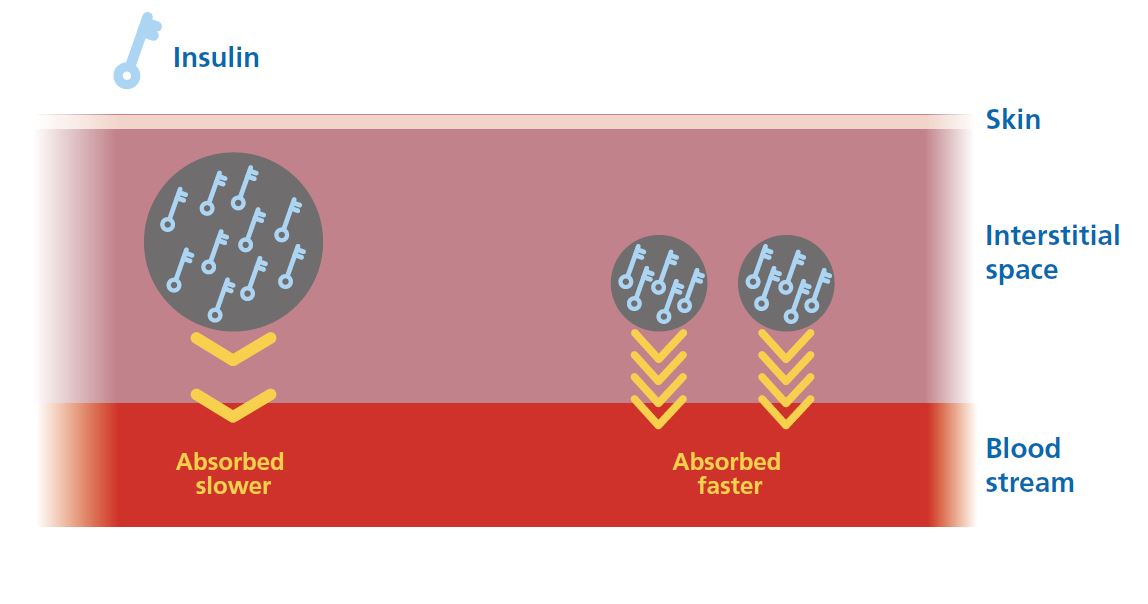
Do large bolus doses absorb more slowly?
Yes. A large insulin depot tends to absorb more slowly than the same dose split across smaller depots. The mechanism is surface area and diffusion: a smaller depot has more surface area relative to its volume and disperses faster.
Splitting every dose adds unnecessary complexity. A practical approach many people find useful: consider splitting any bolus above around 10 to 15 units.
- By injection: split into two equal amounts at least 2 cm apart (for example, 20 units → 10 + 10).
- By pump: use a split or extended bolus, around 50 per cent upfront and 50 per cent over the next 15 to 30 minutes.
The portal mismatch is the central trade-off of bolusing in T1D. Glucose arrives from a meal in minutes; insulin from a pen or pump arrives in hours, into the wrong vascular bed for liver-side damping. Pre-meal timing, site choice, and split-bolus technique all push at the same gap. Worth re-reading the timing and portal sections more than once; they sit underneath everything in Dynamic Glucose Management.
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Bolus Insulin Knowledge Check
That was bolus insulin, and why timing beats reaching for more units. A short assessment checks it has landed, and 9 out of 10 earns your certificate.
Part 4 of 12
Bolus Insulin
The ultimate guide to mealtime insulin dosing
A detailed downloadable guide to getting mealtime (bolus) insulin right with type 1 diabetes: dose timing, carbohydrate counting, and the adjustments that matter most.