
The Harsh Truth
For children diagnosed with type 1 diabetes under the age of five, the stakes are significantly higher. A diagnosis this early means exposure to decades of glycaemic instability, making early complications and reduced life expectancy a very real concern. Landmark studies, such as Rawshani et al. in The Lancet, have demonstrated that earlier onset is associated with increased cardiovascular mortality and overall risk.
There is also compelling evidence that persistent hyperglycaemia during early childhood negatively impacts the developing brain. Cameron and colleagues highlighted the cognitive implications of high glucose levels in this critical developmental window. In short, the earlier the diagnosis, the more bespoke advice is needed.
Glycaemic Targets and the Limits of Technology
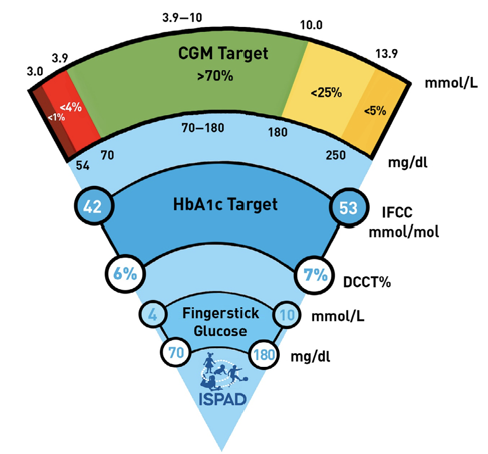
The goal in this age group is more than just “keeping up.” It’s achieving optimal control, defined by over 70% time in range (3.9–10 mmol/L), ideally over 50% in tight range (3.9–7.8 mmol/L) and a HbA1c of 6.5% or 48 mmol/mol. The guidelines recommend these levels as they reflect a glucose management that supports both physical health and cognitive development.
CGM technology offers a foundational level of insight, but real-world data confirms that it is not enough on its own, with children only achieving 54% TIR. Even with the use of Automated Insulin Delivery (AID) systems, many children under five still fall short of these targets. Median TIRs are often in the 60-65% range, and in this age group, hypoglycaemia becomes more common, not less.
This paradox arises because automated systems struggle with the unpredictable eating patterns and extremely low insulin doses typical of toddlers. Without thoughtful lifestyle structures in place, the systems alone are not enough.
Dusk-Then-Drop phenomenon
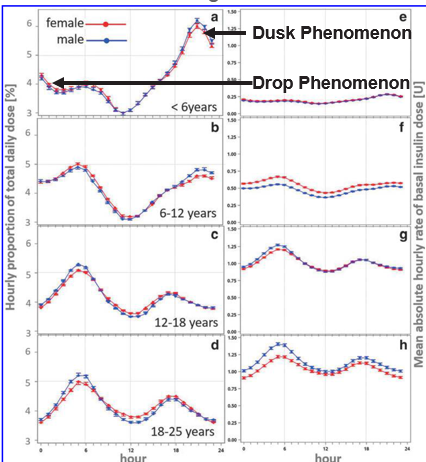
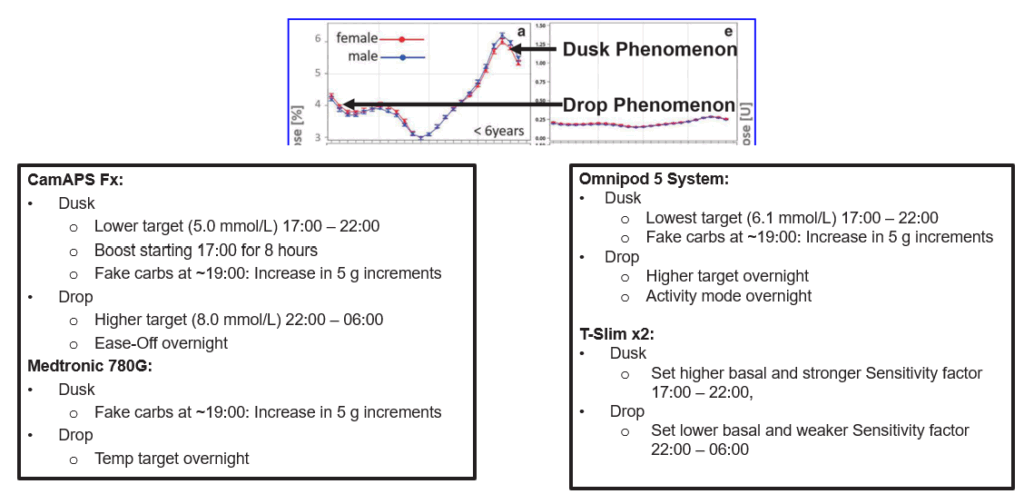
One of the most common and challenging glycaemic patterns in children under five is known as the “Dusk-Then-Drop” phenomenon. Between approximately 17:00 and 22:00, levels of cortisol and growth hormone rise, increasing insulin resistance and driving a need for significantly higher insulin delivery to prevent hyperglycaemia.
Although automated insulin delivery (AID) systems attempt to respond by increasing insulin delivery, they often cannot ramp up insulin fast enough to match the rapid rise in resistance. This mismatch frequently results in evening glucose spikes.
Following this, from around 22:00 to 02:00, levels of cortisol and growth hormone drop sharply. If insulin remains elevated from the earlier phase, this can lead to overnight hypoglycaemia.
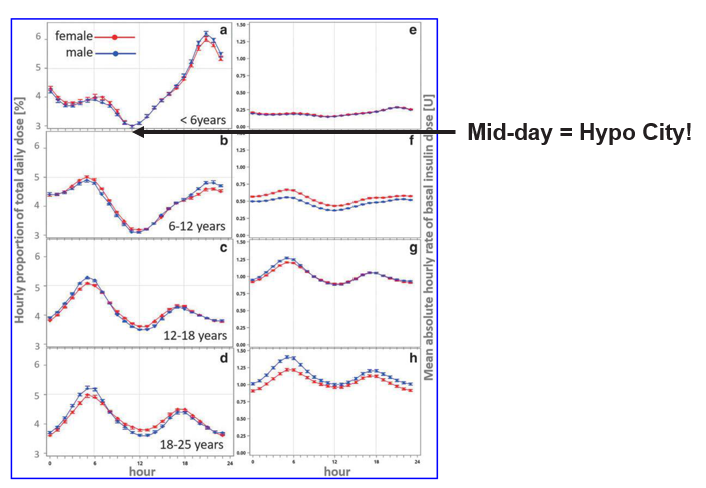
The German Diabetes Prospective Follow-up Registry (DPV) data illustrate this clearly, showing that children under six have the largest swings in insulin requirements of any paediatric age group, making this time of day particularly difficult to manage, even with AID Systems.
This hormonal pattern contributes to significant anxiety for families and frequent overnight alarms, as glucose levels often rise sharply in the evening and then fall dramatically through the night.
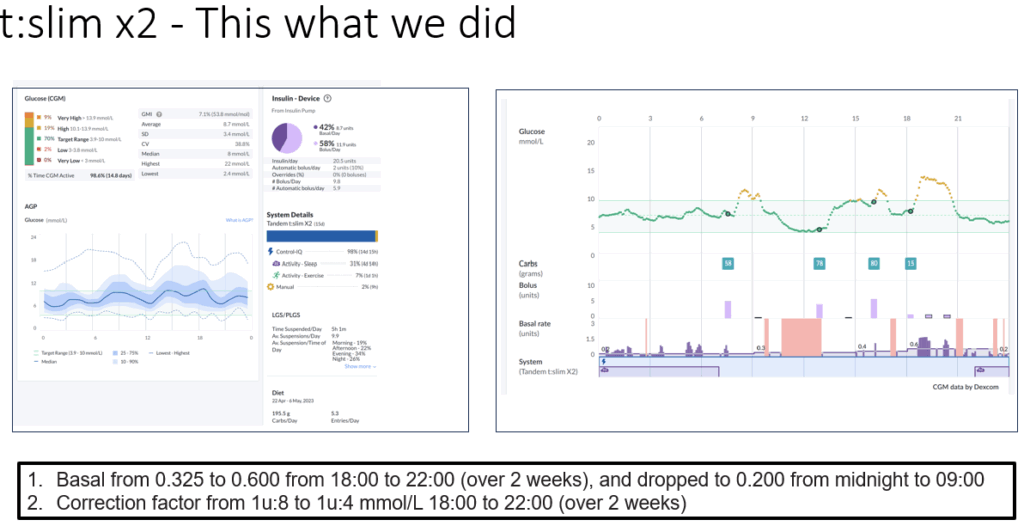
It is possible to proactively address this pattern. For example, using lower glucose targets in the early evening, from 17:00-22:00, can blunt the dusk rise. Adding “fake carbs” (a small bolus without real food) at 19:00 can help stop stubborn dusk glucose rises. This needs to be titrated gradually, in 5-gram increments, to find the right dose. This small bolus at 19:00 can be used with both standard pump therapy and injection therapy. However, with injections, the smallest dose available is 0.5 units, which may be too high for children in this age group.
Then, set a higher glucose target from 22:00 through to 02:00 to help prevent overnight lows caused by the drop element of the phenomenon
Here are some before-and-afters for the different systems;
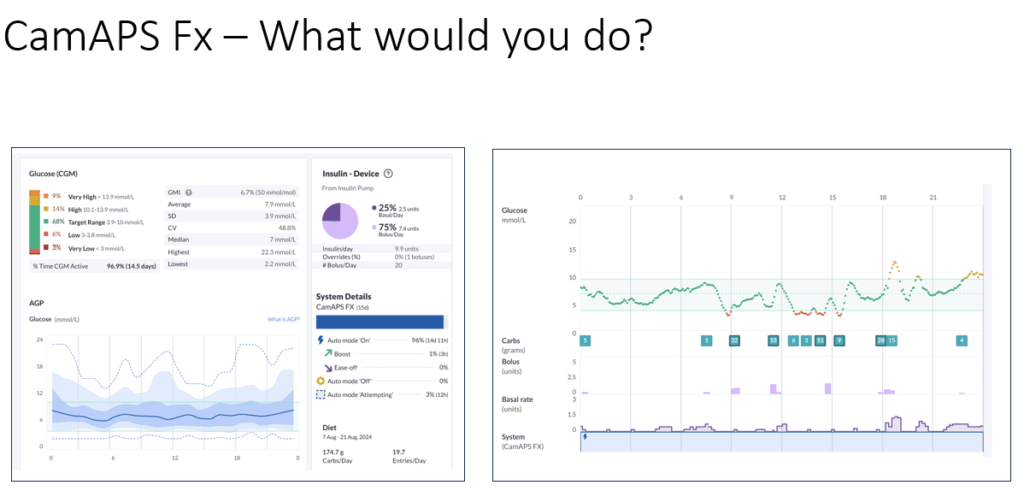
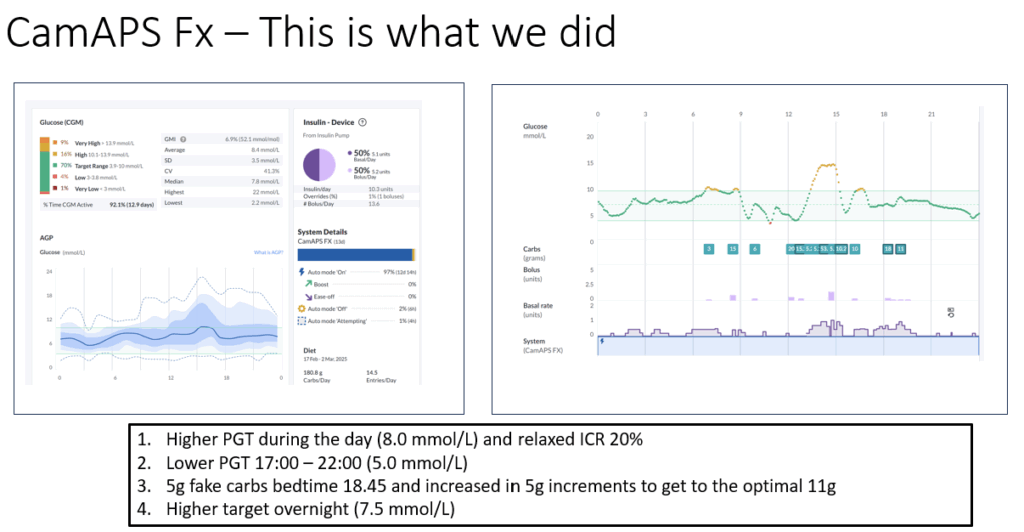
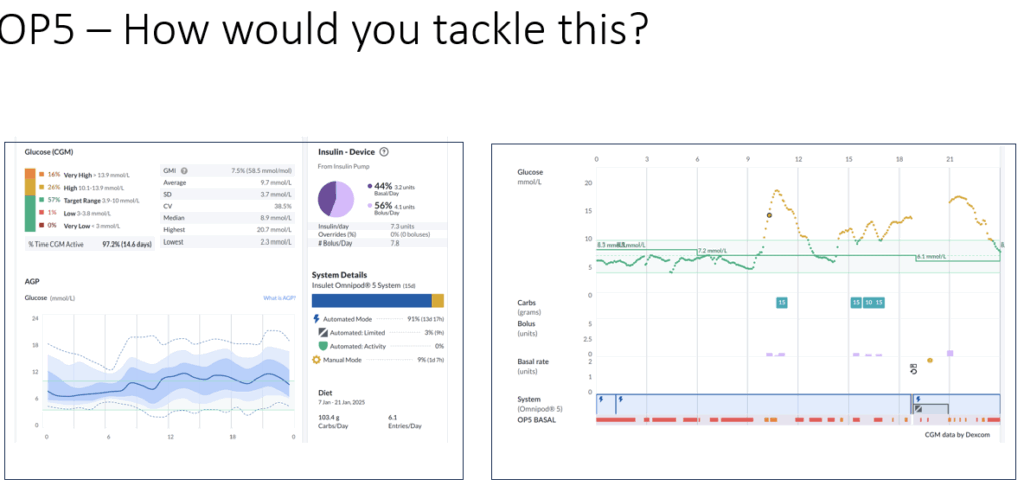
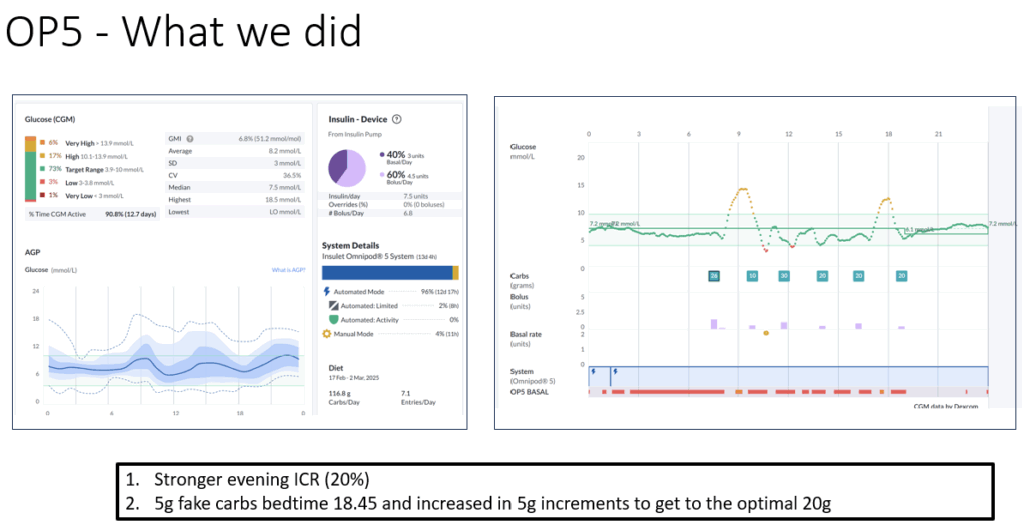
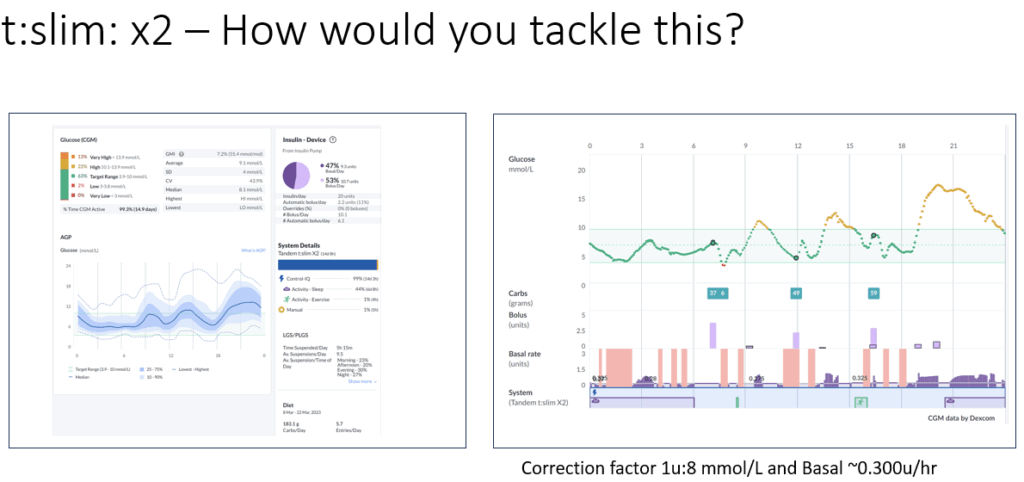
This graphic summarises the AID-specific options.
Tackling the Midday Hypo Trap
Another critical issue in under-5 management is the high incidence of hypoglycaemia between 11:00 and 14:00. For most children, this corresponds with heightened insulin sensitivity, particularly around and just after lunch.
To mitigate this, it’s important to optimise the insulin-to-carbohydrate ratio (ICR) for each meal. In practice, this often means stronger ratios for breakfast and the weakest at lunch. Common starting rules of thumb using total daily insulin doses are:
Breakfast ICR: 150 ÷ TDD
Lunch ICR: 250 ÷ TDD
Evening ICR: 200 ÷ TDD
These ratios align better with the child’s circadian rhythm and can be adapted based on the system’s performance.
Here AID system options
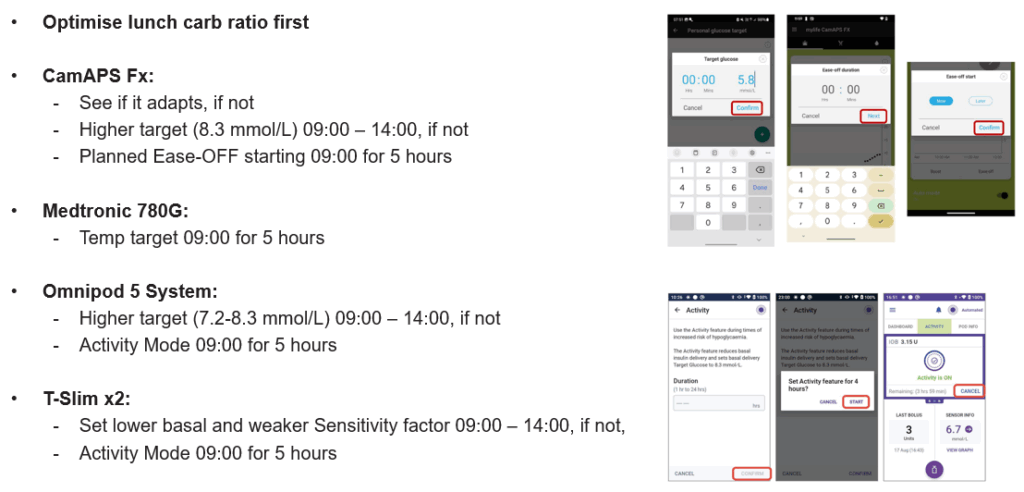
For children on total daily doses under 5 units, diluted insulin or use of activity mode around meals may be needed to prevent excessive insulin delivery.
Structured Meals and Confident Pre-Bolusing
One of the most important lifestyle interventions in under-5 diabetes management is structured eating. Regular family meals with consistent timing is the cornerstone for any young child. Even more importantly, it builds predictability in glucose levels.
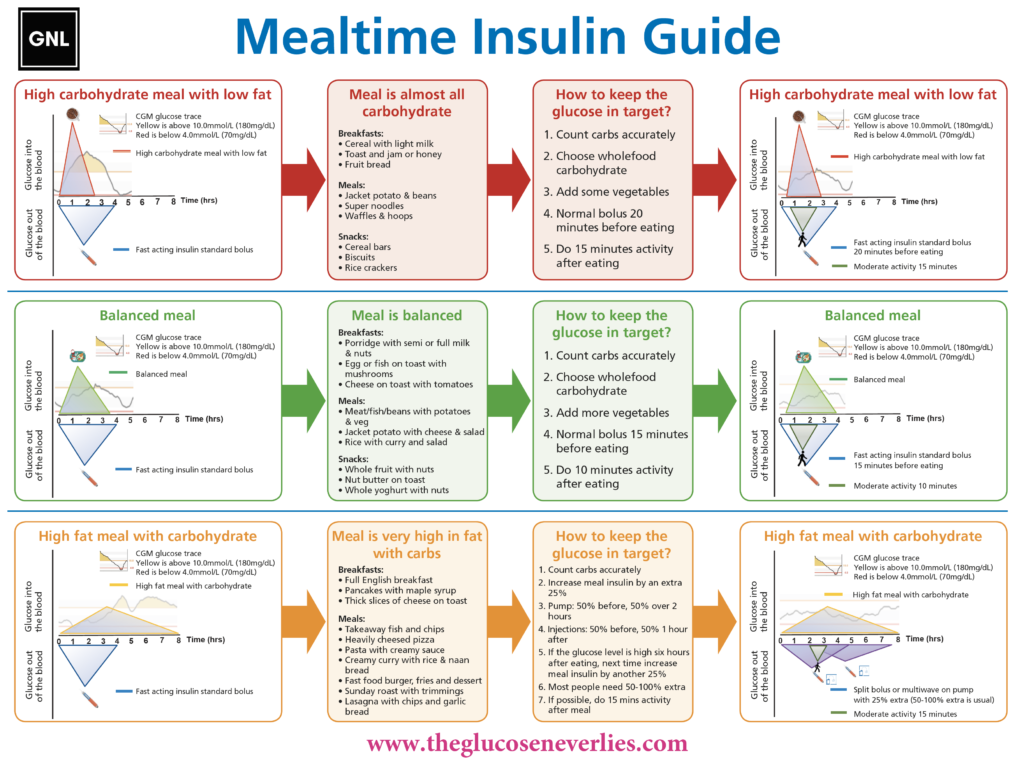
Pre-bolusing is central to success here. Aiming to give as much of the insulin dose as possible around 15 minutes before eating has a profound impact on post-meal glucose spikes. However, full pre-bolusing can be daunting for families, especially in fussy eaters or unpredictable mealtimes. A stepped approach, 50%, then 75%, and eventually 100% pre-bolus, helps build confidence gradually.
Carbohydrate counting should be as accurate as possible, ideally within 5 to 7 grams. Parents are also encouraged to avoid high glycaemic index cereals and to incorporate light physical activity after breakfast when feasible. The meal insulin guide is always worth revisiting.
Parenting with Precision: Behavioural Strategies that Work
Supporting children under five with type 1 diabetes goes beyond insulin adjustments. The parenting framework needs to provide both routine and flexibility. The Triple P framework supports meal routines and insulin timing.
Some of the most effective principles include:
- Keep exposing children to new foods and routines, even if they resist at first.
- Use games and challenges to make meals enjoyable.
- Implement small changes gradually.
- Create routines, same time, same place, for meals and insulin.
- Model behaviour by eating as a family, no phones or iPads at the table.
- Avoid force; instead, offer choices.
- Use positive reinforcement like stickers or charts.
- Maintain a calm family environment around meals.
- Plan the day to reduce decision fatigue.
- Focus on long-term consistency rather than daily perfection.
- These strategies reduce family conflict, increase adherence, and allow AID systems to perform more predictably.
Nutrition and Insulin: Getting the Basics Right
It’s also essential not to overlook basic nutritional needs. Using Schofield equations or equivalent calculators to estimate energy and protein requirements and having 40-50% as carbohydrate ensures the child is meeting growth targets. Balanced meals with appropriate macronutrient distribution are necessary for long-term health and for predictable glucose responses.
Final Thoughts: Progress, Not Perfection
Managing diabetes in children under five is one of the most difficult tasks, but it is also one of the most rewarding. With consistent routines, strong behavioural frameworks, tailored insulin strategies, and early adoption of CGM and AID systems, many children can achieve over 70% time in range and over 50% in tight range.
Success doesn’t come from perfection. It comes from iteration, structure, and trust in the long game. If the first five years of life set the foundation for all that follows, then investing deeply in those years, despite the challenge, is not just worth it. It’s essential.
Please share with those who may benefit.
Podcast to come soon!
Cheers
John (with help from ANP Louise Collins and Dr Ruth Krone)