
If you live with T1D and are choosing to consume drugs, please check in with your diabetes care team and have support in place. This is not medical advice.
Living with type 1 diabetes (T1D) means learning how to navigate life with a body that doesn’t always play by the rules, and partying is no exception. Whether it’s nights out, festivals, afterparties, hookups, or house raves, these are real experiences that many people with T1D encounter.
Yet there’s a surprising lack of honest, relatable guidance on how to manage them. Most official resources stop at “don’t do it”, but that doesn’t help when you’re already in it, planning it, or curious about what others with diabetes have done to stay safe.
This guide exists to explore that gap.

This guide is grounded in the lived experiences of people with T1D, including my own, those of friends, people I’ve worked with, and others I’ve met while partying through my 20s to 40s. It’s written for people with T1D, by people with T1D, and rooted in real-life situations, because, unsurprisingly, there are no clinical trials on this topic. The aim is simple: to reduce harm, spark honest conversation, and discuss practical strategies that have worked for navigating diabetes in high-energy, high-risk environments, without judgement or shame.
Let’s just get real for a second. The human brain doesn’t fully mature until somewhere between 18-25. That’s not a moral judgment, it’s neuroscience. The prefrontal cortex, which handles decision-making, impulse control, and long-term planning, is still wiring itself well into the mid-twenties. This matters. Especially when it comes to substances that profoundly alter how your brain’s circuits fire. When the brain is still developing, these substances carry a higher risk. That’s just the truth.
And this isn’t me standing on a soapbox. I drank alcohol well before I was 18 and took some drugs (not saying if legal or illegal). So I’m not judging, I’m reflecting. If anything, I wish I’d known how much more vulnerable my system was back then. Because when you combine a still-developing brain with substances that mess with serotonin, dopamine, and other core neurochemicals, the risks aren’t just short-term. They can shape the way those systems develop. That’s especially important for anyone under 16, and still relevant under 25.
This isn’t a “don’t do it” message. It’s a “know the terrain before you walk into it” message. If you’re living with T1D and thinking about partying, or already have, take this for what it is: a piece of the puzzle. Something to help you make smarter decisions, not perfect ones.
If you’re going to engage, do it with your eyes open. Be informed. Be surrounded by people you trust. And always, always check in with your diabetes care team.
Let’s be clear right from the start:
- This is not medical advice, it’s what others have done.
- This is not a guide to using drugs or alcohol.
- Always discuss any drug use with your healthcare team
We’re not discussing legality, and here’s why.
Laws around drug use vary wildly by country, region, and context. Some of the most harmful substances, like alcohol and cigarettes, are legal and socially accepted. Others, which may carry lower physiological risk when used with care, are criminalised.
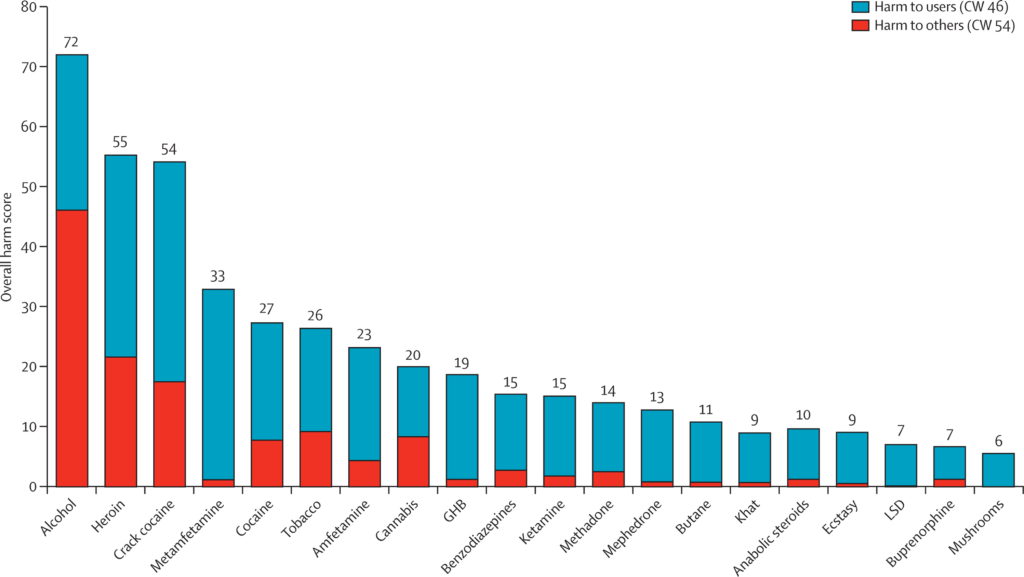
Take a look at the graphic from the landmark study that ranks drugs by objective harm. You’ll see that the most dangerous drug overall, by far, is alcohol. Not because it’s the most potent, but because it’s the most widely consumed, and carries real short and long-term health risks. That’s the reality.
This guide exists to inform, not to promote. It’s here so that people who do choose to party with T1D can do so with a greater awareness of the risks, and ideally, with better safety strategies. For some, reading this may lead to the decision not to take anything at all. For others, it may help reduce the risk of serious harm. Both outcomes are a win.
The Inverted U: Why Dose Matters
Every psychoactive substance, legal or illegal, works on an inverted U-curve.
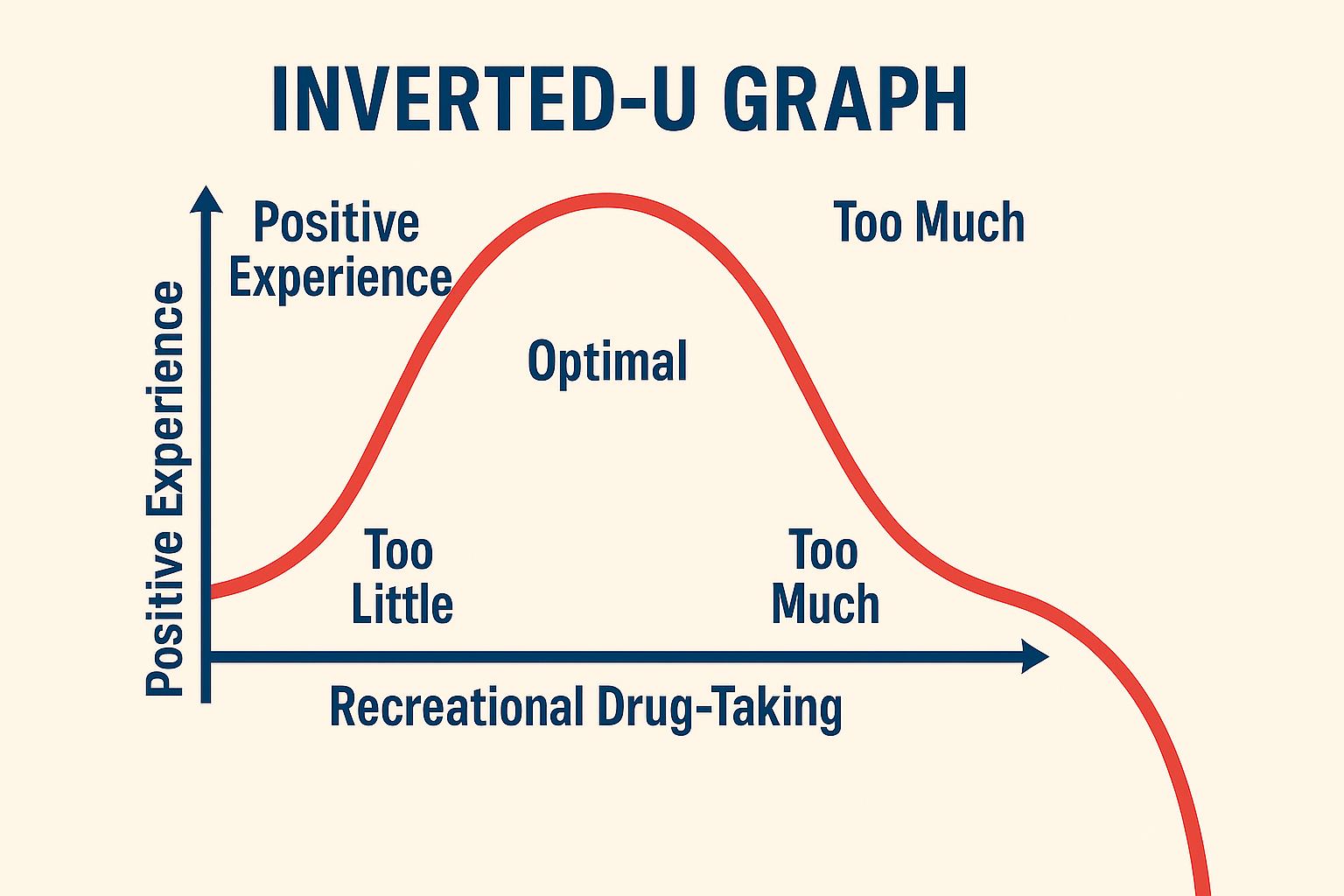
- At the low end, the dose has little or no effect.
- At the peak of the curve, you may feel exactly what you hoped for: connected, confident, energised, euphoric, calm, or introspective.
- But go beyond that peak and further, and the same substance can cause distress, confusion, anxiety, paranoia, dysphoria, blackouts, or worse.
This “Optimal”, the Goldilocks zone, is what many people aim for when they use a substance. But it’s highly variable and depends on four key factors:
- The substance itself — alcohol, nicotine, MDMA, cocaine, cannabis, ketamine, etc.
- The dose — how much is taken and how quickly.
- The person — their weight, tolerance, mood, neurobiology, and diabetes status.
- The set and setting — who they’re with, where they are, and how safe they feel.
The problem is, with unregulated substances, you rarely know the exact dose or purity. That makes overshooting the peak of the U, and falling into the zone of harm, a much higher risk, especially for those who are new or curious.
Take alcohol, for example:
- 2–10 units might help someone feel more relaxed, sociable, or connected.
- But 25–30 units will likely lead to vomiting, memory loss, or worse.
- And 300 units? Likely fatal!
With alcohol, the inverted U-curve is easier to grasp because it’s a regulated substance with clear labelling. We generally know how much alcohol is in each drink. Plus, the amount needed to go too far is relatively high, and the taste and volume itself often limits how much people consume. In contrast, with substances like cocaine, ketamine, or MDMA, there’s usually no way to know the purity, potency, or even the exact contents. Taking a large line or swallowing a wrap from an unfamiliar batch could be the equivalent of unknowingly downing 50+ units of alcohol at once, and that’s assuming the substance is even what you think it is.
That’s why throughout this guide, two principles come up over and over again:
- Test it, don’t guess it.
- Start low and go slow.
When it comes to non-regulated substances, the people contributing to this guide emphasise, test it, don’t guess it:
- Obtaining the substance ahead of time, not buying on the night.
- Using a reagent home test kit to verify content (e.g., MDMA, LSD, ketamine).
- Scales to weigh out the amount.
If someone chooses to experiment, start low and go slow. It’s the best way to reduce the chance of overshooting the inverted U. This mindset helps reduce the risk of panic, harm, or life-threatening situations, for themselves and for others around them.
- Start with a tiny dose, even smaller than “normal.”
- Trial in a comfortable set and setting when you are in a good mood.
- Never do it alone, especially with T1D.
- Let the people know you are with you have T1D and what you are taking.
- Wearing a medical ID, keeping glucose visible, and sharing CGM data when possible.
- Carrying hypo treatments (glucose tabs, gels, Lucozade, sweets).
- Avoid combining substances that push the U-curve even further out of reach.
Remember: There is no universal safe dose.
No “just take this much.”
Because the U-curve is unique to everybody, every moment, and every mix of context.
This guide uses neutral language, not slang, and always frames substance use through:
- Neurochemical effects (e.g., serotonin, dopamine, GABA)
- Behavioural changes (e.g., energy, inhibition, hunger)
- Perceptual shifts (e.g., visuals, altered time, ego loss)
One more time, this guide is:
- Not promoting substance use.
- Not a how-to.
- Not a legal guide.
- And absolutely not a substitute for clinical or medical advice.
It is a resource built from the reflections and experiences of people with T1D who’ve lived these realities, and want to offer others the chance to learn from what they’ve seen, felt, and learned.
Every person is wired differently, both psychologically and physiologically. What might feel like a magical, expansive experience for one person could be destabilising, overwhelming, or even dangerous for another. One person’s elixir can be another’s poison.
Some people have a natural “off switch”, an intuitive sense of when enough is enough. Others find it harder to stop, especially if the substance is tapping into deeper patterns of seeking, escape, or dysregulation. There are real, biological differences in how people respond to dopamine, serotonin, GABA, and other neurochemicals. Some brains are simply more prone to habit loops and compulsion. Some bodies carry trauma that alters how safe a high can feel. And some people, through genetics, history, or circumstance, carry a higher baseline risk for harm.
As an example, I lived with undiagnosed ADHD until July 2025, which likely explains my tendency to use stimulants. I also grew up in a team sport environment where drinking alcohol and using recreational drugs was commonplace. Had I been diagnosed earlier, or perhaps chosen swimming over cricket, this guide might never have existed!
As you move through each section, keep in mind:
- Test it, don’t guess
- Start low and go slow
- The inverted U-curve
- Set and setting create the conditions for experience
Stimulants (Caffeine, Nicotine, MDMA, Amphetamine)
Cannabis, Ketamine and hallucinogens (LSD and Psilocybin)
Leave a Reply