

Ready to learn how to tackle insulin resistacne with type 1 diabetes.
Prefer a Podcast? If so, check out Episode 14

We begin with the foundation, lifestyle, and build up from there, step by step, like a pyramid.
1. Activity: Aerobic Exercise, Strength Training, Movement, Post-Meal Walking
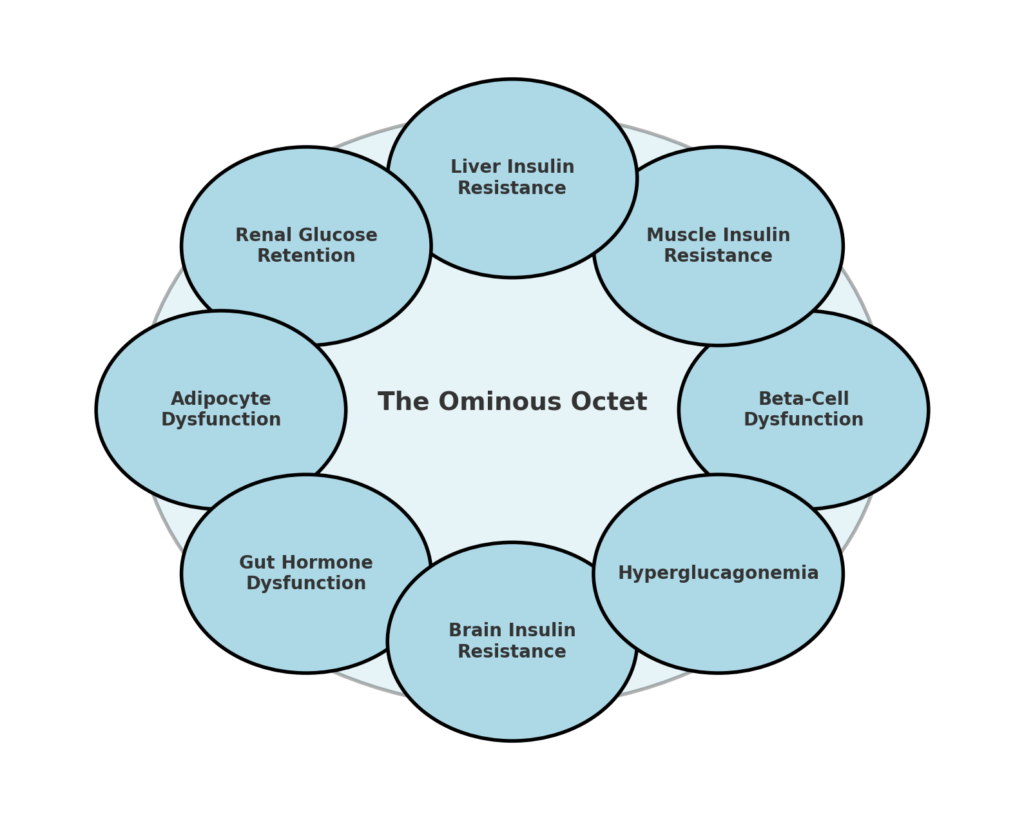
Physical activity plays a crucial role in improving insulin sensitivity, enhancing glucose disposal, and reducing metabolic dysfunction, all of which are key to addressing the Ominous Octet in type 1 diabetes. I know this better than most.
In two years (2022-2024), I suffered three broken collarbones and a broken ankle, which led to a drastic drop in activity and a major episode of severe depression. During that time, my daily insulin needs skyrocketed from 35 units to 60 units per day.
Since fully recovering in January 2025, I’ve worked hard to regain my fitness, and after three months of sustained, high levels of activity, I’ve managed to bring my insulin dose back down to 35 units per day. It’s been a long road, but the impact of movement on insulin sensitivity couldn’t be clearer.
Strength training is one of the most effective ways to enhance muscle insulin sensitivity by increasing glucose uptake without needing insulin. Strength training also helps prevent muscle loss, which is particularly important for staying insulin-sensitive, especially if you lose weight.
Aerobic exercise also plays a crucial role in clearing metabolic “clutter”, particularly by burning intramuscular fat deposits known as DAGs (diacylglycerols). Regular aerobic activity, such as brisk walking, cycling, or swimming, helps remove excess fat from muscle and liver cells, improving how the body processes glucose. It also enhances liver insulin sensitivity, helping regulate glucose production and preventing unnecessary spikes in blood sugar.
Beyond structured exercise, simply being active throughout the day is essential for glucose control. Movement improves insulin action in three key ways: it helps insulin reach muscles faster, enhances non-insulin-mediated glucose uptake, and burns stored fats that interfere with insulin function.


Staying physically active also improves brain insulin sensitivity, which helps regulate hunger, metabolism, and overall energy balance.
To effectively counteract insulin resistance and optimise glucose metabolism, consider integrating some or all of the following strategies into your routine (choose the ones that sing to you):
- Take a 10–15-minute walk after meals: This enhances glucose disposal through non-insulin-mediated uptake in muscles and supercharges the circulating meal insulin, so you need less or don’t get after-meal spikes.
- Engage in strength training 3–4 times per week: Use compound movements (e.g., squats, deadlifts, presses) to increase muscle size and improve insulin sensitivity.
- Incorporate aerobic exercise (3–5 times per week): Cycling, swimming, or brisk walking to burn excess fats in muscle and liver cells, reducing insulin resistance.
- Stay active throughout the day: Stand up regularly, walk instead of driving short distances, and engage in active hobbies like gardening or dancing.
- Mix resistance and aerobic training: This provides synergistic improvements in glucose control and fat metabolism.
- Use activity “snacking“: Short bursts of movement like bodyweight exercises, stretching, or stair climbing to keep the metabolism active throughout the day.
For more insights, check out The GNL Activity Snacking Podcast, where we dive deeper into how movement supports metabolic health! Also, managing T1D is challenging, that’s why I wrote the Exercise Guide.
2. Weight Management (Weight Loss)
If you are overweight, losing body fat can significantly improve insulin sensitivity and overall metabolic health. However, even if you are not classified as overweight, you may still carry excess fat around the liver and central organs. This is often referred to as visceral fat. This type of fat is particularly harmful as it contributes to insulin resistance, inflammation, and metabolic dysfunction.
Losing 5–10% of body weight has been shown to provide meaningful improvements in insulin sensitivity. However, losing 15–20% can be extremely effective, particularly in reversing insulin resistance in the liver and muscle. The key to effective fat loss is ensuring that the weight loss comes from fat rather than muscle. To achieve this, it’s essential to follow specific strategies that prioritise muscle preservation and metabolic health while reducing body fat.
Key strategies:
- Prioritise protein intake: Aim for 1.5–2g of protein per kg of body weight to maintain muscle mass while in a calorie deficit. Protein helps prevent muscle loss, supports satiety, and aids in metabolic function.
- Incorporate strength training: Engaging in resistance training at least 3–4 times per week helps preserve lean muscle mass and ensures that the weight lost comes from fat rather than muscle.
- Create a calorie deficit: Aim for a 500–1,000 kcal deficit per day, which supports a steady weight loss of 0.5–1.0 kg per week. This gradual approach prevents muscle loss and promotes sustainable fat reduction.
- Reduce processed carbohydrates and refined sugars: While total calories matter most, reducing processed foods can help stabilise blood sugar levels and prevent excessive insulin spikes.
- Support fat metabolism with activity: Regular aerobic exercise and strength training improve the body’s ability to burn stored fat, particularly in the liver and muscles, where excess fat storage contributes to insulin resistance.
- Prioritise sleep and stress management: Poor sleep and chronic stress can increase cortisol levels, making it harder to lose fat and increasing insulin resistance. Aim for 7–9 hours of quality sleep per night.

3. Nutrition (Low Sugar Intake, High Vegetables, High Fibre)
Nutrition plays a crucial role in optimising glucose control, reducing insulin resistance, and supporting weight management. Making strategic food choices can enhance insulin action, prevent glucose spikes, and improve beta-cell function over time. While individual needs vary, certain dietary principles are universally beneficial for people with type 1 diabetes.
Key strategies:
- Avoid excessive fat intake: High-fat diets can worsen beta-cell dysfunction by increasing free fatty acids (FFAs), which impair insulin secretion and action. Moderating fat intake, particularly saturated fats, helps support healthy insulin signaling.
- Consider a moderate carbohydrate approach: Reducing excessive carbohydrate intake can minimise post-meal insulin spikes, improve glucose stability, and reduce overall insulin requirements. However, balance is key, carbohydrate intake should be tailored to activity levels, insulin dosing, and metabolic needs.
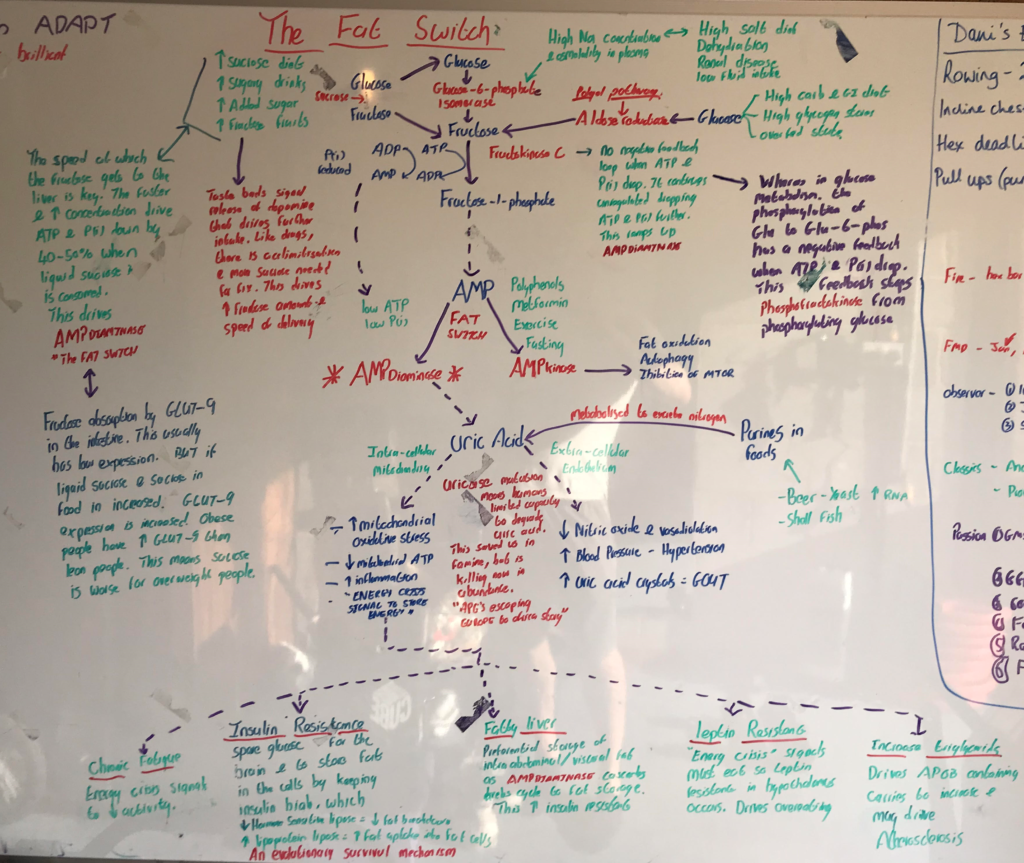
- Limit sugar intake: The podcast by Dr. Rick Johnson highlights how excessive sugar, particularly fructose, contributes to insulin resistance by flicking the “Fat Switch” on in the liver. Prioritising natural, whole-food sources of carbohydrates can help reduce metabolic stress. See the diagram for my nerdy notes on the “Fat Switch”. Simply, avoid sugar (glucose/fructose) based hypo treatments (coke, lemonade, sweets, etc) and keep to glucose-only (dextrose tablets and glucose-only sports drinks) hypo treatments.
- Focus on fibre-rich, whole-food meals: High-fibre foods slow down glucose absorption, improve gut hormone responses, and enhance satiety, leading to better post-meal glucose control. Aim for a diet rich in vegetables, legumes, whole grains, and nuts.
- Monitor glucose trends using a CGM: A CGM provides real-time feedback on how different foods affect blood sugar, helping refine meal timing, portion sizes, and insulin dosing. This is especially useful during caloric restriction and exercise to prevent hypoglycaemia or excessive glucose swings.
- Pre-bolus insulin 15–20 minutes before most meals: Taking insulin ahead of meals allows it to start working before glucose enters the bloodstream, leading to smoother postprandial glucose levels and less variability. You can get fancy by using SET from GAME-SET-MATCH.



4. GLP1-RA’s (Semaglutide or Tirzepatide)
Older GLP-1 receptor agonists, such as liraglutide and Dulaglutide, have been shown in large-scale evidence reviews to improve HbA1c, reduce total insulin dose by approximately 10-15%, and lead to around 5-10% weight loss. However, the newer GLP-1 receptor agonists such as semaglutide (Ozempic) and tirzepatide (Mounjaro) are much more powerful and offer much larger several metabolic benefits beyond glucose control. These medications enhance the body’s natural hormone responses, addressing multiple aspects of glucose regulation, appetite control, and insulin efficiency.
What’s the difference between Semaglutide (Ozempic) and tirzepatide (Mounjaro)?
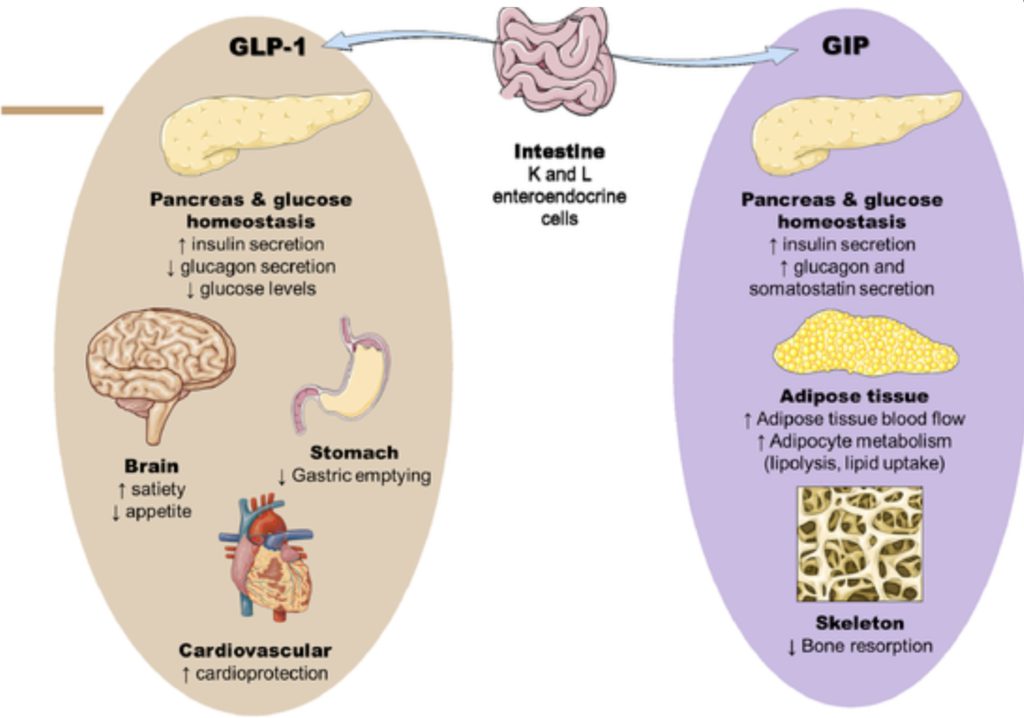
Semaglutide is a GLP-1 receptor agonist that mimics one hormone (GLP-1), while tirzepatide is a dual agonist that mimics both GLP-1 and GIP. Quick recap on why they are so potent.

Which is best?
In trials of people with type 2 diabetes, semaglutide typically reduces HbA1c by 1.5–2.0% and supports 10–15% weight loss at higher doses, while tirzepatide can lower HbA1c by up to 2.5% and lead to 15–22% weight loss. Both are given as weekly injections and have similar side effects, mainly nausea and digestive upset, especially during dose increases. Tirzepatide’s GIP component may make it more effective for some, but individual response varies, what works best depends on the person.
What about people with type 1 diabetes?
Why would GLP-1/GIP be extra beneficial?

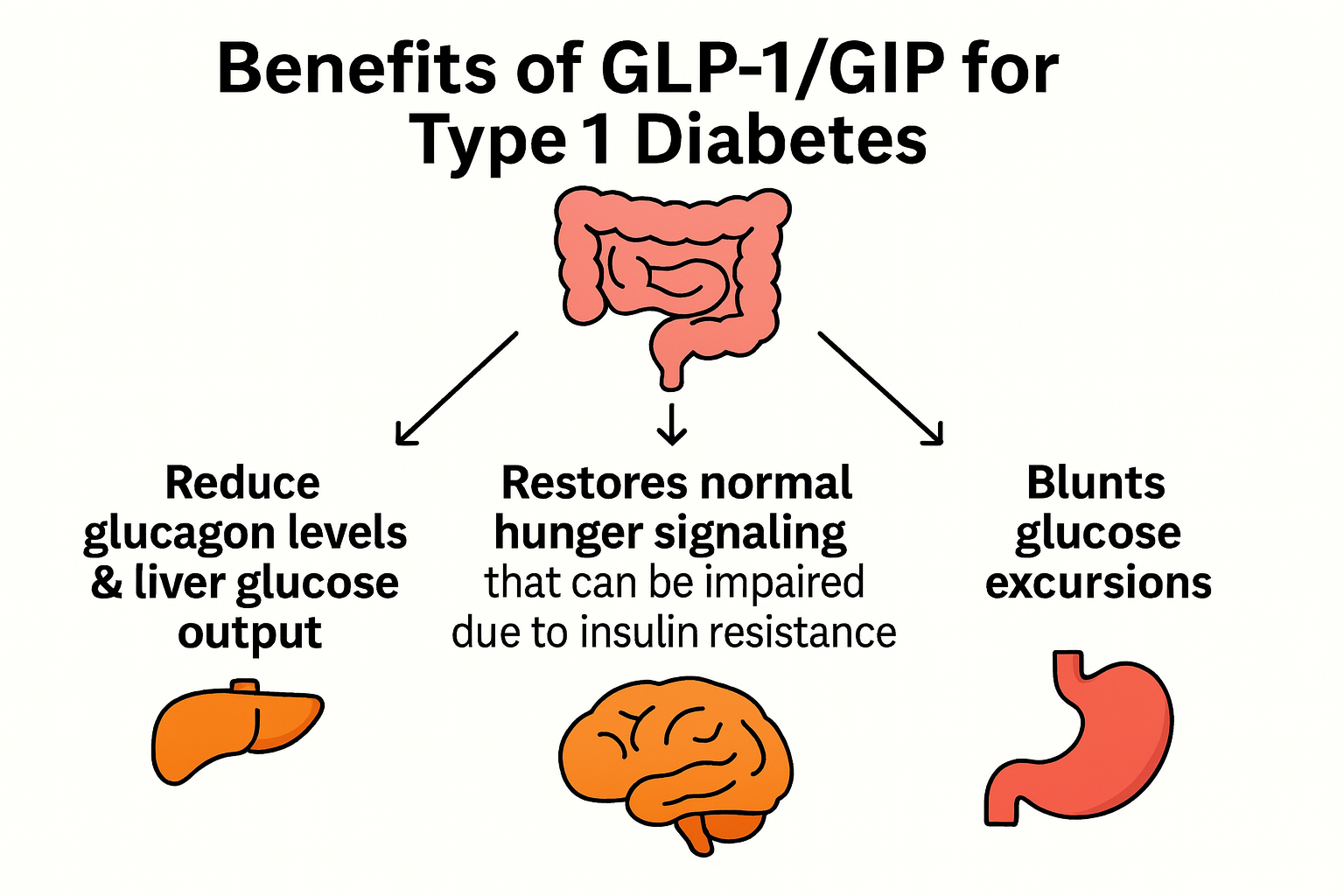
- Reduce glucagon levels & liver glucose output: People with type 1 diabetes produce very little or no insulin from the pancreas. Normally, insulin acts as a brake on glucagon production after meals. In its absence, glucagon can go into overdrive, leading to excessive glucose release from the liver. Increasing levels of GLP-1 and GIP can help restore this balance. These gut hormones suppress glucagon after meals, improving post-meal glucose control and essentially restoring the body’s natural “brake” on glucose production.
- Restore normal hunger signaling & appetite regulation: Many people with type 1 diabetes experience insulin resistance, in part due to chronically elevated circulating insulin levels, often up to four times higher than people without T1D. These high levels reach the brain’s hunger centers and can disrupt normal appetite regulation. As a result, appetite signals become dysregulated, making it harder to feel full and easier to overeat, which can contribute to weight gain. GLP-1 receptor agonists help restore proper hunger cues. They work by binding to receptors in the hypothalamus, the part of the brain that regulates appetite, and enhance the body’s natural satiety signals, reducing cravings and excessive food intake.
- Blunt large glucose excursions: By slowing stomach emptying, these medications slow glucose absorption to better match the insulin profile that peaks after 90 minutes and lasts 4-5 hours. However, if the delay is too long, especially after a higher-fat meal, insulin dosing becomes challenging if not on an AID system.
What does the evidence say for people with type 1 diabetes?
Emerging evidence from the ADJUST-T1D randomized controlled trial (36 adults in both arms) suggests that Semaglutide (Ozempic) may offer meaningful benefits for adults with type 1 diabetes and obesity. Over 6 months, participants using an automated insulin delivery (AID) system and receiving weekly semaglutide (up to 1 mg) achieved:
- ↑ Time in Range by ~9% (70–180 mg/dL)
- ↓ Weight by 8.8 kg (~10%)
- ↓ HbA1c by 0.3% (3 mmol/mol)
- No increase in hypoglycaemia or DKA risk
- 36% of those on semaglutide achieved >70% time in range, <4% time below range, and ≥5% weight loss, compared to 0% in the placebo group.
In a single-centre, 8-month observational study, adults with type 1 diabetes (26 adults) and obesity (average BMI ~36.7 kg/m²) were treated with tirzepatide (Mounjaro), a dual GLP-1/GIP receptor agonist.
Key outcomes at 8-months:
- ↓ HbA1c by 0.6% (6 mmol/mol) at 8 months
- ↓ Body weight by 10% at 8 months
- ↑ Time in Range (70–180 mg/dL) by 13%
- ↓ Total daily insulin dose by ~29%
- The drug was well tolerated, with only two patients discontinuing due to side effects (one for hypoglycaemia, one for constipation), and no diabetic ketoacidosis (DKA) reported.
So, it’s a slam dunk then, these medications must be available for all people with type 1 diabetes living with obesity, right?
Well, not quite. When you consider the approval pathway for these drugs in type 2 diabetes and weight management, it’s based on data from thousands of participants, followed for over two years, with robust evidence and a favourable safety profile. In contrast, for type 1 diabetes, we currently have data from fewer than 40 people in a randomized controlled trial and just 26 individuals in a single-centre observational study. While the early results are encouraging, this is nowhere near the evidence threshold needed for inclusion in national guidelines, NHS formularies, or insurance coverage. So it’s currently not covered on-label.
At present, any use in type 1 diabetes would either be off-label via a prescribing doctor (a lot are doing this) or through unregulated online sources, which carry significant risks. I’m not here to preach, but to highlight that going solo increases the risk, you won’t have liver enzymes monitored, and if you don’t reduce your insulin under medical supervision, you could face a higher risk of hypoglycaemia.
If going for it, read this excellent opinion of GLP1-RA for T1D. It highlights the need for;
- Lower daily insulin doses by approximately 30% upon initiation to prevent hypoglycaemia, as the medication lowers food intake and glucagon levels.
- Monitor for nausea or digestive side effects, as slowing gastric emptying can cause temporary gastrointestinal discomfort in some individuals.
- Easier to manage on an AID system due to delayed food absorption, making insulin dosing challenging.
- Pair with strength training and protein intake to preserve muscle mass while benefiting from reduced appetite and weight loss.
- Use a CGM to track glucose trends and adjust insulin dosing accordingly, particularly after eating.
- Get blood tests before and after initiation.
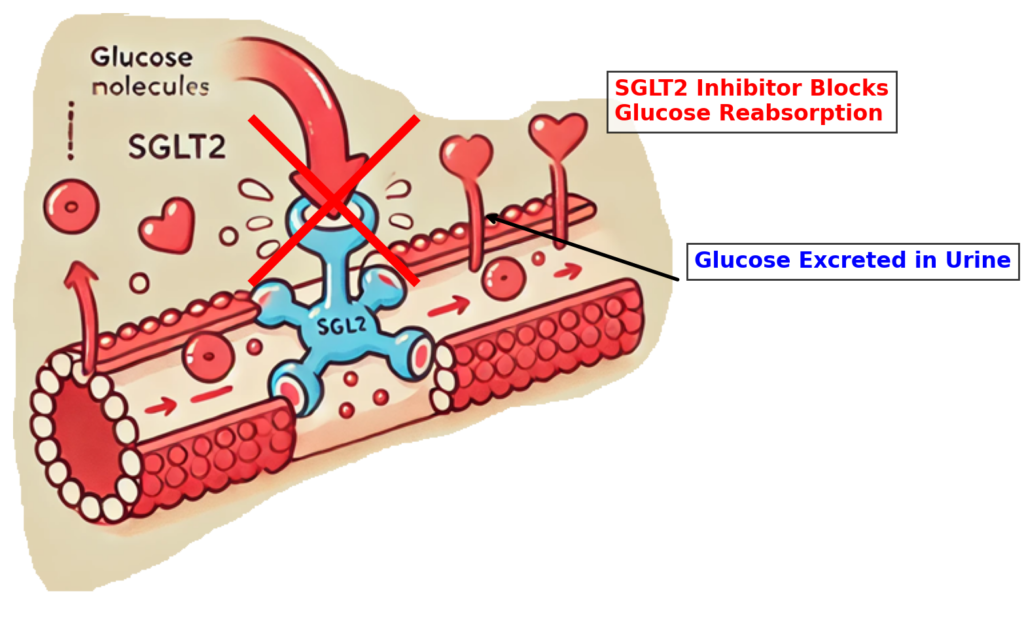
5. SGLT2 Inhibitors
SGLT2 inhibitors (such as empagliflozin, dapagliflozin, and canagliflozin) provide a unique approach to lowering blood glucose levels without increasing insulin doses. They work by blocking glucose reabsorption in the kidneys, allowing excess glucose to be excreted in urine, which helps reduce glucose toxicity and insulin resistance.
Key actions:
- Lower glucose toxicity by reducing overall glucose burden: By excreting glucose through urine, SGLT2 inhibitors help prevent excess glucose from accumulating in the bloodstream, reducing insulin resistance over time.
- Block glucose reabsorption in the kidneys: Normally, the kidneys reabsorb glucose back into the bloodstream. SGLT2 inhibitors interrupt this process, allowing glucose to be eliminated instead.
- Help reduce glucose burden and insulin doses: Unlike other glucose-lowering therapies, SGLT2 inhibitors do not increase insulin production or require additional insulin administration. In fact, losing 40-120g per day of glucose in the urine can markedly reduce insulin requirements.

However, SLGT2s are not always offered to people who live with T1D due to increased DKA risk. So, your Doctor and you should consider reading this excellent opinion of SGLT2s for T1D. It highlights;
- Increased risk of diabetic ketoacidosis (DKA): SGLT2 inhibitors can lower insulin levels while still allowing glucose to be excreted, potentially increasing ketone production. This can raise the risk of euglycaemic DKA (normal blood glucose but high ketones), which requires careful monitoring.
- Stay well-hydrated: Increased urinary glucose loss can lead to dehydration, making proper fluid intake essential to prevent complications.
- Monitor ketones regularly: Since SGLT2 inhibitors can increase ketone production, it’s important to check ketone levels, especially during illness, fasting, or periods of low carbohydrate intake.
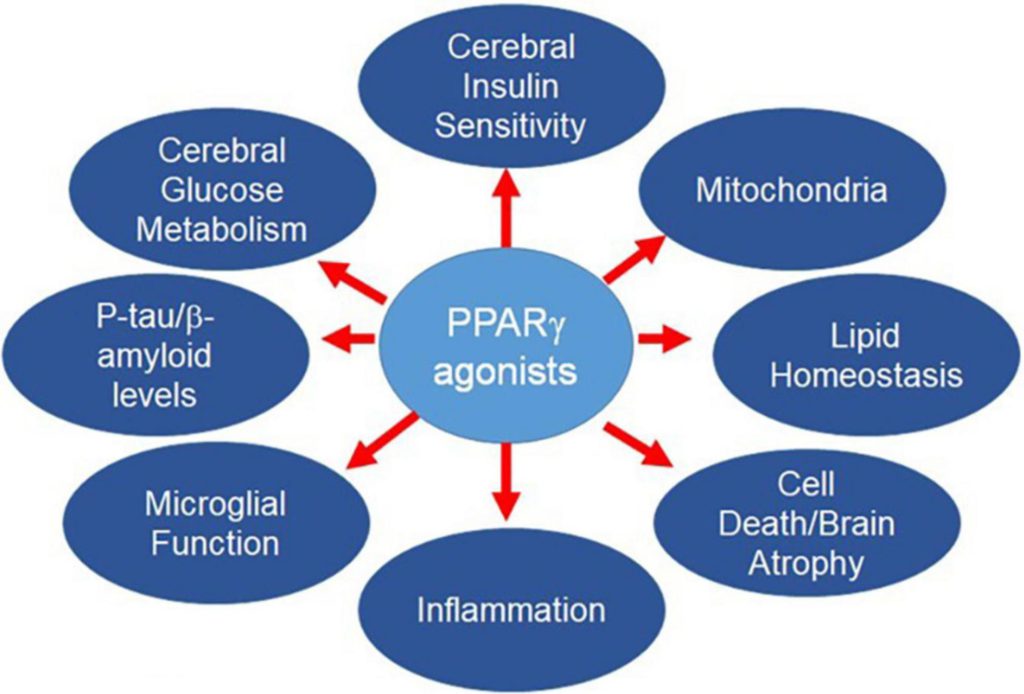
6. Pioglitazone (Actos)
Pioglitazone is a PPAR-gamma activator that plays a unique role in insulin sensitivity by redistributing fat from harmful locations (such as the liver and muscles) back into subcutaneous fat stores, where it is less metabolically damaging. Despite being misunderstood and often overlooked, pioglitazone offers significant benefits for improving insulin signalling and reducing insulin resistance.
Key actions:
- Improves insulin sensitivity by redistributing fat properly: Excess fat in the muscles, liver, and pancreas contributes to insulin resistance and metabolic dysfunction. Pioglitazone helps move fat away from these critical organs into safer subcutaneous fat stores, where it has a lower impact on glucose metabolism.
- Enhances insulin signaling: By reducing intramuscular and liver fat, pioglitazone helps restore proper insulin action, making insulin more effective at regulating blood sugar.
- Lowers liver insulin resistance: Pioglitazone reduces hepatic fat accumulation, preventing excess glucose production by the liver, which is a major contributor to high fasting glucose levels.
- Reduces systemic inflammation: By addressing metabolically harmful fat storage, pioglitazone helps lower chronic inflammation, which is a key driver of insulin resistance.

Some considerations:
- It does not cause “true” weight gain: While pioglitazone shifts fat storage, leading to an increase in total body weight, this is due to redistribution rather than fat accumulation. The metabolic benefits outweigh the change in scale weight.
- Monitor for fluid retention: In some cases, pioglitazone may cause mild fluid retention, which should be monitored, especially in individuals with heart conditions.
- Takes time to show effects: Unlike rapid-acting glucose-lowering therapies, pioglitazone works gradually by improving fat metabolism and insulin sensitivity over weeks to months.
- Best used alongside strength training: Since it redistributes fat rather than burning it, pairing pioglitazone with resistance training and a high-protein diet helps preserve muscle mass and optimise body composition.
7. Metformin
Metformin is often thought of as a general insulin sensitiser, but its effects are limited to the liver because muscle tissue lacks the necessary organic cation transporter required for metformin uptake. This means it does not directly improve muscle insulin sensitivity, which was a surprising revelation. Cheers to Dr. Ralph DeFronzo for his groundbreaking mechanistic studies!
For years, I taught that metformin works like oil on a rusty lock, helping muscle cells respond better to insulin. However, after listening to Peter Attia’s podcast, I’ve come to realise that metformin’s action is entirely liver-based, making me a better educator in the process!
How metformin works in the liver:
- Reduces fat oxidation by inhibiting energy production through the electron transport chain (Complex 1).
- Forces the liver to use glucose instead of fat for energy, which increases glucose consumption and reduces glucose output into the bloodstream.
- Lowers blood glucose levels by decreasing hepatic glucose production, preventing glucose toxicity.
Why metformin isn’t the best first-line option for T1D but will be beneficial in a multi-drug approach:
- No direct impact on muscle insulin sensitivity—any benefits in insulin resistance are secondary and largely due to modest weight loss (often from reduced appetite and GI side effects).
- Insulin-lowering effects are mild. Research suggests it may reduce daily insulin needs by about 5%, which is helpful but not transformative.
- It’s cheap and has a fantastic safety profile, making it a reasonable option for a multi-drug approach. but it’s not a first, second, or even third-line treatment for improving insulin sensitivity in T1D.
Insulin resistance is a multi-faceted problem that needs a combination approach
If there’s one key takeaway from this, it’s that insulin resistance in T1D isn’t just about insulin. It’s about the bigger picture. How you move, eat, sleep, and manage stress all play a role. Small, consistent changes in these areas can have a significant impact, improving insulin sensitivity and making diabetes management that bit easier.
So, whether it’s adjusting your nutrition, being more intentional with movement, or prioritising recovery, the goal isn’t perfection, it’s progress. And every small step counts. If lifestyle is not enough, you now know which drugs to discuss with your doctor!
A final reminder of the Octet and how to overcome them!

Hope this was helpful
John
