

As a presenter at the ISPAD 2023, I had the opportunity to delve into the practical application of the ISPAD Exercise 2022 guidelines, intricately combining scientific insights with clinical artistry. For those interested, my talk is accessible for download.


During the conference, I meticulously compiled notes, now available for thorough review in a comprehensive 35-page document, complete with linked references. Yet, with the intention of driving actionable change, I’ve distilled these insights into five immediately implementable Type 1 Diabetes (T1D) management tips, along with a glimpse into evolving trends that are shaping the future of T1D care.
Five Actionable T1D Management Tips
- Automated Insulin Delivery (AID) Systems and Carb Counting: One study shows while accurate carbohydrate counting optimises AID systems (70-75% time in range), fixed carb estimates for standard meals perform commendably (65-70% time in range) with no increase in hypoglycemia. Notably, the Beta-Bionics pump simplifies this by only requiring meal size and type, benefiting those who forgo precise carb counting.
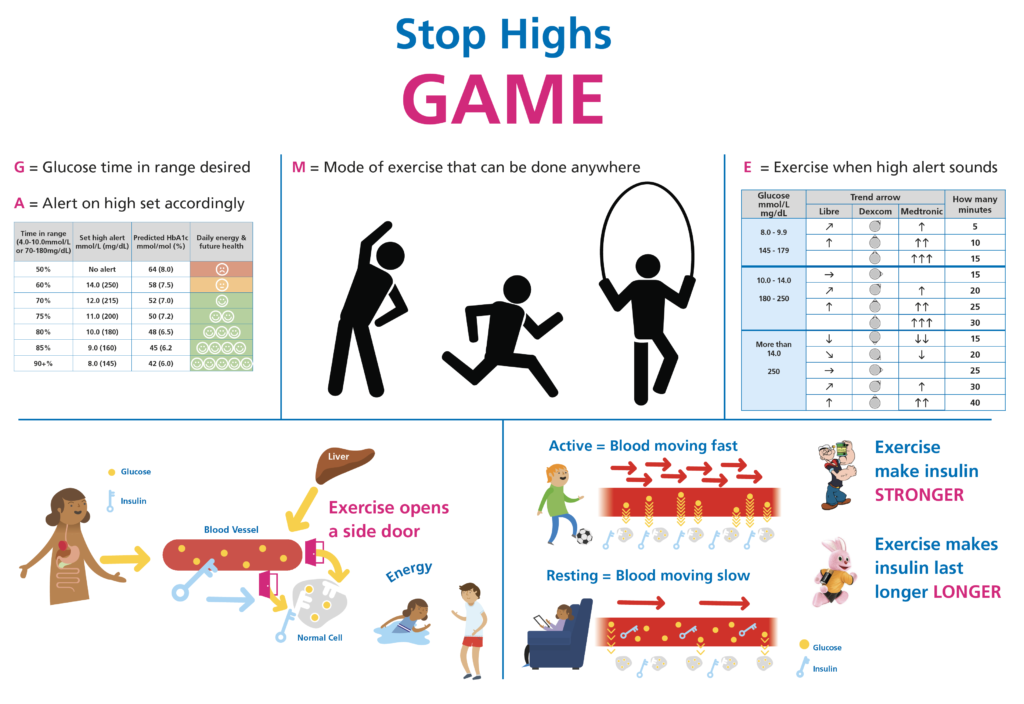
- Managing Postprandial Glucose Peaks: 10 minutes of moderate activity post-meal can reduce glucose levels by approximately 2 mmol/L (40 mg/dL). Our study shows this strategy, though not universal, helps individuals without AID systems achieve a 70% time in range. The theme of physical activity as a secret weapon for T1D was emphatically highlighted by Dessi Zaharieva from Stanford and Jennifer Sherr from Yale. Dessi demonstrated that the more steps you take in the first year after diagnosis, the better your blood glucose control becomes. Jennifer reminded everyone that if achieving 60 minutes of activity and two strength training sessions per week were a medication, people would be doubling their doses from age 2. So, the message is straightforward: the more active you are, the better your blood glucose control and overall health.

- Early AID System Adoption: Studies show initiating AID systems from diagnosis improves time in range at 1 and 2 years, despite not preserving c-peptide or extending the honeymoon phase. This suggests a positive long-term impact on health, making it advisable for most.
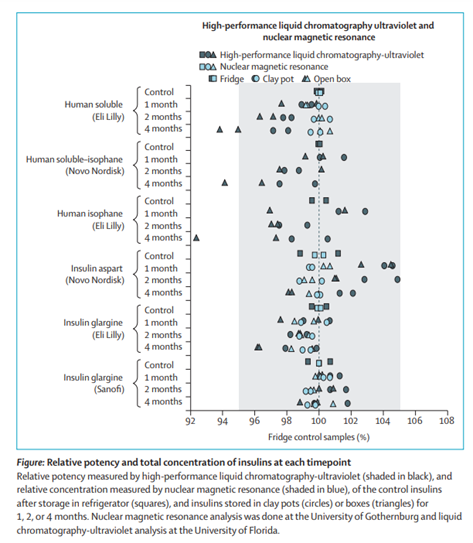
- Insulin Viability Post-Storage Guidelines: Research challenges the notion that insulin loses potency 28 days post-refrigeration. Findings indicate that insulin remains over 95% potent even after four months at temperatures up to 33°C, calling for a re-evaluation of current guidelines.
- Effective Communication in Consultations: The language used in consultations holds significant weight. Phrases such as “people with diabetes” versus “diabetics” matter, as does avoiding terms like “healthy controls” when they are not factually accurate descriptions. Furthermore, a simple opening of “Thank you for coming today, what would make this appointment a good use of your time?”, helps set the tone.
Emerging Trends in T1D
- Preservation of C-Peptide: Immuno-modulating therapies (Teplizumab) show promise in delaying T1D stage 3 by 2.5 years, with U.S. licensure for ages eight and up. Screening programs for early-stage T1D are underway, hinting at a future where multiple agents may dramatically prolong T1D onset. Read this excellent summary article. It’s important to differentiate between the use cases of cancer and rheumatoid arthritis with T1D – very different long-term prognoses.
- Enhancing AID Systems with Additional Drugs: Adding synthetic amylin or GLP-1 receptor agonists to AID systems has been shown to increase time in range and reduce insulin requirements and weight, signifying potential breakthroughs in T1D management. [Clinical trials]
My Diatribe on the above (stop here if you don’t like speculation, curiosity, and fanciful thinking)
Physical activity and T1D.
As an optimist, I’d like to believe that this information alone should convince everyone to take action. However, I know our obesogenic environment is too influential for simple education. So, what’s the solution? If I were appointed as the head of public health policy, here’s my plan:
Step 1: Every primary school should incorporate a one-mile walk at the beginning of the day and after lunch, 20 minutes each time. This should include teachers and students, with teachers receiving extra pay for the additional 40 minutes of daily activity, promoting better health (win-win).
Step 2: Carefully document the improvements in health and well-being resulting from these initiatives.
Step 3: Implement the same approach in secondary schools.
Step 4: Extend this program to public sector workers.
Step 5: Private industries and insurance companies won’t require much persuasion; the evident cost savings from improved health would be undeniable. Since they focus on their bottom lines, the long-term savings would be irrefutable.
However, returning to reality, we must continue to set an example and educate people about the benefits of 60 minutes of daily activity and two weekly strength training sessions. Perhaps someday, the government will prioritise prevention over investing in treatments with limited upside. Although, it’s less likely in a four-year governmental system.
Language Matters.
I am a type 1 diabetic and work as Dietitian supporting “people living with type 1 diabetes”. I have been debating this over in my head. Here’s a pique into the nonsense up there.
Debate on Language and Representation in Diabetes Care
Opening Statement – Affirmative Side
Moderator: “Today, we engage in a timely debate on how we address and refer to people with diabetes in both clinical settings and research. Our affirmative side argues for a conscious shift in language to avoid objectification and for accurately describing control subjects in studies.”
Affirmative Speaker: “Thank you for this opportunity. It’s essential we recognise the power of language in healthcare. When we refer to ‘people living with diabetes,’ we acknowledge their humanity first, rather than defining them by their condition. Moreover, the term ‘healthy controls’ in research is misleading, as health is subjective. For example, as someone living with type 1 diabetes, my health markers are exemplary. We advocate for descriptors such as ‘participants without diabetes,’ which are statistically and ethically more appropriate.”
Opening Statement – Opposition Side
Moderator: “The opposition may now present their viewpoint.”
Opposition Speaker: “While we understand the intent behind the affirmative’s stance, we must consider the practical aspects of medical and research communication. Terms like ‘diabetic’ are not meant to objectify but to communicate efficiently in fast-paced environments. Additionally, the term ‘healthy controls’ is a technical classification within research contexts, not a subjective assessment of overall health.”
Rebuttal – Affirmative Side
Affirmative Speaker: “Efficiency should not come at the cost of dignity. It’s about evolving our language to reflect the respect and empathy that people deserve. Furthermore, research must evolve to represent reality accurately. If a participant living with diabetes can have better health markers than people non-living without diabetes, our terminology in studies must reflect that to avoid bias.”
Rebuttal – Opposition Side
Opposition Speaker: “The call for language evolution, while noble, overlooks the societal context in which these terms are used. They have specific meanings in medical and research lexicons that are not intended to dehumanise. The term ‘healthy’ in research delineates a group without the condition being studied, nothing more. We risk complicating communication by overanalysing these terms.”
Closing Statement – Affirmative Side
Affirmative Speaker: “Our debate today touches the very core of humanity in healthcare. We must not underestimate the impact of words. As the field progresses, so must our language to encapsulate respect, accuracy, and empathy. It’s not merely about political correctness; it’s about the fundamental way we view and treat people within our care.”
Closing Statement – Opposition Side
Opposition Speaker: “Healthcare’s primary goal has always been to provide the best care and outcomes. While language is important, the utility and clarity of terms in fast-paced clinical and research environments must be preserved. We can be respectful and empathetic without sacrificing the precision and utility that certain terms provide.”
Moderator: “This concludes our debate. It’s clear that both sides have valid points. Language in healthcare is a powerful tool that can both classify and comfort. It’s a balance between clinical efficiency and the humanity of patient care. The conversation must continue, keeping in mind the ever-evolving landscape of medicine and the individuals at its heart.”
I’ve given you fair warning, so here’s the essence of my viewpoint:
After reading “Coddling of the American Mind,” I’ve become somewhat inclined toward valuing free speech over excessive political correctness. For me, the principle of freedom stands above all.
“Anti-fragility” has been another influential read for me. It’s taught me to see the challenging words and criticism I face as opportunities for personal growth, rather than as threats.
I believe that almost everyone means well but is often under pressure and trapped in language habits formed over decades. Let’s assume that when people unintentionally use objectifying language, they’re not doing it with bad intentions. We should all strive to be more resilient and understanding in the face of such habits.
Immunomodulation for b-cell preservation for T1D stage 2
It makes sense from a medical viewpoint to intervene with the immune system early. This strategy is likely to become common practice in the future.
We might be looking at a future where we give patients with two auto-antibodies a combination of immuno-modulation medications every two to three years over two decades to prevent or push back the onset of T1D stage 3. Yet, this approach might not be implemented for another 10 to 20 years.
The current understanding is that patients receiving cancer treatments or those suffering from rheumatoid arthritis or psoriasis can often take a combination of immuno-modulation medications with few adverse effects. This leads to the proposal that such an approach could be safe for other diseases, like T1D, but it’s crucial to examine the particulars of each case:
a. For severe and disabling conditions such as cancer and rheumatoid arthritis, it’s generally accepted to use aggressive treatments early on. However, T1D isn’t usually as immediately life-threatening, so it’s a different use case. Furthermore, with AID systems, the long-term prognosis is very different from cancer and rheumatoid arthritis.
b. Rheumatoid arthritis and psoriasis treatments never start at the tender age of two. We don’t have much data on what could happen if we begin such early and regular treatments with multiple drugs that modify the immune system.
c. Researching these treatment options for T1D is essential, but we have to distinguish their use in this condition from how they’re used in treating cancer, rheumatoid arthritis, and psoriasis. Our enthusiasm for these new methods must be tempered by the understanding that such interventions could disrupt natural developmental and growth processes.
For those interested in the detailed exposition of the conference, the full annotations and discussions are available in this comprehensive 35-page document,
Cheers
John
