
Conference report
EXTOD 2023: exercise and type 1 diabetes
The critical insights from two days of physiological, metabolic, and management sessions at the EXTOD 2023 conference, plus a framework for thinking about perceived threats and how to be BRAVE.
About this report
The Exercise and Type One Diabetes (EXTOD) conference of 2023 focused on physiological and metabolic responses to exercise and on management strategies to address glucose challenges. Sessions provided a framework for supporting people with type 1 diabetes who want to exercise. The report also covers a psychology session from Dr Josephine Perry on how to be BRAVE.
The physiology of glucose during exercise
Sessions shed light on the interplay between insulin-independent and insulin-dependent pathways that affect glucose uptake during exercise. GLUT-4 translocation can occur independent of insulin, which, when combined with insulin-dependent uptake, significantly raises the risk of hypoglycaemia during physical activity.
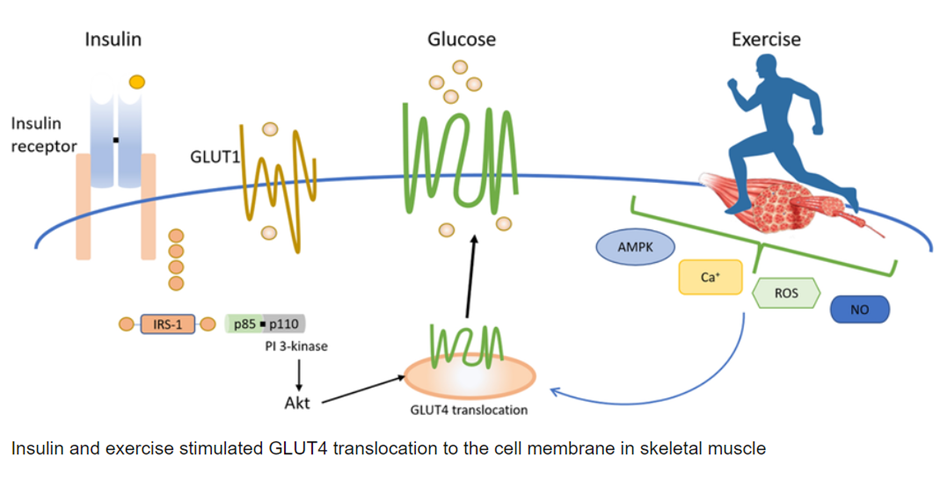
A primary concern discussed was the impact of subcutaneous insulin, which has an extended half-life that results in peripheral insulin levels being 2.5 to 4 times higher in people with type 1 diabetes compared to those without the condition. This peripheral insulin acts like a sledgehammer against the adrenaline and glucagon response, particularly when large amounts of insulin are present in the blood.
Interestingly, when only basal insulin levels are present and no bolus insulin has been given in the last 3 to 4 hours or while fasting, an adrenaline surge from high-intensity exercise can trigger a glucose rise due to liver glycogenolysis. This mechanism matters when interpreting unexpected glucose rises during intense effort.
Factors associated with glucose drops during exercise
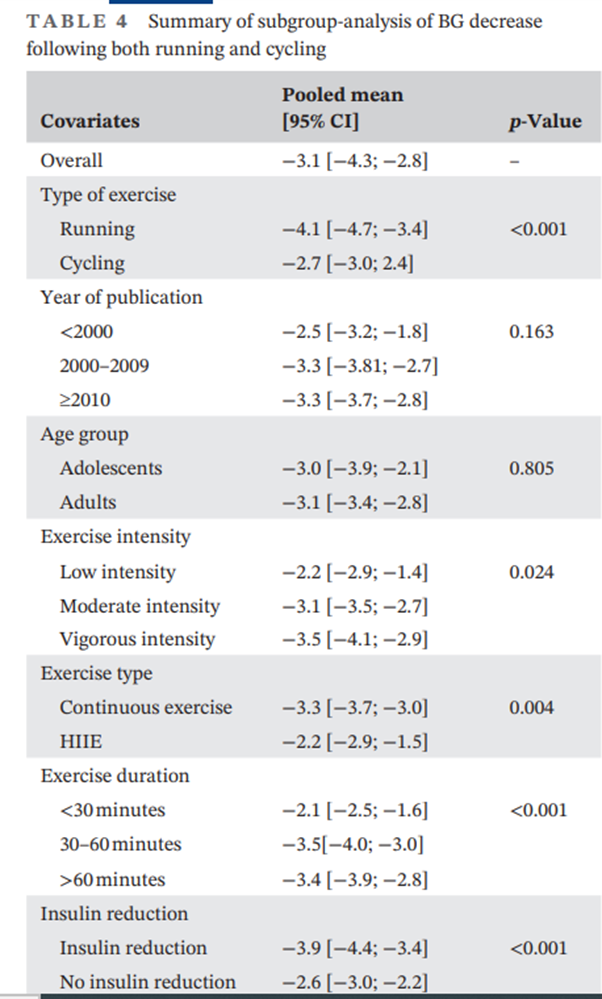
An analysis of clinical trials pinpointed several factors leading to significant glucose level drops during exercise. According to Eckstein et al.’s 2023 study in Diabetic Medicine, running was found to cause greater glucose reductions compared to cycling, due to the engagement of more muscle groups. Both the duration and intensity of exercise were directly proportional to the extent of the glucose drop.
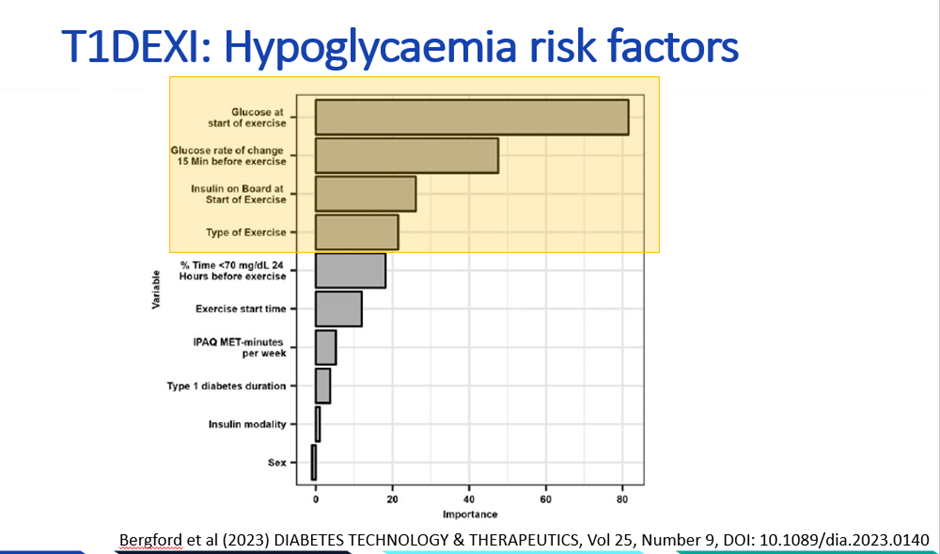
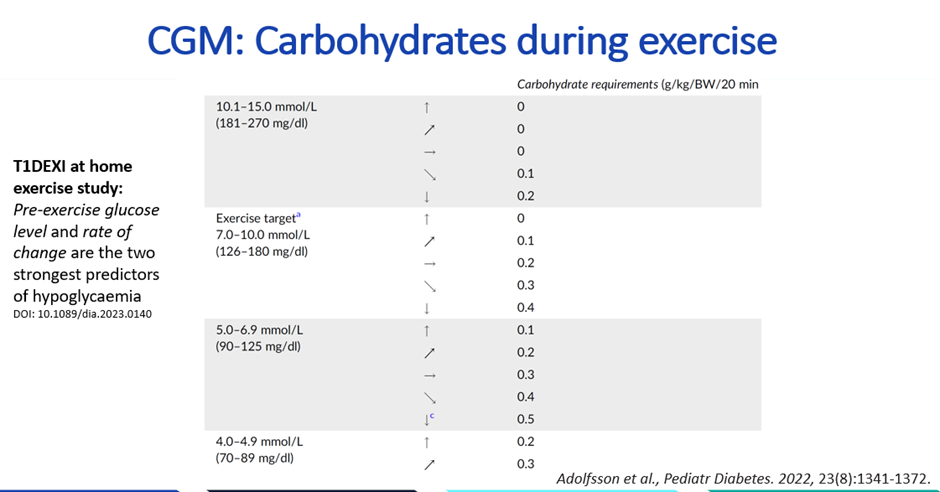
Real-world evidence from Bergford et al. 2023, involving close to 500 adults with type 1 diabetes recording nearly 10,000 exercise sessions, identified four predominant factors associated with hypoglycaemia risk, in order of importance.
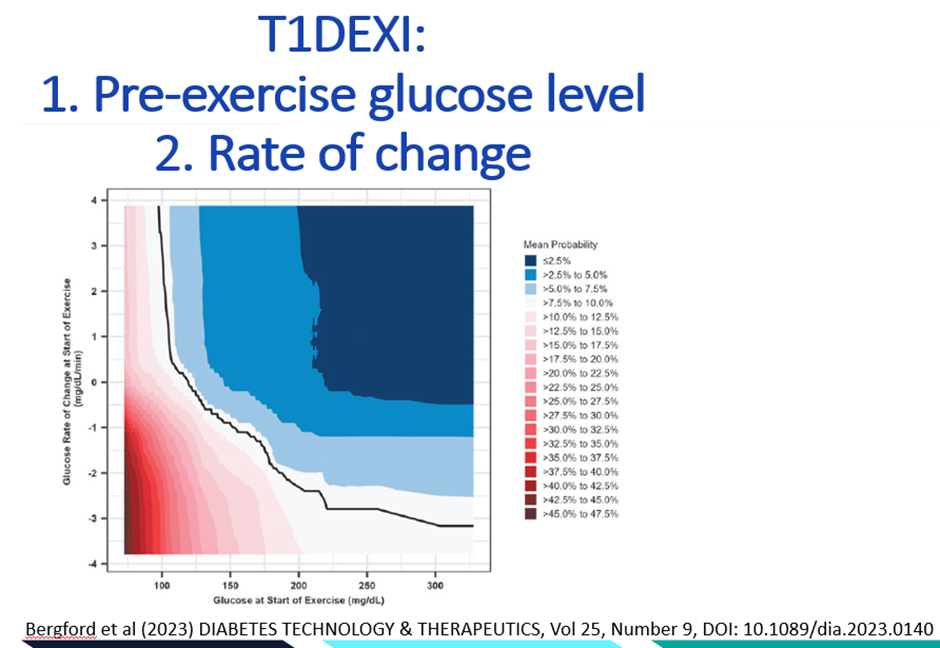
- The pre-exercise glucose level
- The rate of glucose change as indicated by CGM trend arrows
- The amount of insulin on board
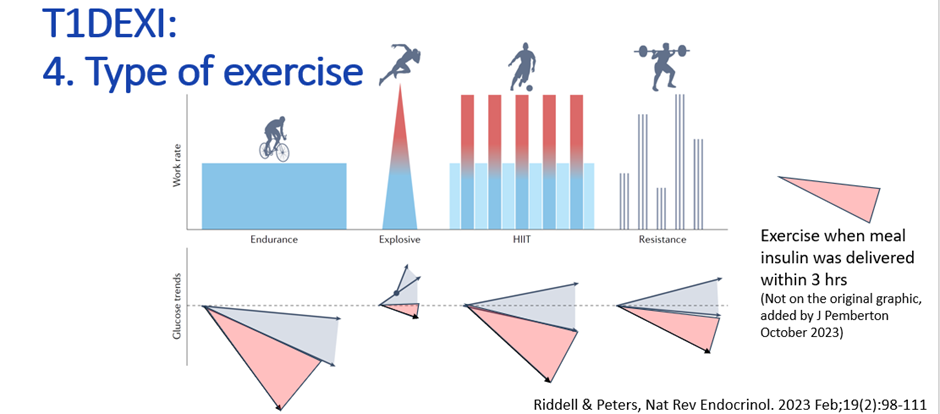
- The type of exercise performed
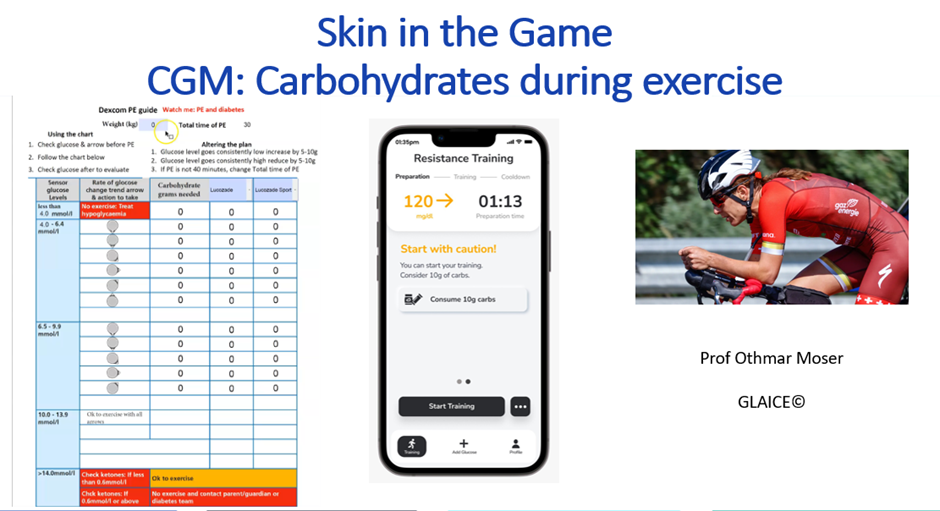
Carbohydrate needs during exercise
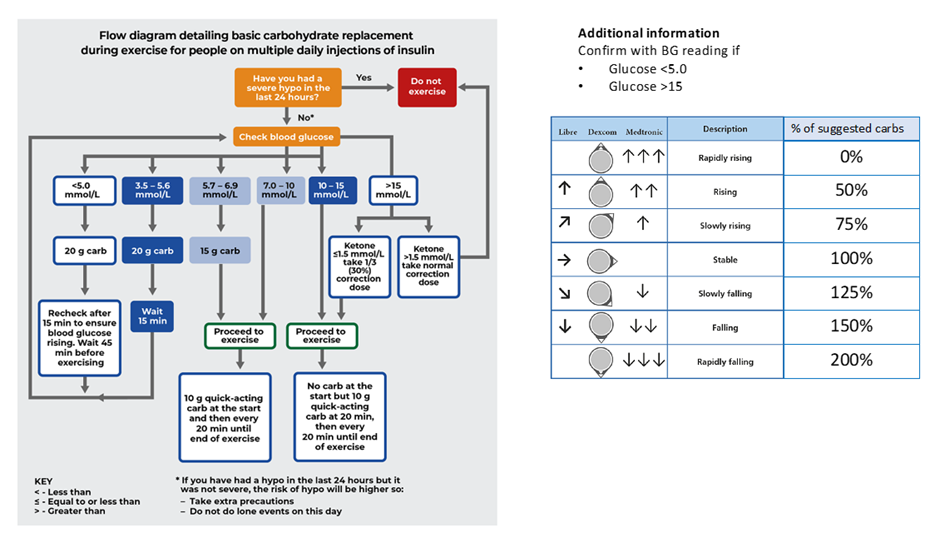
Several management strategies were presented. A key question is how much carbohydrate is needed when using blood glucose testing and CGM. The EXTOD advice is shown below.
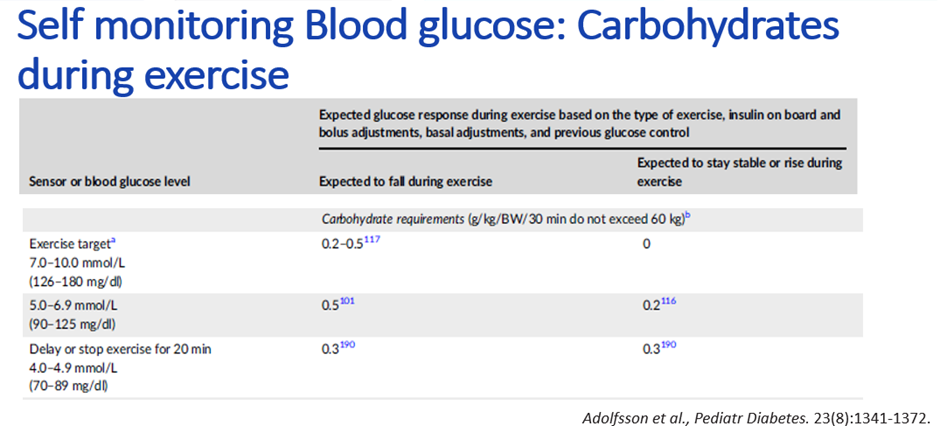
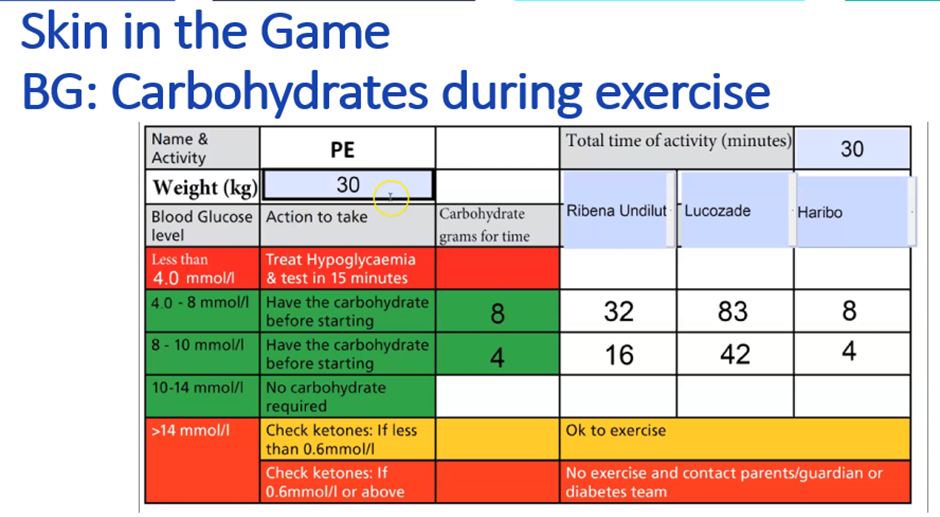
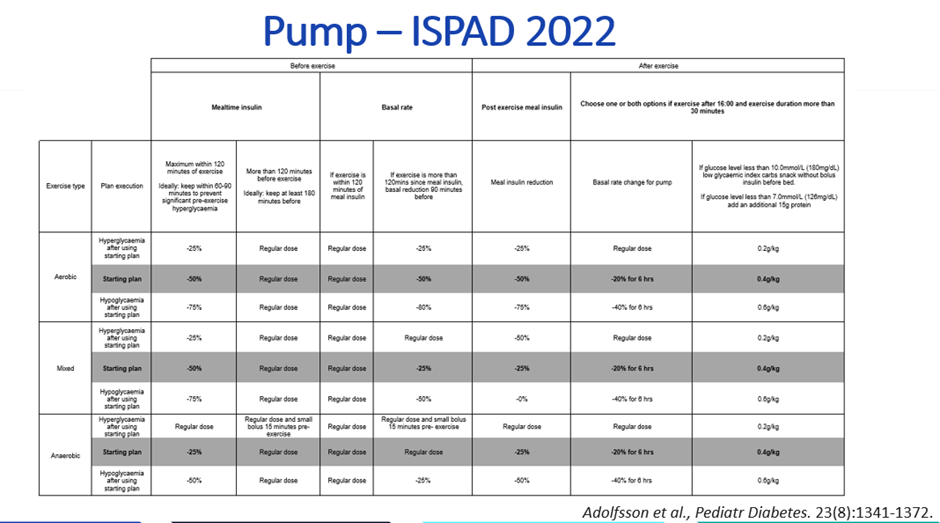
The ISPAD 2022 Exercise Guidelines carbohydrate amounts for those using finger prick testing are below, along with how to implement them practically.
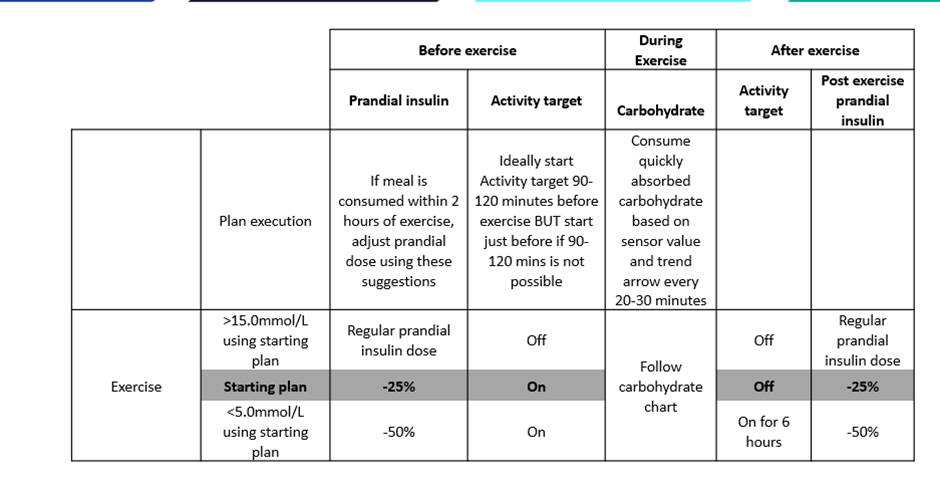
The ISPAD 2022 Exercise Guidelines carbohydrate amounts for those using CGM are shown below.
Here is how to implement it practically. The exercise carbohydrate calculators can be downloaded — you will need Adobe Reader for computer, Android, or Apple device.
- Dexcom G6 — Exercise Carbohydrate Calculator
- Libre 1 and 2 — Exercise Carbohydrate Calculator
- Medtronic — Exercise Carbohydrate Calculator
- Dexcom G6 with pump — Exercise Carbohydrate Calculator
Insulin on board and timing around exercise
Then it is all about insulin on board. The key patterns to understand:
- Aiming to have the last meal and insulin three hours before exercise tends to produce the most consistent glucose levels
- If eating within 2 hours of exercise, reducing the usual dose by around 50% is a common starting point for exploration
- Where possible, exercising within 60 minutes of insulin reductions can help prevent glucose rising too high before starting
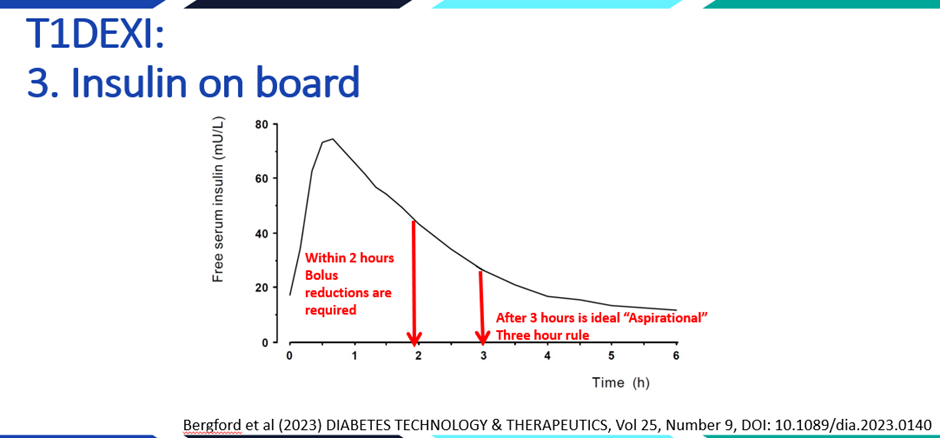
The type of exercise matters, but if exercise occurs within two hours of bolus insulin, glucose is very likely to drop regardless of exercise type.
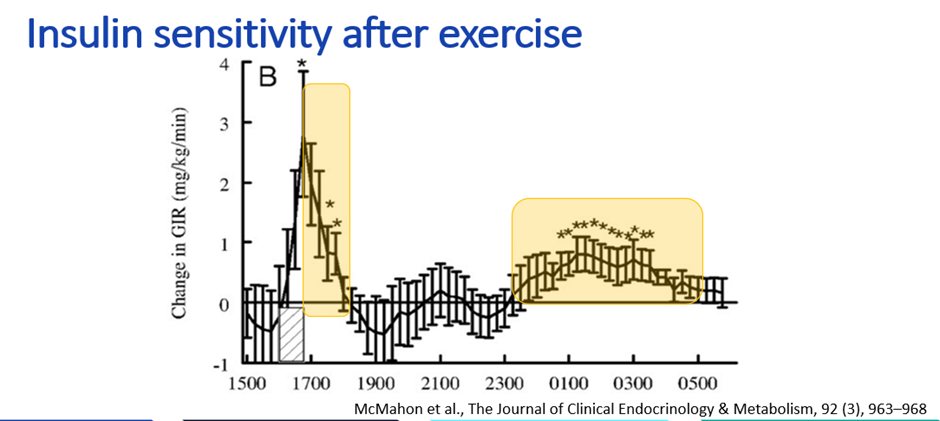
Insulin sensitivity tends to be high immediately after exercise. A 50% insulin reduction at the meal after exercise is a common starting point for exploration. For exercise after 4 pm, a 20% reduction in background basal insulin, or 20g of carbohydrates without fast-acting insulin before bed, may be worth exploring when glucose is below 10 mmol/L. When glucose is below 7 mmol/L before bed after evening exercise, adding 10 to 20g protein may also be useful. These patterns vary significantly between individuals and are worth exploring with CGM data and your care team.
A useful starting framework is 50/50/20 combined with this table from the ISPAD Guidelines 2022.
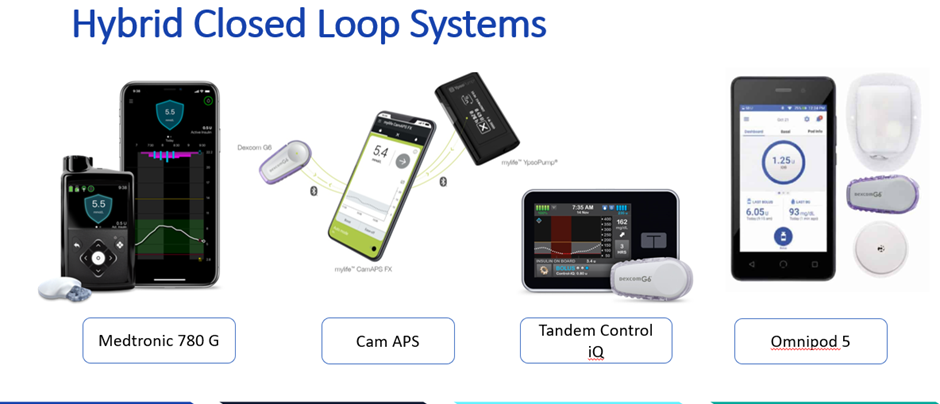
Hybrid closed-loop therapy and exercise
Exercise plans with hybrid closed-loop systems share some principles with manual therapy, but the algorithm changes what is possible and what is needed. This publication led by Dessi Zaharieva is excellent for practical top tips.
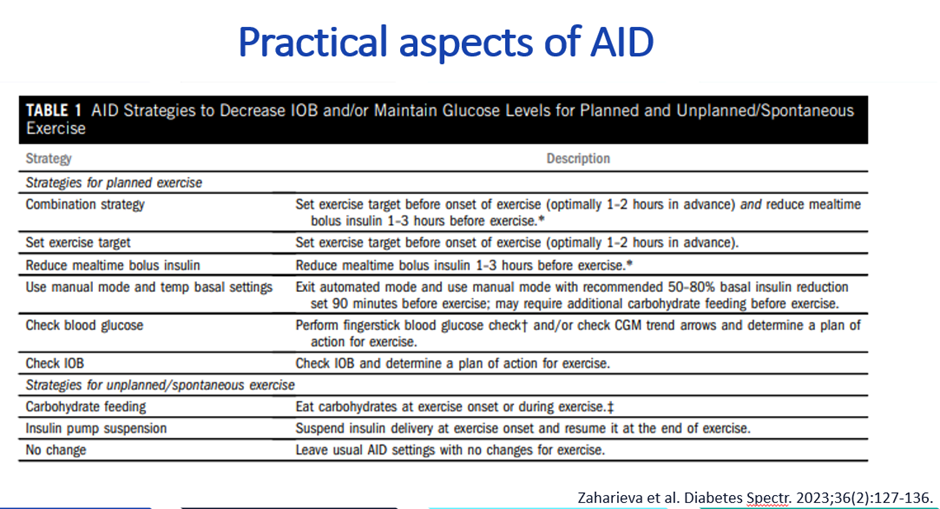
A simplified algorithm for getting started:
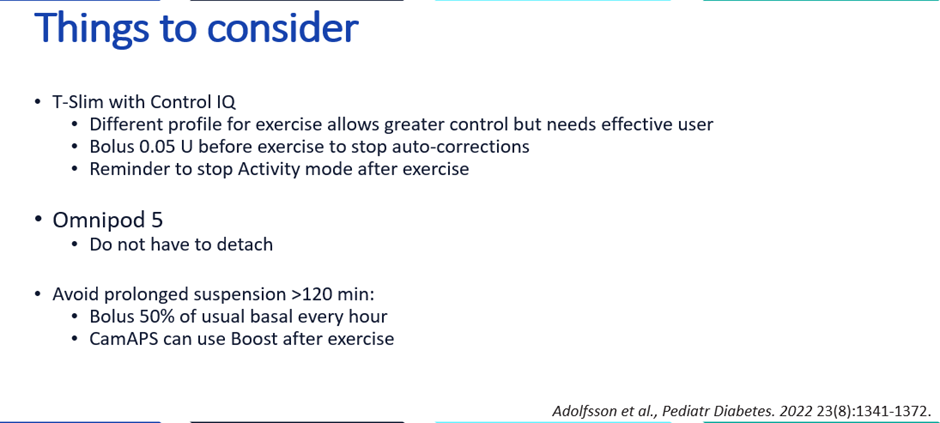
Device-specific considerations for hybrid closed-loop systems and exercise:
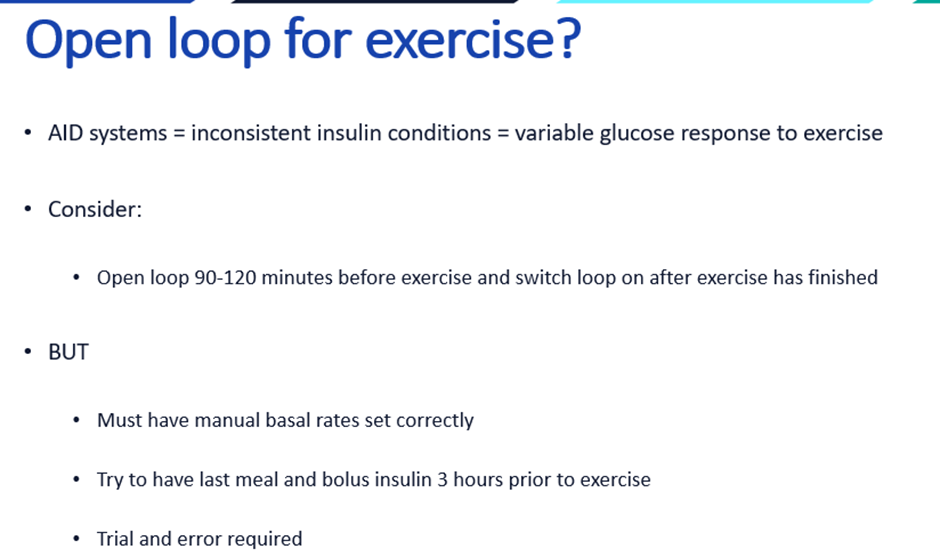
People who already have well-established exercise plans may benefit from switching to open loop two hours before starting exercise. This allows more certainty about the insulin conditions going in, which tends to produce more reproducible glucose responses for the same plan. Switching the loop back on after exercise then allows the algorithm to help reduce the hypoglycaemia risk in the recovery period.
For more detail, the EXTOD website contains excellent information to support people with type 1 diabetes to manage exercise.
Psychology session: Josephine Perry — how to be BRAVE
Dr Josephine Perry explored how the amygdala perceives threats, which are then addressed either rapidly through habit or more deliberately through decision-making. When the brain’s wiring has a low threshold for perceiving something as a threat, and habits responding to these threats become established, significant anxiety can result. The key is to become more conscious of perceived threats and to contemplate them more thoroughly, aiming to develop a new habitual relationship with how threats are perceived. This requires dedicated effort.
- Threat: The amygdala predicts threats, triggering fight or flight responses.
- Habit: The mid-brain operates automatically, forming habits in roughly 66 days.
- Decision: The pre-frontal cortex is involved in slower, more deliberate decision-making.
Factors contributing to a low threshold for perceiving threats include previous trauma, overthinking, perfectionism, judgmental attitudes, external rewards, recent failures, fear of failure, and a strong self-identity as an athlete. Situational factors include hunger, tiredness, low glucose levels, and having values violated.
The BRAVE framework
- B — Be aware of your worries and verbalise what the amygdala is signalling, creating a sense of safety.
- R — Reassign these worries to your safety seekers and create characters for them, such as “Lazy Larry” or “Imposter John”.
- A — Advocate for yourself using positive affirmations at a ratio of 5 to 1 to counteract negative thoughts.
- V — Focus on your values; identify your top three, such as fairness, challenge, and progress.
- E — Engage in simple strategies to combat anxiety, such as breathing exercises, grounding, CBT strategies, smiling, and chunking.
Special thanks to Josephine Perry for these insights. By envisioning an imaginary character for your perceived threats — like “Imposter John” — it becomes possible to think more slowly about those threats, face them, and act despite them. Strong convictions, loosely held.
The educational frame
- All management strategies described here reflect population-level patterns and averages from research, not individual predictions
- Individual responses to exercise, insulin timing, and carbohydrate intake vary significantly
- The frameworks described are starting points for exploration with your own CGM data
- Discuss any changes to exercise management with your diabetes care team
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.