The five UK AID systems, side by side
Automated Insulin Delivery Systems
In clinic, the question almost never lands as “Which system?”. It lands as “Which one fits the life I am already living?”. Five systems, four different algorithm families, all clinically meaningful step-changes over manual dosing. Picking between them is a conversation about you, not a league table.
Ask Grace
Want to ask which AID system might suit your life, or how the algorithms compare on the things you care about? Ask Grace.
What an AID system does
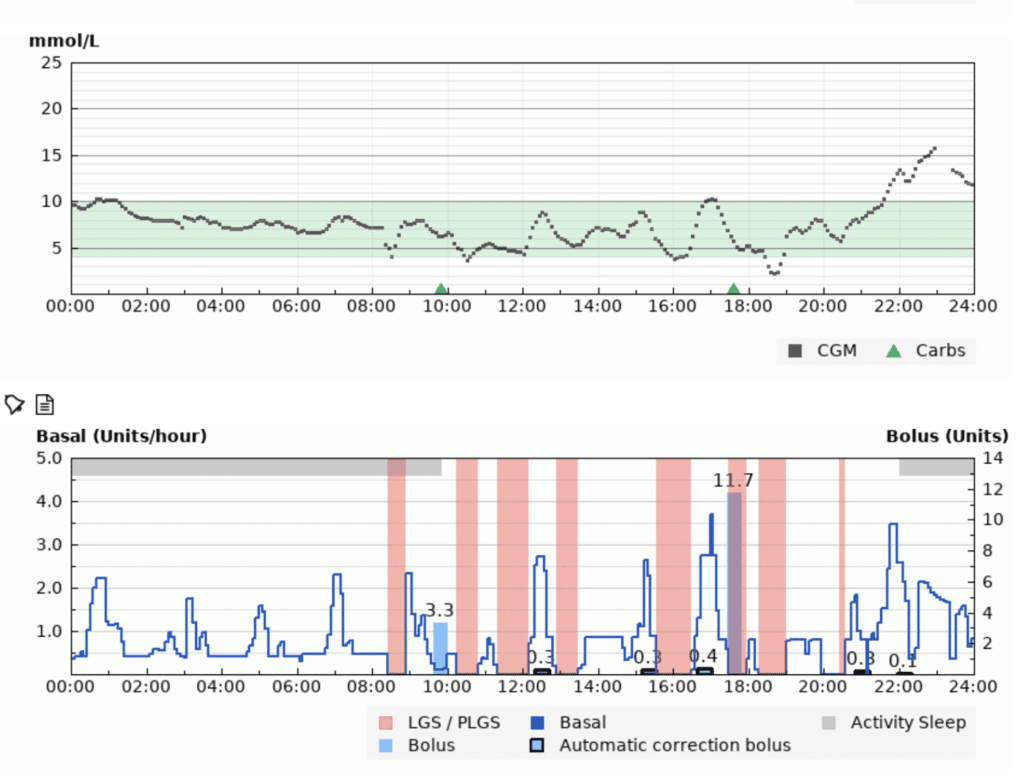
An AID system is three things working together: an insulin pump, a CGM, and an algorithm that adjusts insulin every few minutes. When glucose is predicted to rise, the algorithm pushes more insulin (extra basal, sometimes a small auto-correction). When glucose is predicted to fall, it eases off or suspends. You still bolus for meals; the system covers what sits between them.
From DAFNE clinic the line that lands hardest is rarely about the pump. It is about sleep. Eight hours back. Fewer overnight hypos. Fewer wake-ups high. Flatter overnight lines for the person living with T1D, and for the parent listening for the alarm.
The five UK-available systems in 2026 are Tandem t:slim X2 with Control-IQ, Tandem Mobi (CIQ+), MiniMed 780G, CamAPS FX, and Omnipod 5. Every system covered here is a hybrid closed-loop; you still bolus for meals, the algorithm covers the rest. The foundations still apply on every one of them: balanced meals, accurate carb counting, bolusing 10 to 20 minutes before eating. AID is a substantial layer on top, not a replacement.
What improvement to expect
On CGM alone, time in range (3.9 to 10.0 mmol/L / 70 to 180 mg/dL) typically sits around 40 to 60%. On AID, around 60 to 90%. The typical lift is 10 to 30 percentage points versus baseline, and the larger gains tend to arrive for the people starting from a lower TIR. The lift comes with less micromanagement, not more: fewer corrections through the day, fewer hypo treatments, fewer “what now” decisions at 2pm.
The trade-off you are choosing between systems. No matched-population study shows one system delivering significantly more TIR than another. The factors that drive outcomes are the basics done well, the settings tuned with the team, and the system used consistently. The differences between the four are about how the algorithm gets there, what it asks of you, and how the device fits your life.
Hidden superpower: sleep
The most consistent win from AID is overnight. Eight hours back where the algorithm holds the line is eight hours of cognitive bandwidth returned the next day. Parents notice it first; adults notice it within a week. The trial data shows the same pattern: most TIR gain on AID lands in the overnight window, where meal management is not in play and the algorithm is doing what algorithms do best.
The five UK AID systems at a glance
Read the guide on each system, then try the quiz; nine out of ten earns a certificate.
Tap a system to expand. The first is open by default.
Tandem t:slim X2 with Control-IQ
Algorithm: 30-minute predictive horizon, both basal modulation and automatic correction boluses (Autobolus, up to once an hour). CGM: Dexcom G6 or G7. Distinctive: dual-channel automation (basal AND bolus), fixed 5-hour AIT so on-screen IOB is a reasonable physiological proxy. Best fit: people who want algorithm strength with IOB visibility, particularly useful around exercise.
Tandem Mobi (CIQ+)
Algorithm: the same Control-IQ family algorithm, lever values match t:slim Control-IQ at every level. CGM: Dexcom G6 or G7. Distinctive: Tandem’s tubeless miniature pump form factor; algorithm behaviour is identical to Control-IQ, only the hardware differs. Best fit: people who want Control-IQ’s algorithm with a smaller, tubeless body. The Optimiser carries Mobi as its own row alongside Control-IQ.
MiniMed 780G
Algorithm: SmartGuard, fully closed-loop with 5-minute auto-corrections. CGM: Guardian 4, Simplera Sync, or Instinct (Abbott-made for MiniMed, 15-day, CE Mark March 2026). Distinctive: the most automated high-glucose response of the four; AIT is the dominant lever (2 to 3 hours), shorter AIT means stronger corrections and a lower target. Best fit: people who want the algorithm to do more of the work and are happy to bolus consistently for meals.
CamAPS FX
Algorithm: Cambridge Adaptive Algorithm, runs on an Android phone, drives a Ypsomed YpsoPump, Sooil Dana-i, or Tandem t:slim X2. CGM: Dexcom G6 / G7, FreeStyle Libre 3. Distinctive: the most adaptable algorithm, customisable target (4.4 to 11.0 mmol/L), Boost and Ease-Off modes, the deepest evidence base in young children and pregnancy. Best fit: children, families, pregnancy, and adults who want a target they can tune.
Omnipod 5
Algorithm: SmartAdjust, runs on the Pod itself so dosing continues even when the phone is away. CGM: Dexcom G6 or G7. Distinctive: tubeless, waterproof, the algorithm sits on-body; target adjustable 6.1 to 8.3 mmol/L; like the 780G, uses a shorter AIT to enable more frequent corrections. Best fit: people who want a tubeless system, simple day-to-day operation, and minimal kit on a busy day.
AID Systems Knowledge Check
Try the assessment on this page any time, before you explore the pump guides below or once you have worked through them. It is a quick way to see where the gaps are in the AID essentials, and 9 out of 10 earns your certificate.
Find your top two: the AID selector
Pick the three things that matter most to you. The selector scores each system against your priorities and shows your top two as a starting point for the conversation with your team.
Check CGM compatibility first. Every UK AID system needs a CGM, and not every system pairs with every CGM. If you already use one (or plan to), that often narrows the field straight away.
Select 3 priorities (0 of 3 chosen)
What the head-to-head evidence shows
The honest answer to “which system is best?” is the same answer the trials keep giving back: in matched populations, no system delivers significantly more TIR than another. Gera 2025 ran Omnipod 5 against Control-IQ in 272 young people; 90-day TIR around 62 to 64% on both. The one finding that did separate the systems was demographic: female participants, non-Hispanic Black participants, and those with public insurance were more likely to choose Omnipod 5. Navas Moreno 2023 (adults, n=97) and Beato-Vibora 2024 (real-world registry) showed the same null pattern across Control-IQ vs MiniMed 780G and Control-IQ vs CamAPS FX. The German-Austrian DPV registry (Karges 2024, n=13,922) confirmed it across age groups: baseline TIR was the strongest predictor of outcome, not which brand was on the pump.
What that means is honest, and worth saying plainly. The conversation with your team is not “which is the best system?”. It is “which system fits how I live, what CGM I already use, what my paediatric centre supports, and what I want the algorithm to ask of me?”.
What holds in children and young people
For a parent the moment that lands hardest is rarely the one in the textbook. It is the half-second pause before a feed at 4am, the school-nurse phone call at 1:15pm, the teenager who leaves the pump in a drawer for three days because they want to feel normal. From the conversations I have in clinic at Birmingham Women’s and Children’s, what families describe is the same pattern with different specifics. Most of the work happens at home, between visits, by the people who never get called diabetes specialists.
The trial spine over the last decade tells a consistent story when you read it as a parent. KidsAP02 (Ware 2022, NEJM) added around two extra hours a day in target on CamAPS FX in children aged 1 to 7, with nighttime time-in-range reaching 82% and time below range unchanged. The Omnipod 5 preschool work landed in the same direction in 2 to 5 year olds: more hours in range, HbA1c down by half a point, no DKA across the trial. Two trials, the same shape of finding.
The honest counterweight comes from the registry. Karges 2024 (Lancet Diabetes Endocrinol) showed hybrid closed-loop cut hypoglycaemic coma but was associated with a higher overall rate of DKA, concentrated in young people with HbA1c above 7.5%. The most likely mechanism is undetected insulin under-delivery, a cannula occlusion or a device failure that goes unnoticed because the algorithm is doing more of the day-to-day adjustment. Reading that as a parent, the answer is not less AID. It is active sick-day rules, ketone-monitoring routines that actually run when the child is unwell, and a low threshold for checking the cannula site.
What changes when the evidence and the family meet is the same pattern as the adult experience: AID does not remove the work, it shifts where the work goes. You watch fewer numbers in the middle of the night. You hold a closer eye on cannula sites and on sick days. You reclaim some of the sleep you have lost. ISPAD 2024 (chapters 16, 17, 23) recommends hybrid closed-loop across all paediatric age bands where available. Decisions about which system and which settings for any individual child are a conversation with your paediatric diabetes team. Ask early, ask in writing if you need to, and ask again if the first answer is “not yet”.
Does ultra-rapid insulin add much on AID?
Ultra-rapid formulations (Lyumjev and Fiasp) absorb faster and clear sooner than standard rapid-acting analogues. Rakab 2025 (Frontiers in Endocrinology, systematic review and meta-analysis of 12 RCTs across six AID systems) found ultra-rapid insulin produced less than 1 percentage point of TIR improvement compared with standard insulin, not statistically significant. The AID algorithm compensates for insulin speed so effectively that the formulation barely changes overall TIR. The benefit, where it is real, sits in reduced glycaemic variability and improved exercise safety margins, not in the headline TIR number. Discuss with your diabetes care team whether either of those is a priority for you.
How to use this guide
Read this overview, then open the system page that fits your shortlist. The system pages explain how each algorithm behaves, what the primary levers are, and how the GNL AID Optimiser maps onto its settings.
Tandem t:slim X2 with Control-IQ (and Tandem Mobi)
Dual-channel automation with Autobolus, fixed 5-hour AIT, IOB visible. Highly customisable when well set up. Tandem Mobi runs the same Control-IQ algorithm on a tubeless miniature pump.
MiniMed 780G
The most automated high-glucose response. AIT is the dominant lever. Lower target at higher algorithm strength.
CamAPS FX
Adaptable algorithm, customisable target, deepest evidence base in young children and pregnancy.
Omnipod 5
Tubeless, on-body algorithm, simple to operate. Adjustable target. Like the 780G, uses a shorter AIT for more frequent corrections.
How this guide was built
Written from clinical practice and personal use of every commercially available AID system between 2017 and 2026, supporting more than 300 children and young people through AID starts at Birmingham Women’s and Children’s NHS Foundation Trust. The 5-level AID Optimiser ladder that runs through the system pages was reviewed and refined with input from CamAPS, MiniMed, Tandem and Insulet global medical leads; it is a Grade D educational synthesis, not a manufacturer endorsement, with a declared bias toward IOB visibility. Any settings change is a conversation with your diabetes care team.