

This could be the most important thing you will ever read about diabetes. It’s the most challenging read so far. However, I will start slow and layer in the complex stuff as we go. Please stick with it. If you understand this, there will be no stopping you.
The Podcast Episode will also be useful – Episode 7: Fundementals of The Glucose Never Lies

Let’s go!
Bolus insulin just means the delivery of fast-acting insulin to cover:
- Glucose from digested carbohydrate; a meal bolus.
- Bringing a high glucose level back into target; a correction bolus.
- Both of these combined.
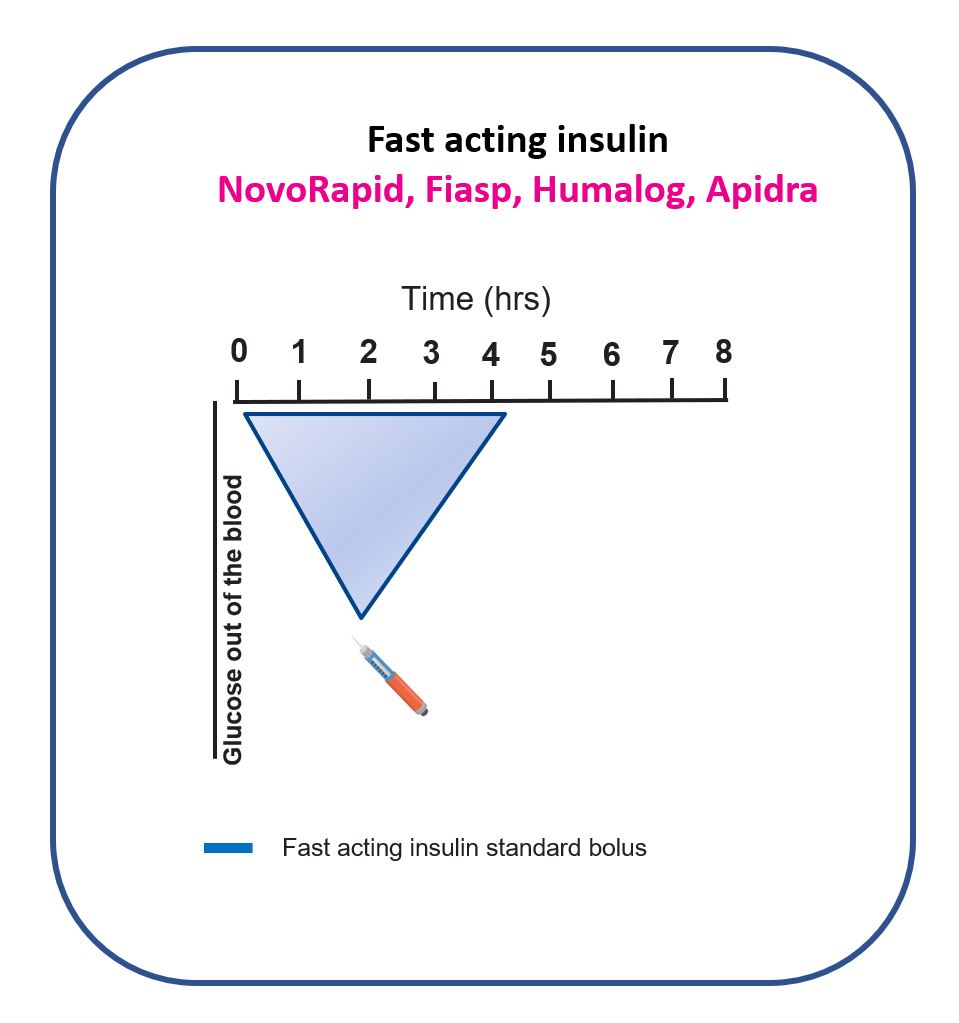
This picture shows how a bolus of fast-acting insulin starts slowly, hits peak action about two hours after delivery, and finishes glucose-lowering by four hours.

How do you match a bolus of fast-acting insulin to the carbohydrate in a meal?
Your diabetes team should teach you to count carbohydrates to the gram. Don’t worry if not, I will teach you soon enough.
You will then be given a few insulin-to-carbohydrate ratios (carb ratio) for the different mealtimes.
Here are my current carb ratios, where u refers to units of fast-acting insulin and g represents grams of carbohydrate:
Breakfast: 1u:15g
Lunch: 1u:25g
Evening meal: 1u:20g
Let’s say I had 50g of carbs at each meal. Here’s the math.
Grams of carbohydrate in meal / grams in the carb ratio = fast-acting meal bolus insulin units
Breakfast: 50g / 15 = 3.3 units
Lunch: 50g / 25 = 2.0 units
Evening meal: 50g / 20 = 2.5 units
Carb ratios vary in strength from person to person. The strength required is determined mainly by physical fitness and daily activity level. The fitter and more active you are, the less insulin you will need, and therefore, the weaker the carb ratios required.
I am physically fit, so my ratios are fairly weak. An unfit 40-year-old would have carb ratios more like 1u:8g.
Carb ratios also vary in strength from meal to meal. It mainly depends on your sensitivity to insulin at different times of the day. Most people are least sensitive in the morning, most sensitive at lunch, and in the middle at the evening meal. You can see my carb ratios follow this pattern.
How do I know if my carb ratios are right for me?
Here are the steps you need to follow:
- No food or bolus insulin in the four hours before the test.
- Make a balanced meal (carbs, protein, veg) with your usual amounts of carbs for that mealtime.
- It cannot be a high-fat meal; these require more insulin, and I will teach you how to deal with these in the Mealtime Insulin Guide.This Podcast Epidsode willbe helpful – Episode 7: Fundementals of The Glucose Never Lies
- Count the carbs accurately.
- Give the insulin before the meal.
- Only usual activity and no corrections in the four hours after eating.
- Review the results using the picture below and make adjustments if required:
- Too weak: Make the carb ratio more aggressive by 10-20%
- Perfect: No changes
- Too strong: Make the carb ratio weaker by 10-20%

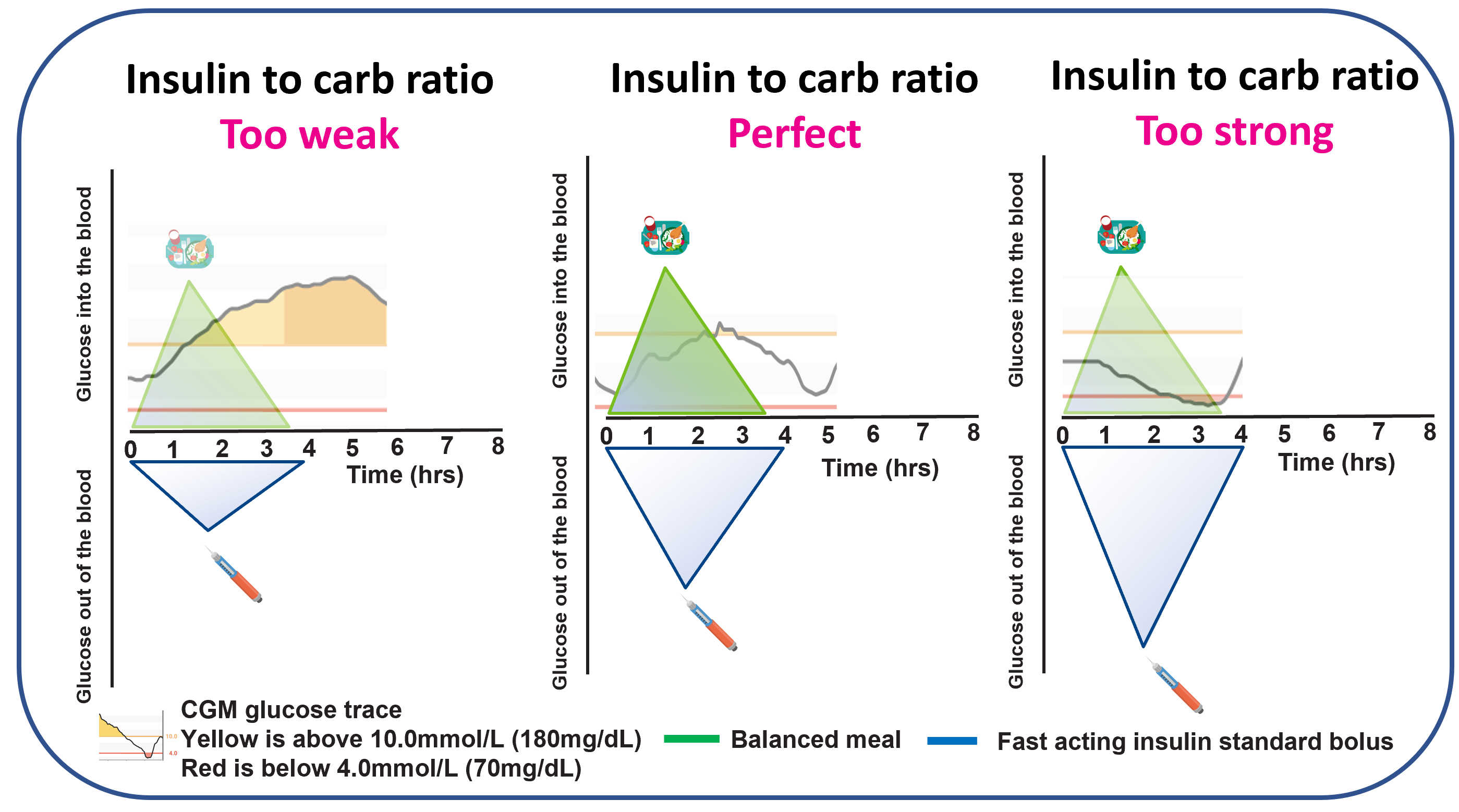
Why does the glucose level go higher after eating even if the carb ratio is perfect?
Dani, I am sure you spotted that the glucose level still goes higher after eating when the carb ratio is perfect in the picture above.
Want to know why?
Time to put on the propeller hat and get nerdy!
Let’s start slow. Speaking of slow. In comparison to glucose from a meal, insulin is very slow. It’s a tortoise-and-hare situation.


The simple solution is to make sure the insulin is delivered twenty minutes before eating. This has proven to be successful time and again.
The picture below is from a famous study showing that fast-acting insulin given twenty minutes before a meal keeps the glucose spike under control.

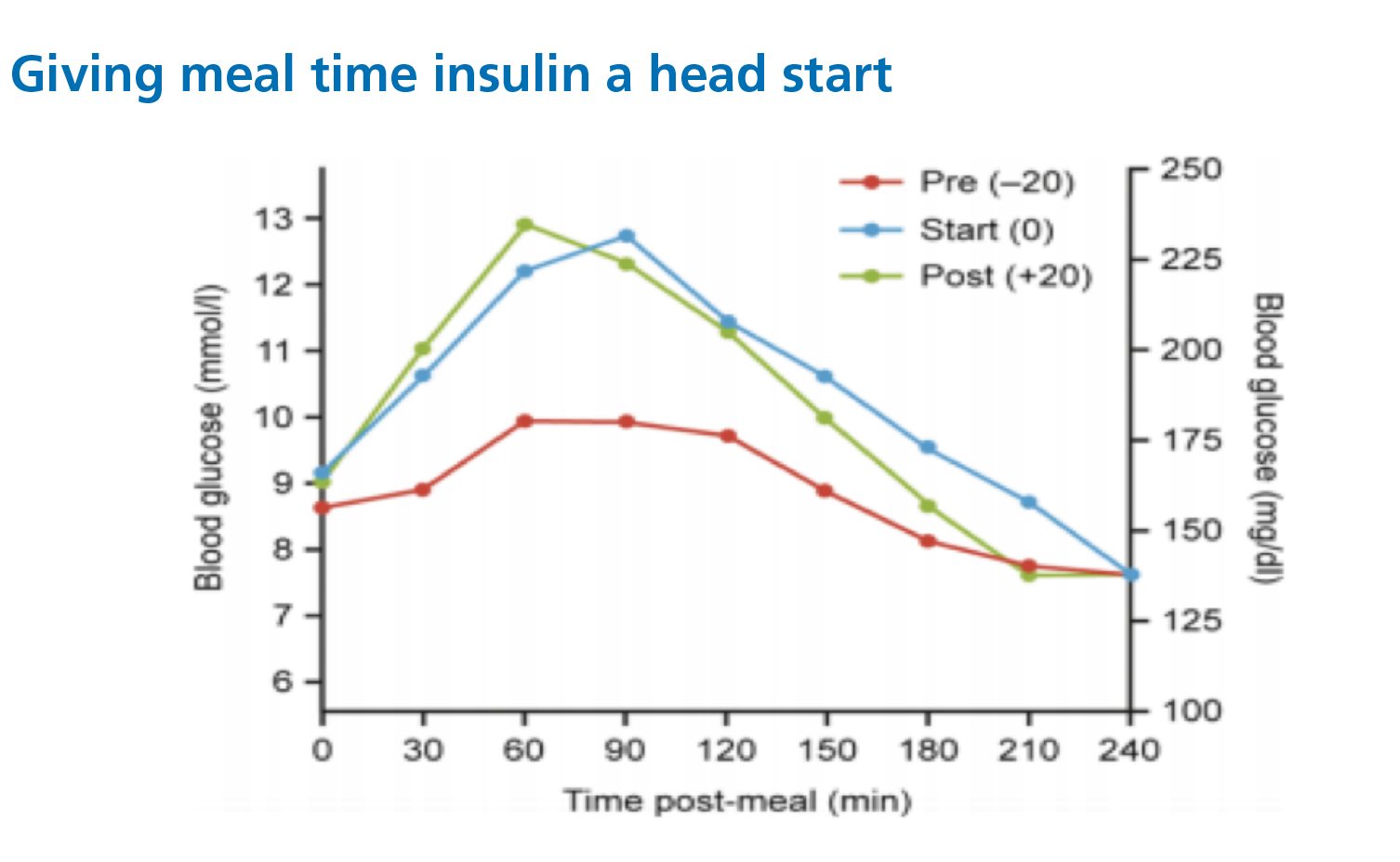
This is great, but even with insulin twenty minutes before a meal, there is still a little spike. What’s going on?
It took me ages to do these next two graphics. So please, take some time to appreciate them.
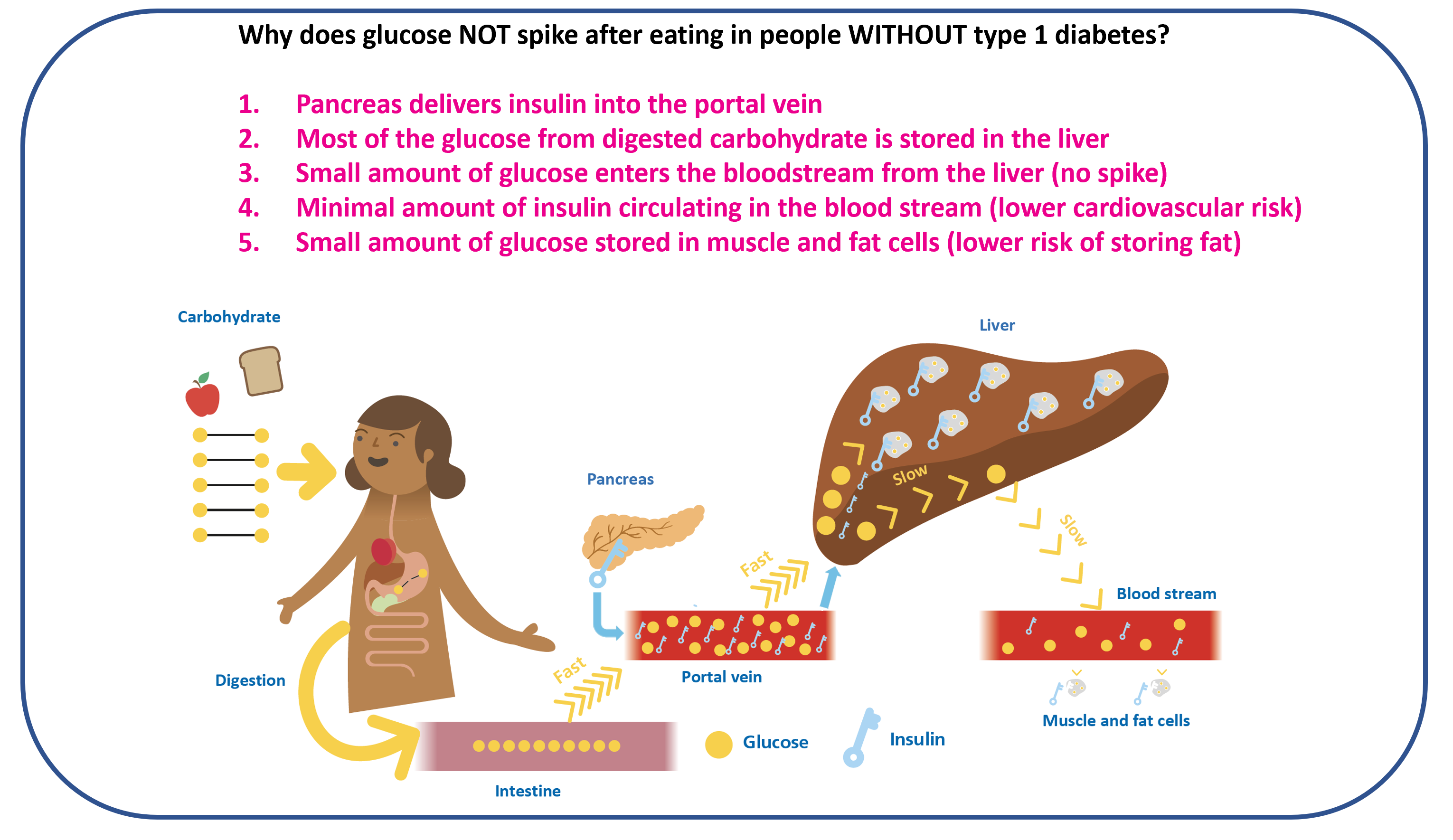
The first cartoon shows why people without type 1 diabetes don’t get a spike – hint, it’s all about plenty of insulin in the portal vein.

This one shows why people with type 1 diabetes get a spike – hint, it’s all about lack of insulin in the portal vein.

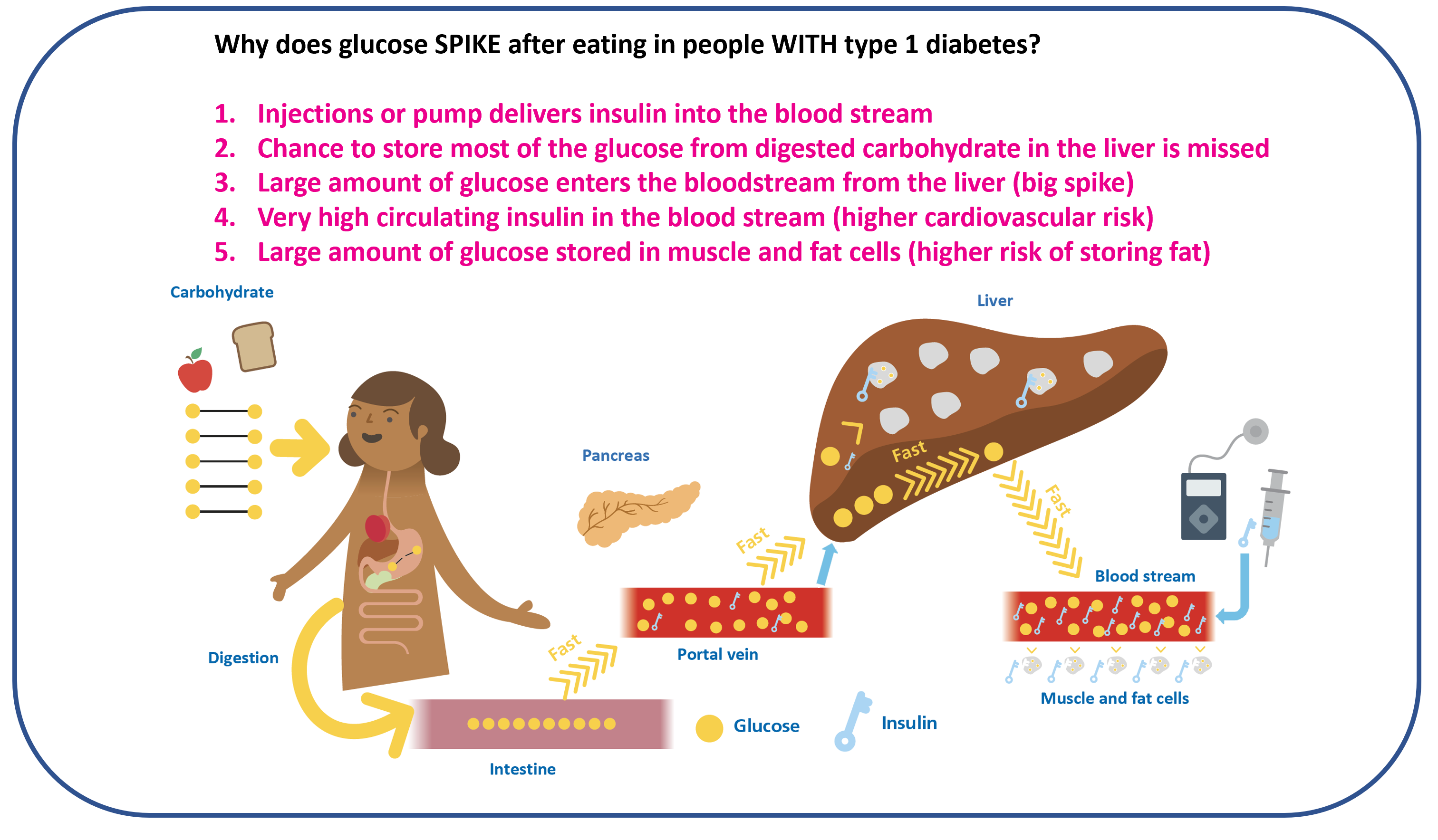
You now understand the issue is a lack of insulin in the portal vein and too much in the blood stream, but there is something else.
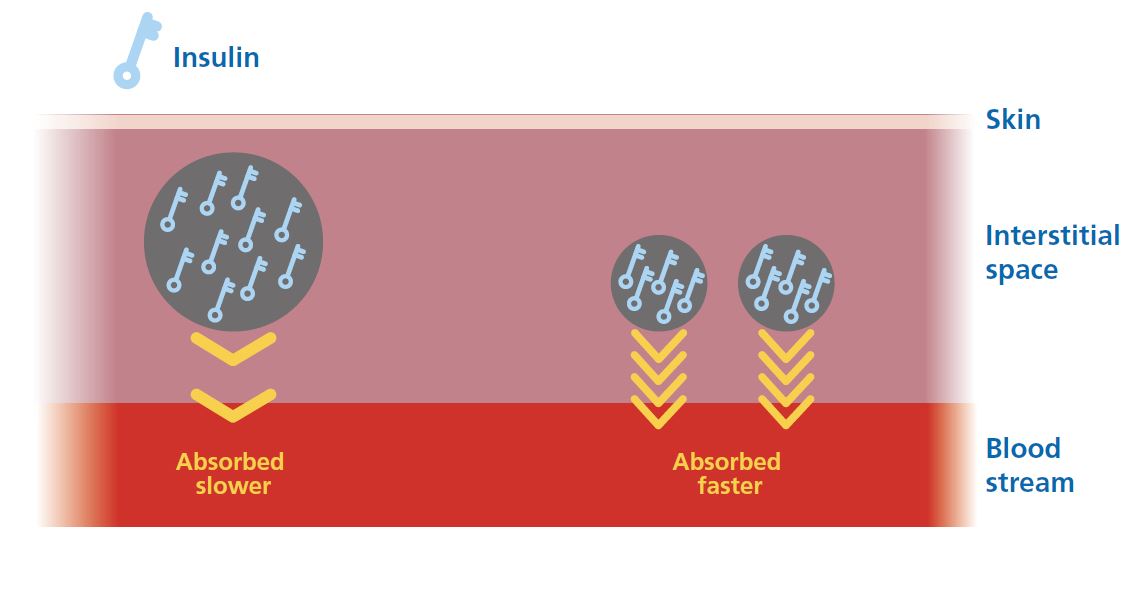
This picture explains why insulin absorption from an injection or pump is much slower than from the pancreas.

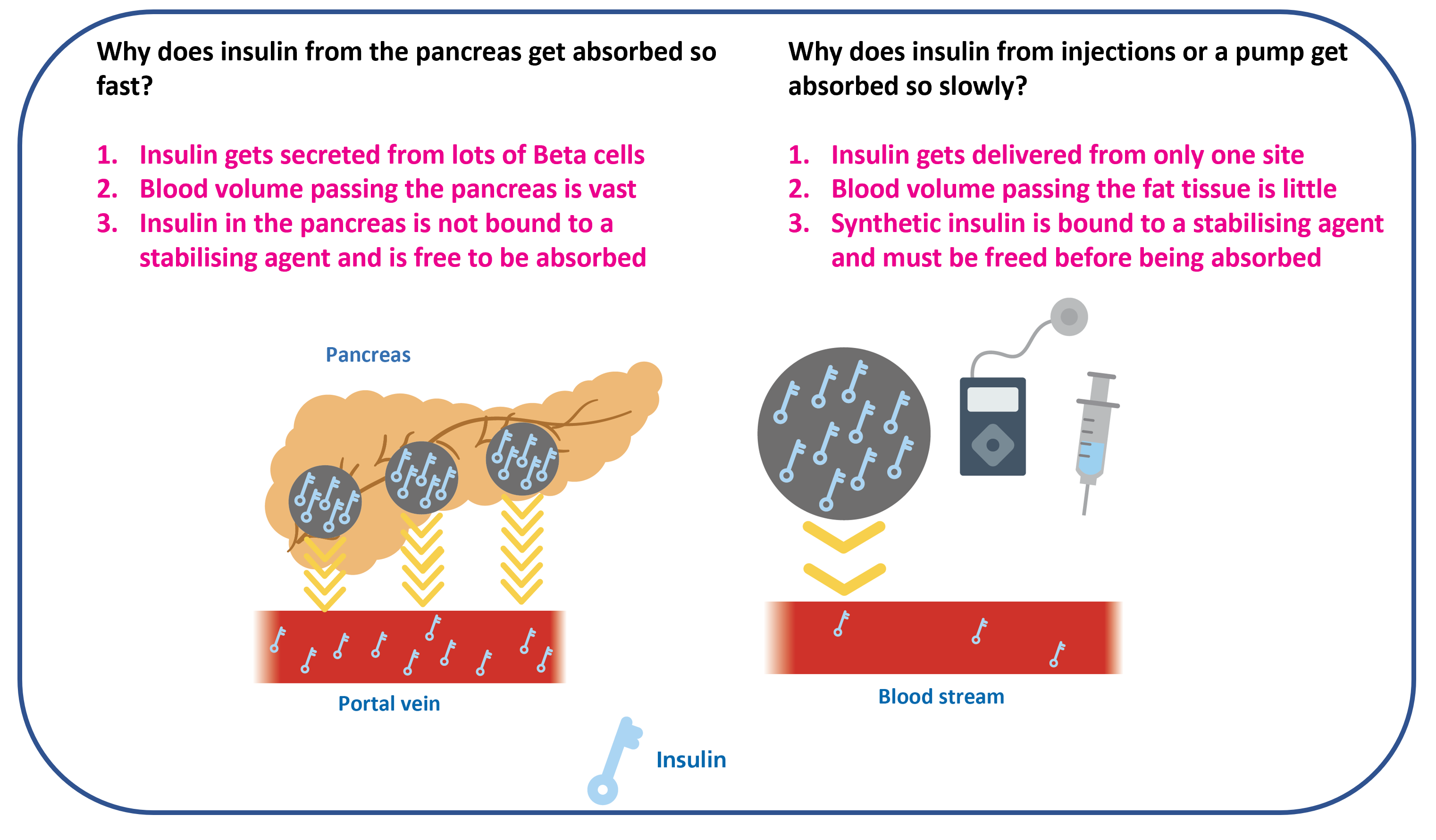
This double whammy of slow absorption and lack of insulin in the portal vein makes it challenging to stop glucose spikes after eating.
It can be done.
How?
Using SET of Dynamic Glucose Management. Here is teaser: you can change the pre-meal insulin timing depending on glucose level and arrow, but you will have to wait until you finish the foundations.
The Mealtime Insulin Guide is also packed with after-meal glucose spike-busting tactics.
Stay here for now.
More tricks can help stop the after-meal glucose spike.
Does giving fast-acting insulin help stop after-meal glucose spikes?
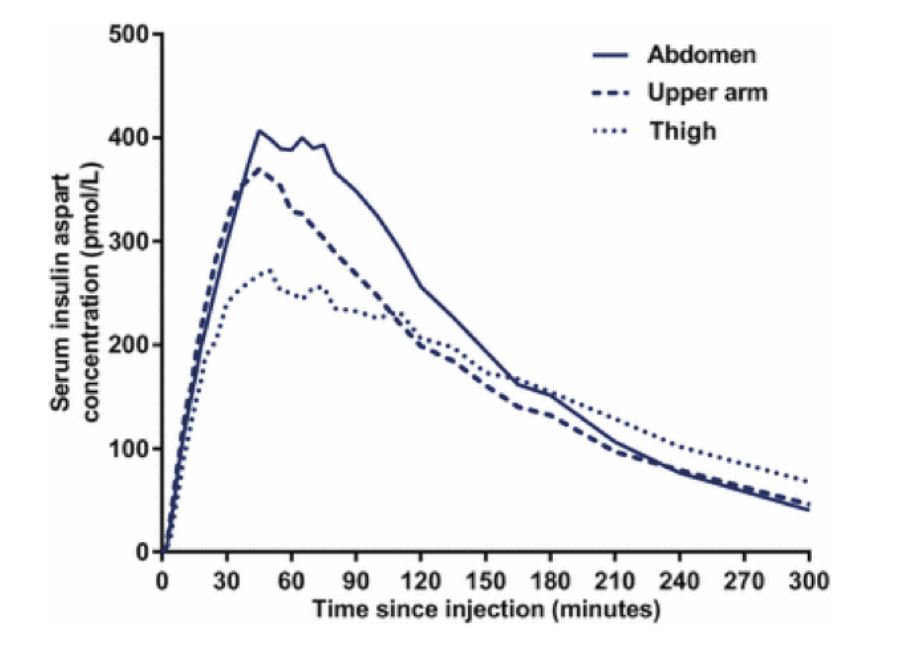
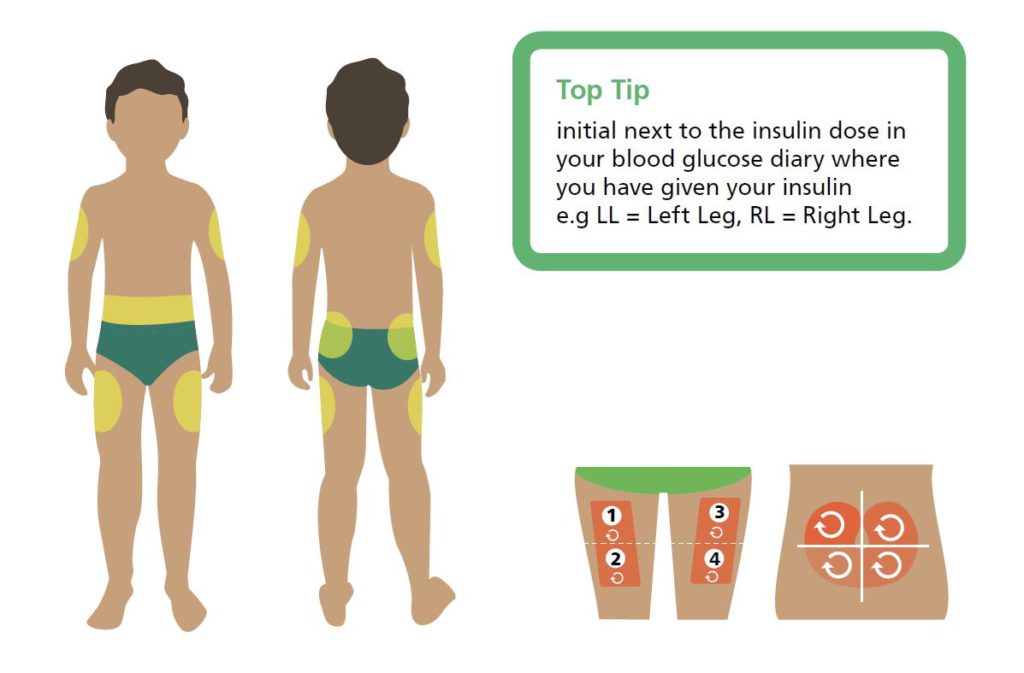
It certainly does. This graph shows that fast-acting insulin works the fastest in the abdomen (belly), second fastest in the upper arm, and at snail’s pace in the outer thigh.

Top tips:
- If using a pump, only use the abdomen and upper arm for cannula sites. If you regularly swap from thigh to abdomen, expect a rollercoaster ride!
- If using injections, inject basal insulin into the thigh or buttocks and fast-acting insulin into the abdomen or upper arm.
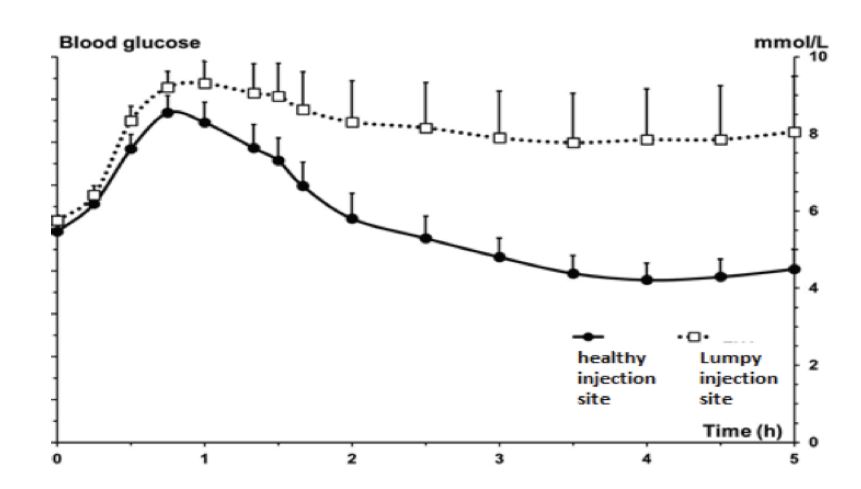
Whilst on injection sites, this picture shows how important it is to avoid lumpy areas. Insulin is poorly absorbed from damaged tissue, and the glucose will be high.

To prevent lumpy areas, you will be wise to rotate injection/cannula sites. Here is an easy rotation system to follow.

Do large doses of fast-acting insulin take longer to absorb?
You already know the answer is yes from the previous discussion where I showed lots of Beta cells delivering insulin is faster than one big site.
The same principle applies here. Halving a large dose is faster. This picture tells the story.

Obviously you do not want to split every dose! Keep it simple, split any dose above 10-15units:
- Injections: Split into two equal amounts. For example, a 20-unit bolus could be given as two injections of 10 units at least 2cm apart.
- Pump: Do a split bolus with 50% upfront and 50% over the next 15-30 minutes.
It’s probably worth reviewing this part a few times. It’s essential for Dynamic Glucose Management and the Mealtime Insulin Guide.
What’s next? Correction Insulin

This has been really useful and made me understand a lot of details, thank you so much!