
This is the AID hub where all the resources can easily be accessed.
This page also explains what AID systems are, how they work, what improvement to expect, and how to choose between systems. We reccomend you read this page first, but, If you want to jump straight to a specific system, exercise guidance, or optimisation tips, use the hub links below.
Jump to a system:
- Choosing an AID System: Which Superhero?
- Tandem t:slim X2 with Control-IQ → Spider-Man
- Medtronic 780G → The Incredible Hulk
- CamAPS FX → Batman (see also: CamAPS FX FAQ)
- Omnipod 5 → Iron Man
Other useful AID resources:
- Top 10 tips to optimise time in range
- AID + exercise (key guide)
- Looping blind: DIY perspective
- GNL AID Study Day
Skin in the game
Adhering to the principle of skin in the game, I spent from 2017 to 2026 gaining personal and professional experience before writing this guide.
I have personally tried Medtronic 670G/780G, Tandem t:slim X2 with Control-IQ, Omnipod 5, DIY Loop, and Android APS. In clinical practice, I have helped more than 300 children and young people start on every commercially available AID system.
Short version: they are all game-changers.
Choosing between them is like choosing a supercar: there is no single “best system”, only the right one for you.

What this guide will help you do
- Understand what AID systems are and how they work.
- Apply simple decision criteria when choosing a system.
- Use practical tips to get the most from whichever system you choose.
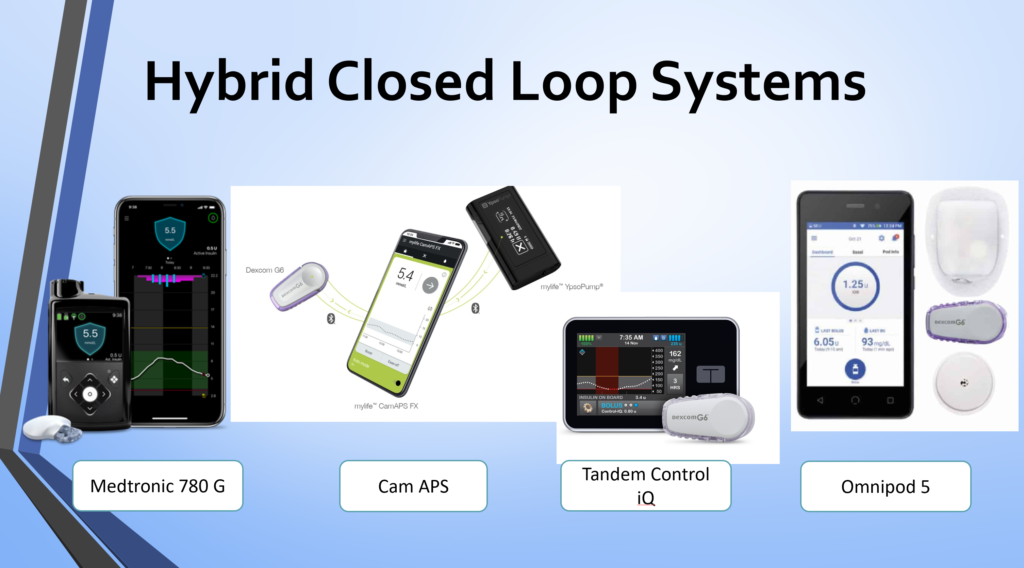
What are AID systems and how do they work?
AID systems combine three components:
- An insulin pump.
- An algorithm (in the pump or a smartphone app) that adjusts insulin to reduce highs and lows.
Current commercially available systems in the UK (January 2026):
How AID systems operate (in plain English)
- When glucose is predicted to rise above target, the algorithm increases insulin (extra basal and/or an auto-correction bolus).
- When glucose is predicted to fall, it reduces or suspends insulin delivery.
- You still need to enter carbohydrates eaten and bolus for meals. AID cannot yet replace meal boluses.
Foundations still apply. AID is not a replacement for the basics; it is a powerful layer on top:
- Accurate carb counting
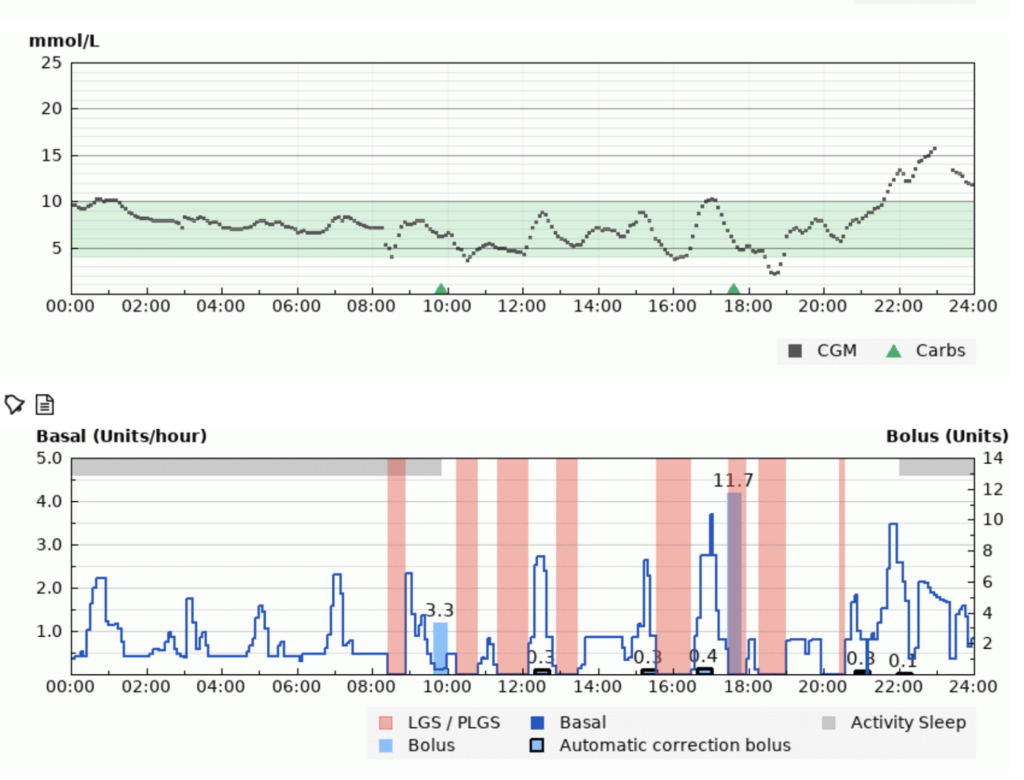
How does the algorithm increase insulin?
Overnight, the system typically increases basal insulin when glucose rises above target. Later in the day, many systems will also deliver automatic corrections (for example, a small correction dose when glucose is predicted to remain high).
How does the algorithm decrease insulin?
To prevent lows, basal insulin is reduced and may be suspended entirely when glucose is predicted to fall. Meal boluses still show as separate doses — the system is supporting your decisions, not replacing them.
Expected improvement with AID systems
- CGM alone: often ~40–60% time in range (TIR 3.9–10.0 mmol/L / 70–180 mg/dL).
- AID systems: commonly ~60–90% TIR.
- Typical gain: +10–30% versus baseline (larger gains when starting from a lower TIR).
This improvement is usually achieved with less micromanagement, not more.
Without AID, pushing beyond ~70% TIR often requires:
- Checking CGM repeatedly across the day.
- Multiple correction boluses.
- Frequent hypo treatments.
- Ongoing trial-and-error learning.
AID systems let you get more by doing less.
The hidden superpower: sleep
You get your eight hours back.
Fewer overnight hypos. Fewer wake-ups high. Flatter lines overnight — for you, and for parents of children with Type 1 diabetes.
Choosing your system
All AID systems improve glucose control and quality of life. If you cannot access a specific system, do not stress. They all deliver meaningful benefit.
The question is not “Which is best?” The question is: Which is best for you?
Important: AID is powerful, but it still depends on CGM performance, insulin timing, meal boluses, and the basics. If you’re struggling with exercise on AID, start here: AID + exercise (key guide).
Ready to explore the systems?
- CamAPS FX → Batman (see also: CamAPS FX FAQ)
AID resources (hub)
Use these pages to go deeper, troubleshoot, or optimise: