Mastering Type 1 Diabetes
Dynamic Glucose Management
A practical framework for high time in range, built on fast movers between meals, not slow insulin corrections.
Overview
Dynamic Glucose Management is a practical framework for achieving high time in range by using fast movers between meals, especially short bursts of activity, instead of relying on insulin corrections alone.
The Foundations section teaches safety. This is where you learn to get skilled.
Want to jump straight to the tools? These pages work best as a system, used in order.
Prerequisites: only continue if you have completed and genuinely understood the Foundations section. You also need to be using a CGM with alarms. CGM is both the teacher and the safety net here.
Video: Dynamic Glucose Management explained
The video below is the recommended starting point for understanding how the framework fits together.
Where this came from
Dynamic Glucose Management has been in development since diagnosis in 2008, years of trial and error, repeated failures, and constant tinkering, with nose in the research trying to understand why glucose behaves in such stubborn, mysterious ways.
The aim is to cut the learning curve to six months or less.
The framework rests on three pillars:

Trial and error with plenty of tinkering is needed to make the system personal. The framework provides the principles; CGM data provides the feedback.
Christmas Day 2018: the slow-lane disaster
The insight that made the model unavoidable arrived on Christmas Day 2018.
The day started simply enough: no breakfast, a bacon sandwich for lunch, then a planned Christmas dinner. The high alert was set at 11.0 mmol/L (200 mg/dL). The plan was to correct highs with insulin and prevent lows with Coca-Cola.
Carbohydrates were weighed and counted precisely. Insulin was delivered 20 minutes before eating. Every extra gram was accounted for. Then, an hour after starting Christmas dinner, glucose climbed steeply. It took five separate correction doses over five hours to return to range.
The meal dose was 10 units (around 200 g carbohydrates). Corrections added another 15 units, a total of 25 units, 150% more than expected for the meal alone.
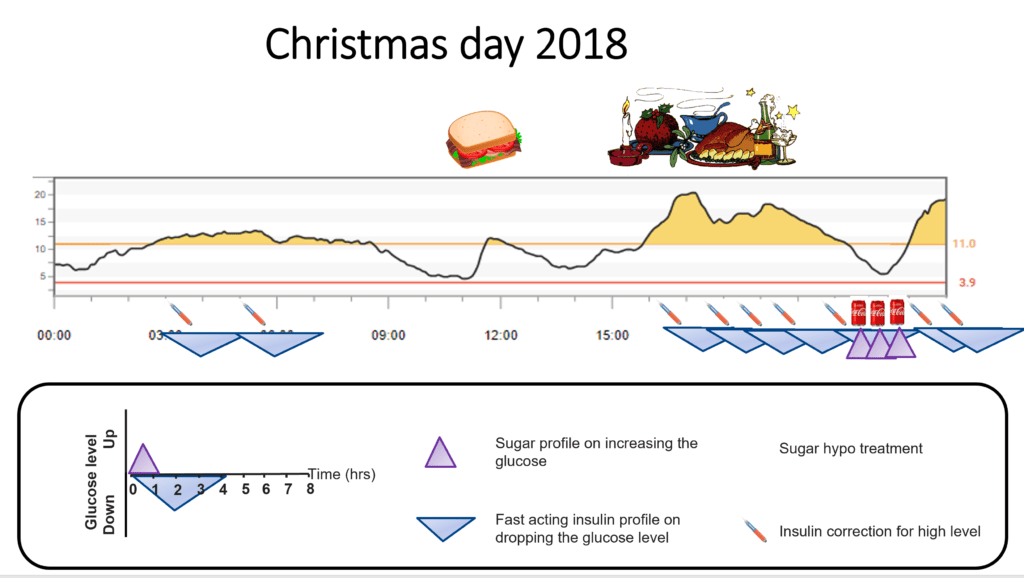
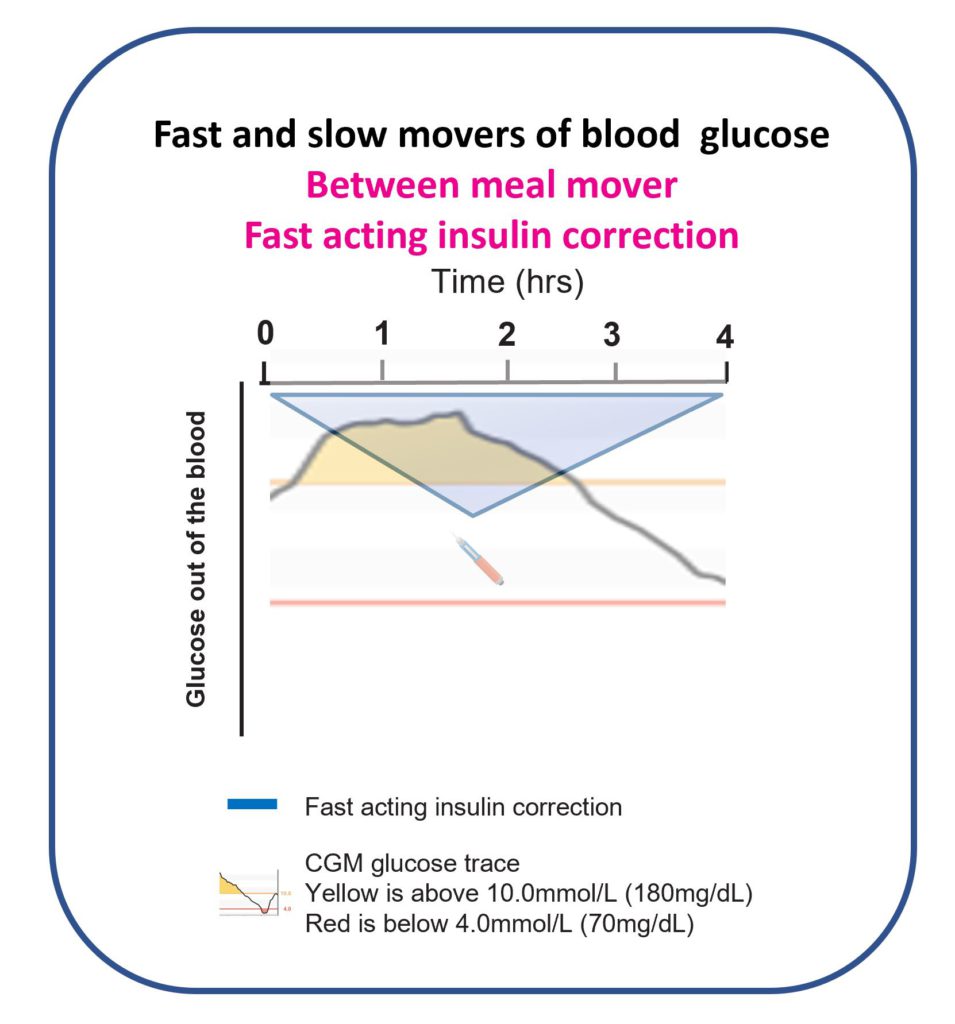
The extra insulin was not the main problem. The problem was speed. Fast-acting insulin peaks around 90 minutes after injection and keeps lowering glucose for roughly four hours. With correction after correction stacking up, glucose eventually nosedived.
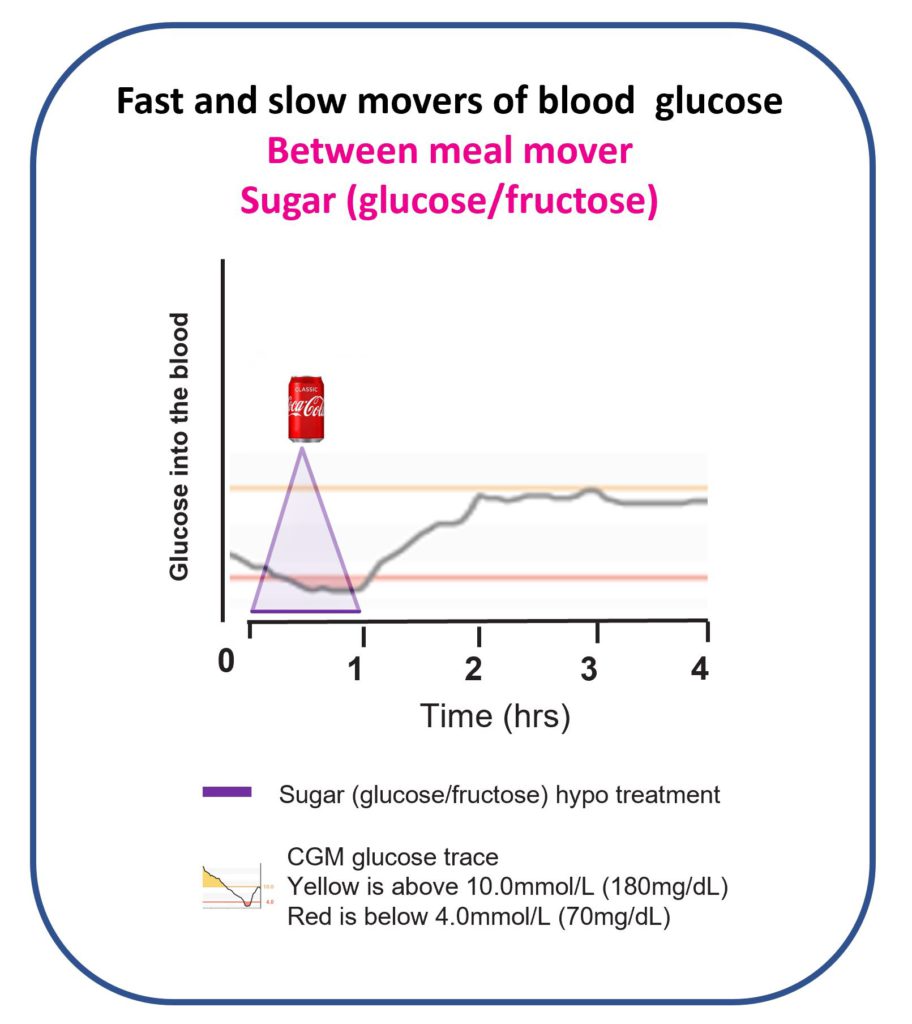
Three 200 ml portions of Coca-Cola were used to try to stop the drop. Each was slow to act. Glucose eventually levelled out, then climbed again. By the end of the day, after ten years of living with type 1 diabetes and working as a diabetes dietitian, glucose management had been thoroughly outwitted.
The shift: stop living in the slow lane
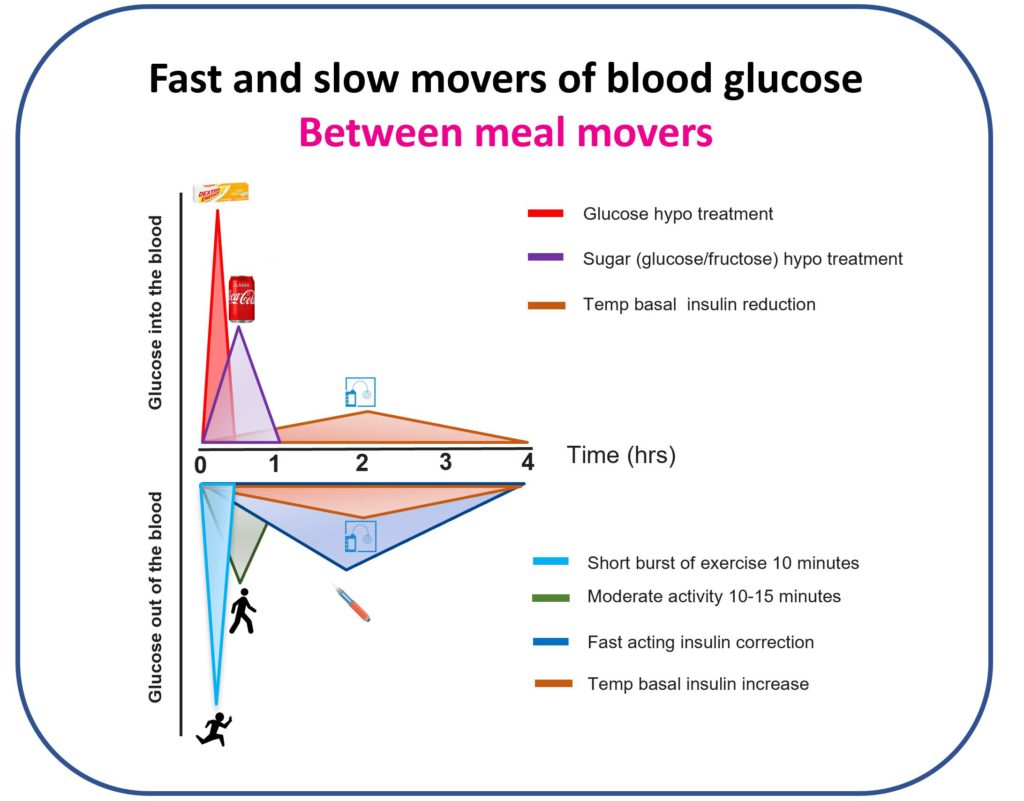
The lesson from 2018 was clear. Between meals, some tactics move glucose very fast and some are painfully slow. The default approach, correcting highs with insulin and treating lows with sugary drinks, relied entirely on slow movers.
The question was: what are the fast movers?
Christmas Day 2019: the fast-lane win
The same food plan as 2018, no breakfast, bacon sandwich for lunch, Christmas dinner feast, but this time with a commitment to fast movers throughout.
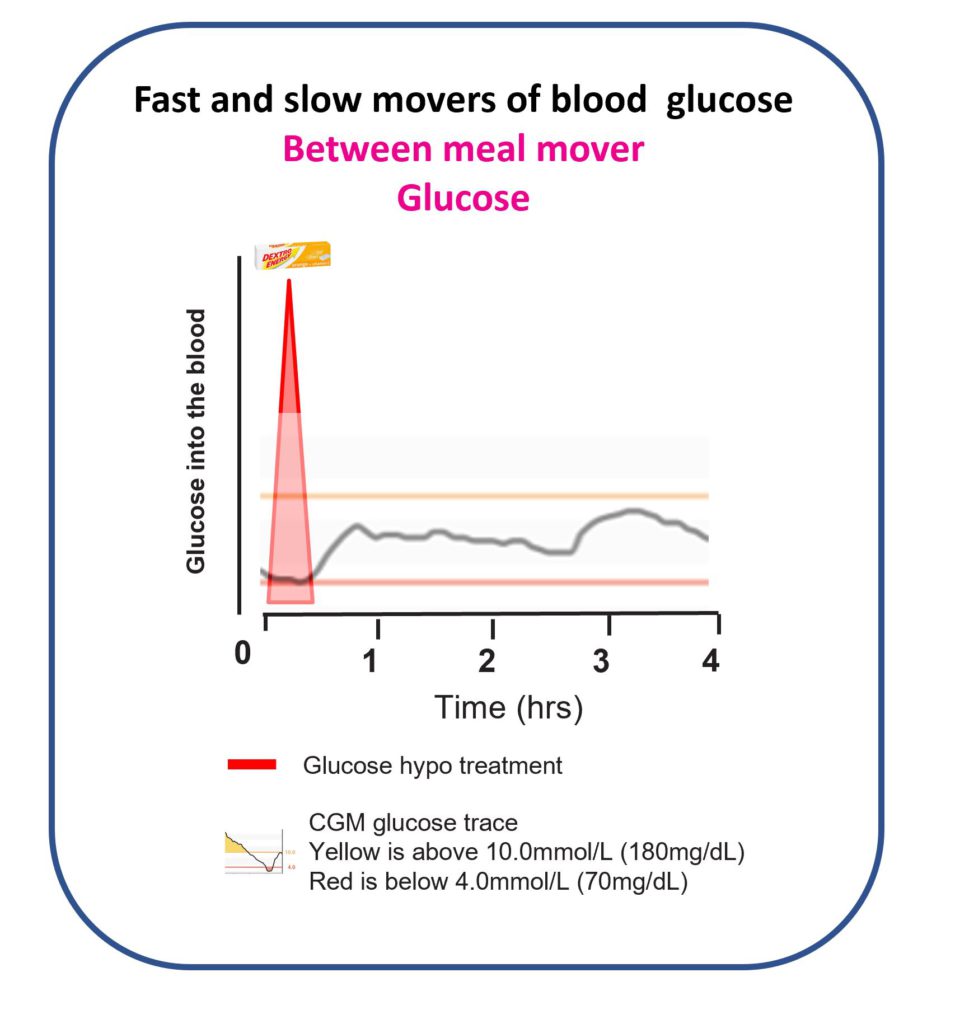
The high alert stayed at 11.0 mmol/L (200 mg/dL), but instead of correcting highs with insulin, short bursts of exercise were used. Coca-Cola was replaced with dextrose tablets.
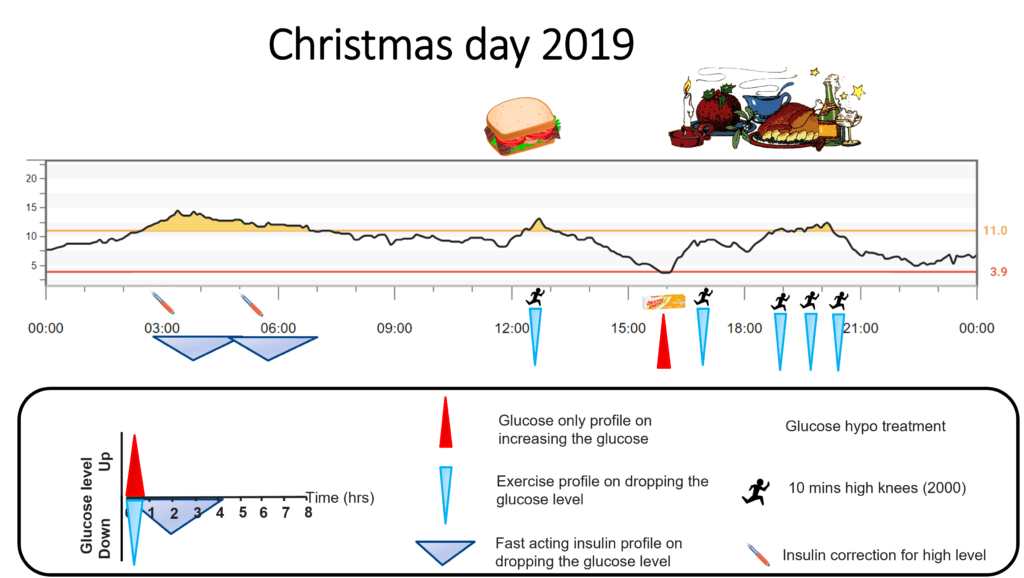
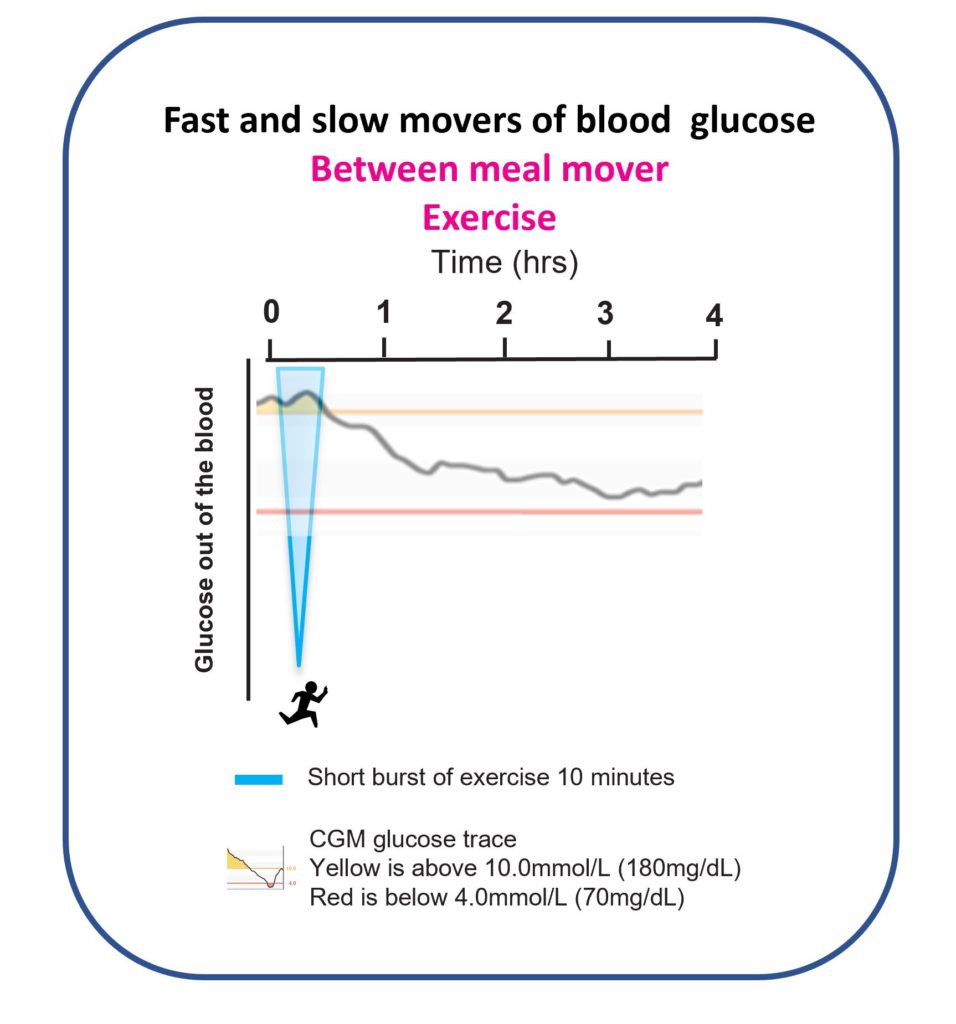
When glucose nudged up after lunch, 10 minutes of high knees brought it back into range almost immediately, exactly as the Activity and movement page explains it should.
Before dinner, glucose drifted low. Rather than a full treatment, half a treatment was used, three dextrose tablets instead of six, resulting in a controlled rise back to mid-range without overshoot.
Christmas dinner itself required the same 10 units as in 2018 (around 200 g carbohydrates). As glucose started climbing, a 10-minute burst of high knees stopped the rise before the alarm even triggered. Pudding, cheese, and crackers triggered the alarm later; three more bursts of exercise over 90 minutes, totalling around 10,000 high knees across the day, kept glucose in range through to bedtime.
Result: in range by bedtime. No insulin stacking. No glucose stacking. Safe overnight sleep.
This was an extreme demonstration. No one uses this level of activity every day to manage diabetes. But no one eats Christmas dinner every day either. The demonstration showed clearly how fast movers change what is possible.
GAME-SET-MATCH: the three pillars
That day, the three pillars of Dynamic Glucose Management became clear.
Stop highs, GAME
- G: Glucose time in range desired
- A: Alert on high set according to the desired time in range
- M: Mode of exercise that can be done anywhere
- E: Exercise on high alert, based on glucose value and trend arrow
Stay in target, SET
- S: Start insulin before eating
- E: Eat three balanced meals
- T: Ten minutes of activity after eating
Prevent lows, MATCH
- M: Measure weight to calculate hypo treatment dose
- A: Always use glucose only, not sugar
- T: Try to prevent lows before they happen
- C: Change treatment based on glucose value and arrow
- H: Have patience and wait 20 minutes
How Dynamic Glucose Management compares with AID systems
What follows describes what AID systems did and did not do in one individual’s diabetes. It is not a general claim about AID system capabilities across all users.
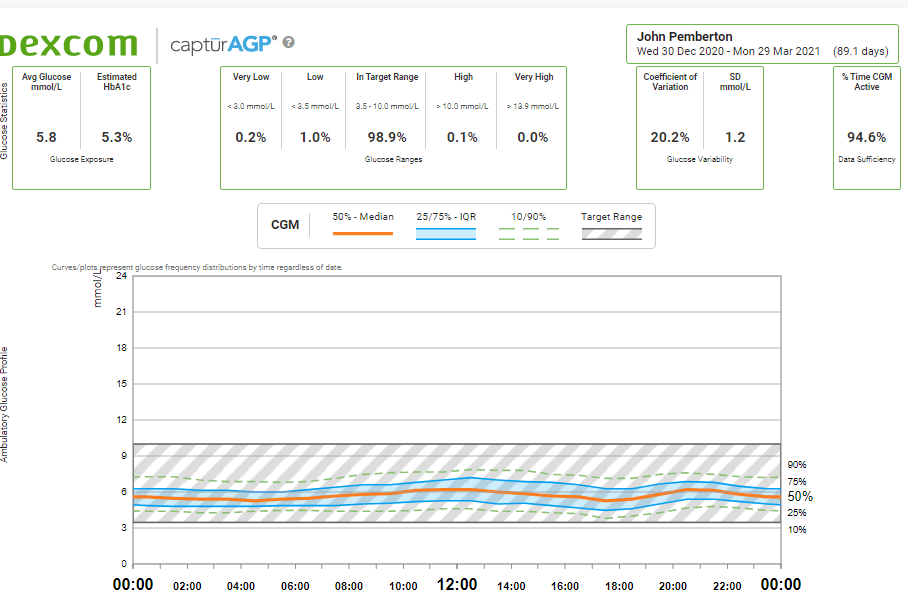
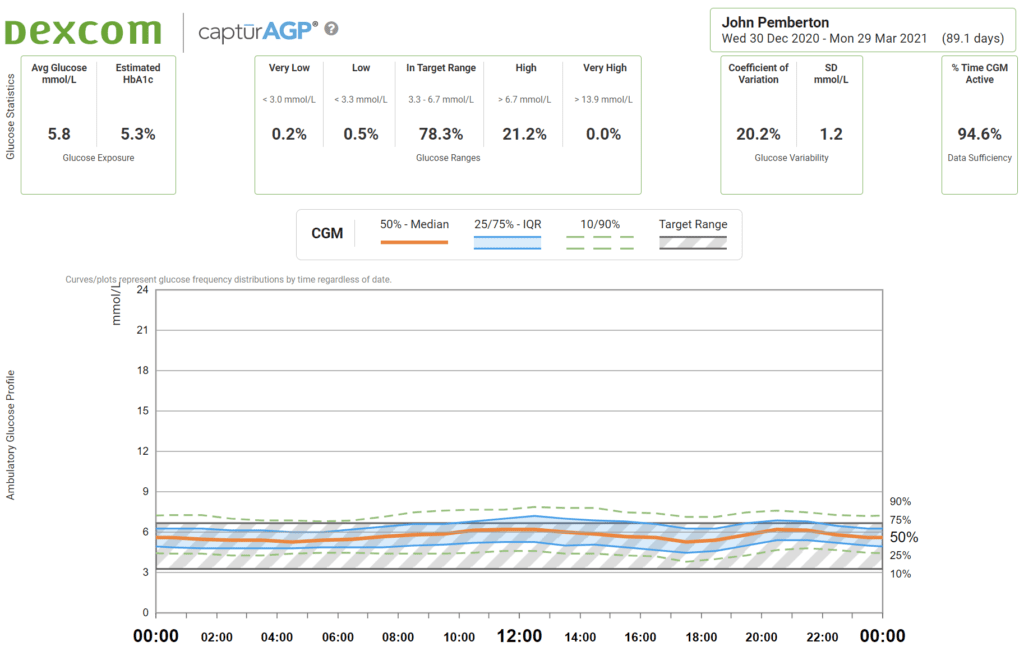
In personal experience, DIY looping, Control-IQ, and the 670G all typically delivered around 85% time in range with roughly 3% time below target. That is solid control. Dynamic Glucose Management during waking hours pushed this to around 99% time in range and roughly 1% time below target in the same individual’s data.
AID systems are excellent overnight, when liver glucose output is the main variable and insulin alone can manage it well. During the day, food, activity, stress, and unpredictability enter the picture. Using only insulin, a slow mover, cannot keep up with those variables as quickly as fast movers can.
In personal data, AID systems typically managed around 50% time in the optimal non-diabetic range (3.3 to 6.7 mmol/L or 60 to 120 mg/dL). Dynamic Glucose Management pushed this to around 80% during the day.
The optimal combination, based on personal experience, is an AID system overnight for safe sleep combined with Dynamic Glucose Management during waking hours.
Dynamic Glucose Management takes time, attention, and a degree of persistence. Some people will find that engaging. Others will not. Both responses are entirely reasonable, it is an individual choice based on individual circumstances.
The only approach that has been found to match this level of control is severe carbohydrate restriction. This has also been explored in detail in the 120-day carbohydrate experiment.
There is no need to severely restrict carbohydrates to achieve near-perfect glucose control, provided fast movers are used between meals.
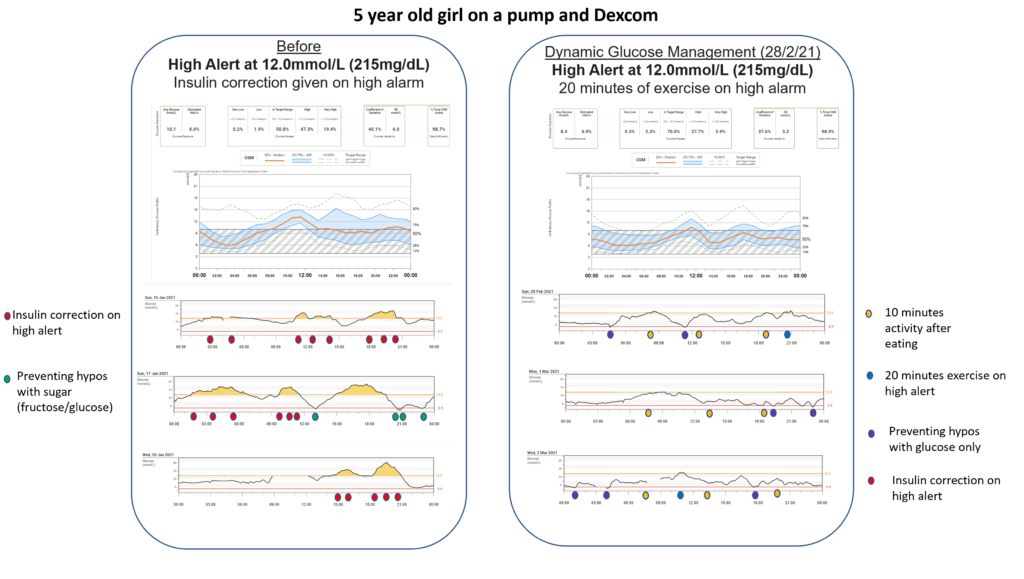
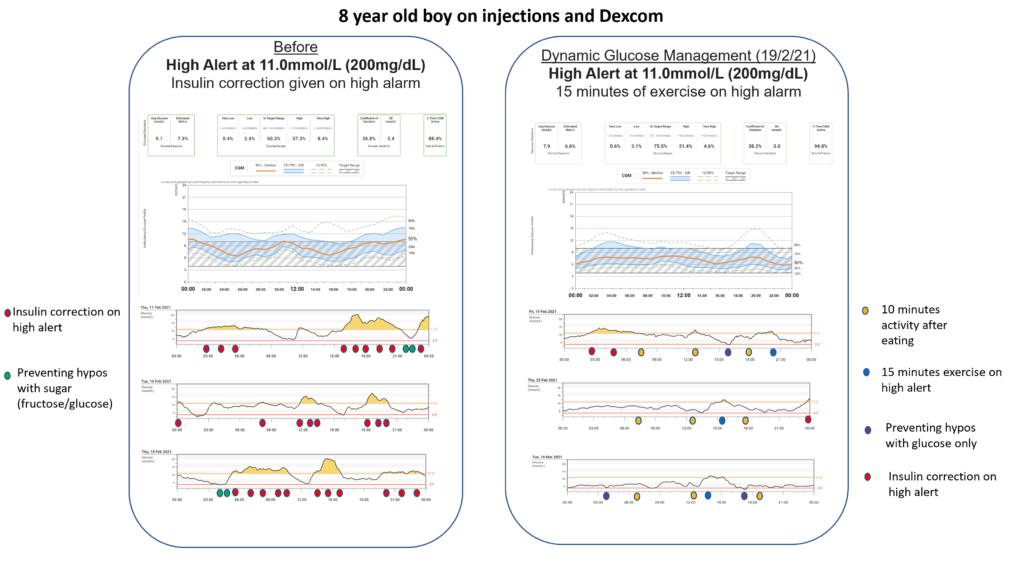
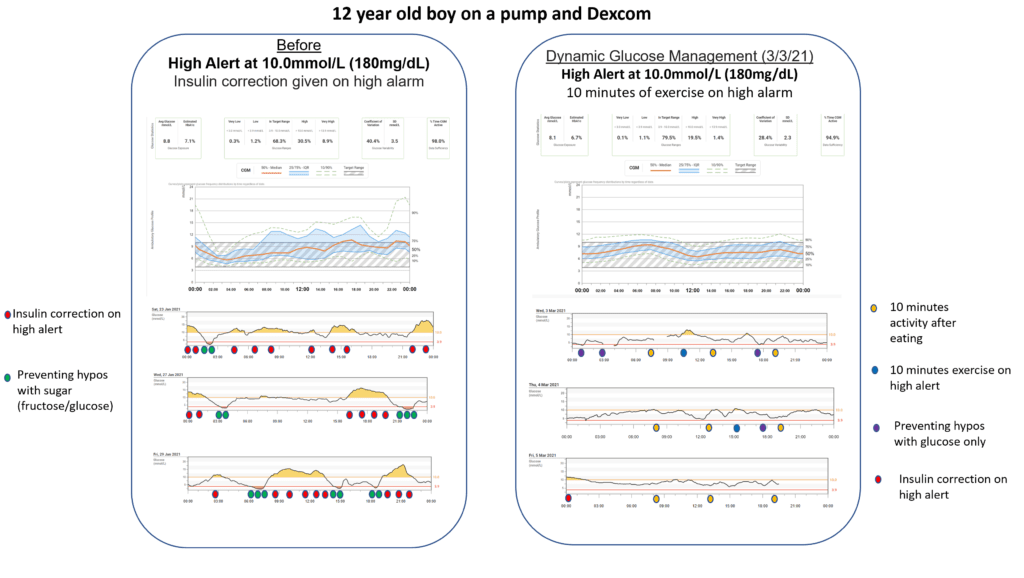
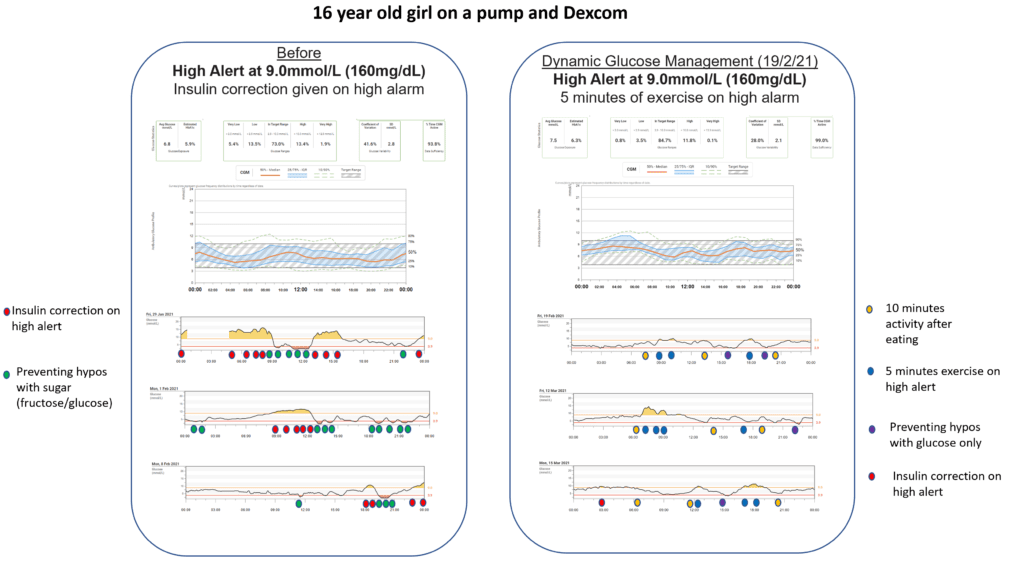
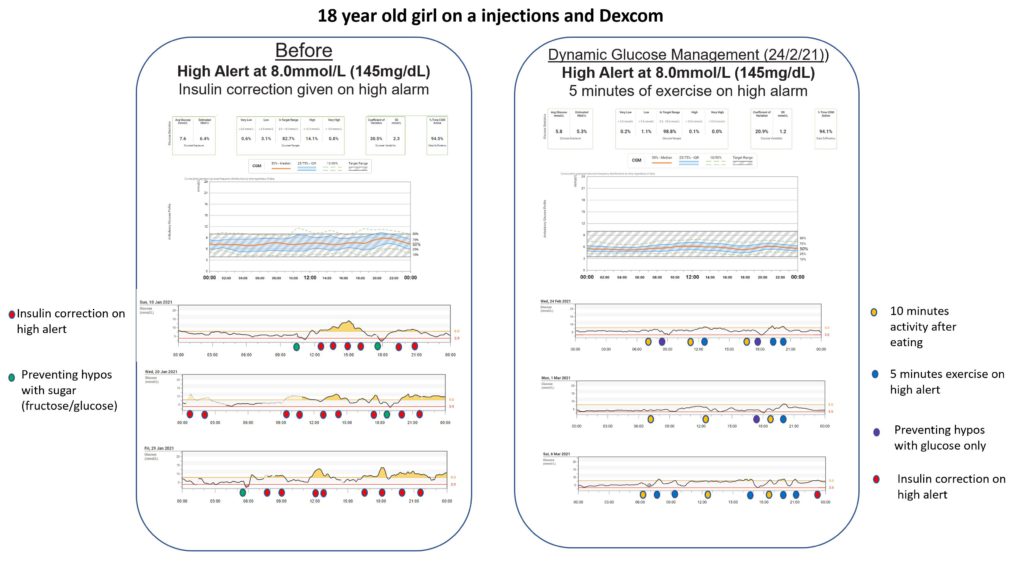
What the evidence shows in children and young people
A CGM structured-education programme teaching Dynamic Glucose Management to children, young people, and their families was introduced at Birmingham Children’s Hospital. The first fifty participants educated were published in the research record (available in the Research section).
The programme stopped problematic hypoglycaemia and increased time in range by around 10% on average. Those who used the framework most consistently reached the highest time in range, roughly 70 to 90%.
In an audit of the first hundred participants educated, the strongest drivers of improved time in range were: short bursts of activity to correct highs between meals, adjusting pre-meal insulin timing based on glucose value and trend arrow, and using glucose-only treatments (not sugar) for lows.
What to explore in your own CGM data
- What does your glucose trace look like in the two hours after a large meal? Does using short bursts of activity during that window change the pattern?
- How does the size and timing of your pre-meal bolus affect the post-meal glucose curve?
- What is the difference in your overnight trace on nights following high versus moderate activity during the day?
Dynamic Glucose Management is a framework. Your CGM data is the feedback that shows how it works, or needs adapting, for you specifically.
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Start here
Work through the pillars in order. Don’t jump ahead.