

It’s finally landed!
The Automated Insulin Delivery (AID) and Exercise Consensus Statement
Download all the best graphics for mmol/L here and mg/dL here
As a member of the writing group for the European Association for the Study of Diabetes (EASD) and the International Society for Pediatric and Adolescent Diabetes (ISPAD) position statement, I am honoured to contribute to this essential guidance. This document consolidates the latest evidence and clinical practices to provide comprehensive and actionable recommendations for exercising safely with type 1 diabetes using AID systems. By leveraging these insights, individuals, families, and healthcare providers can better navigate the complexities of managing physical activity, ensuring both safety and enjoyment. The practical tools offered in this position statement make it accessible and easy to incorporate into daily life, irrespective of experience with AID systems.
Here are the people to thank, with the biggest love being sent to Othmar and Dessi who drove the Consensus. I am sure it nearly drove them mad!

A little background
Exercise plays a vital role in managing type 1 diabetes, improving overall health and quality of life. Yet, for individuals using AID systems, physical activity can bring unique challenges, particularly around glucose fluctuations. This article highlights the key messages for safely managing exercise with AID systems, along with practical strategies to make implementation straightforward.
If you are new to exercise and T1D – here is a guide to get you started
Core Principles for Safe Exercise with AID Systems
The consensus outlines key strategies that address various aspects of physical activity and glucose management:
1. Planned Physical Activity: Setting a higher glucose target 1–2 hours before exercise is essential when a drop in glucose levels is anticipated. Conversely, for activities likely to raise glucose levels, maintaining regular or lower glucose targets is more appropriate. If exercise occurs within 2 hours of a meal, reduce the amount of carbohydrates entered into the AID system by 25–33%. This adjustment lowers the risk of hypoglycemia, even if glucose levels temporarily exceed the target range. The 25–33% carbohydrate reduction results in a net insulin decrease, as the system will not deliver more insulin than has been omitted for elevated glucose levels during exercise. This strategy only applies when exercising within 2 hours of eating.
2. Unplanned Physical Activity: For sudden activity, adjustments can be made on the spot by increasing glucose targets and consuming small amounts of fast-acting carbohydrates if glucose levels fall below 7.0 mmol/L (126 mg/dL)
3. Carbohydrate Management: Balancing carbohydrate intake around exercise prevents hypoglycemia while minimising post-activity hyperglycemia. Tailoring the type and timing of carbohydrates is essential. Start supplementing with carbs below 7.0 mmol/L (126 mg/dL) with 3-20g every 20-30 minutes. The amount required depends on the trend arrows before and expected glucose behavior during activity. This graphic (my favorite of this kind) from the paper will help you think about what will happen during the exercise.


4. Timing and Insulin on Board (IOB): Engaging in activity with minimal insulin on board reduces hypoglycaemia risk (Three-hour rule: last meal, and bolus insulin at least three hours before starting). Planning exercise before meals or during fasting periods is often safer.
5. Device Adaptations: Most AID systems allow temporary adjustments, such as higher glucose targets or activity-specific settings, which can be used to reduce hypoglycaemia risk during exercise.
These strategies underscore the importance of understanding individual glucose responses and using available AID features effectively.
System-Specific Considerations
The position statement provides tailored guidance for managing exercise across different AID systems, including Othmar’s wife amazing infographics:
• Beta Bionics iLet: Limited in its ability to adjust glucose targets before exercise, requiring manual carbohydrate management for safety.


• CamDiab mylife CamAPS FX: Features “Ease-off” mode to safely elevate glucose levels, relax the aggressiveness of the algorithm, and therefore mitigate hypoglycemia risk during activities. Alongside increasing the personal glucose target, if required.


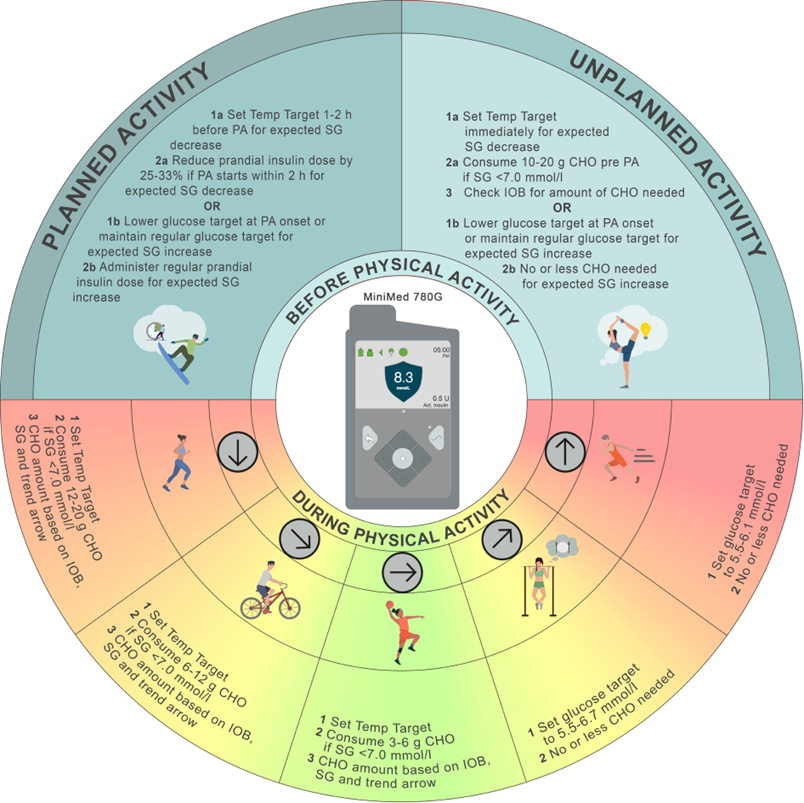
• Medtronic MiniMed 780G: Utilises a “Temp Target” setting that prevents automated bolus corrections during exercise, making it particularly effective for hypoglycaemia prevention.
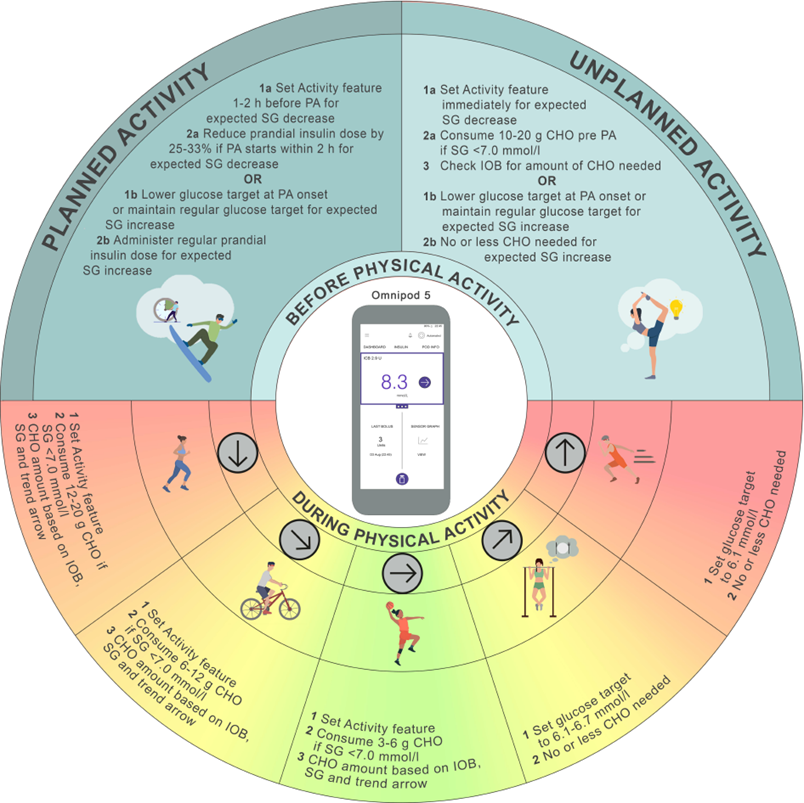
• Omnipod 5: Provides an “Activity” feature for setting a higher glucose target 1–2 hours before exercise to stabilise levels, and reduce the aggressiveness of the Smart Adjust.
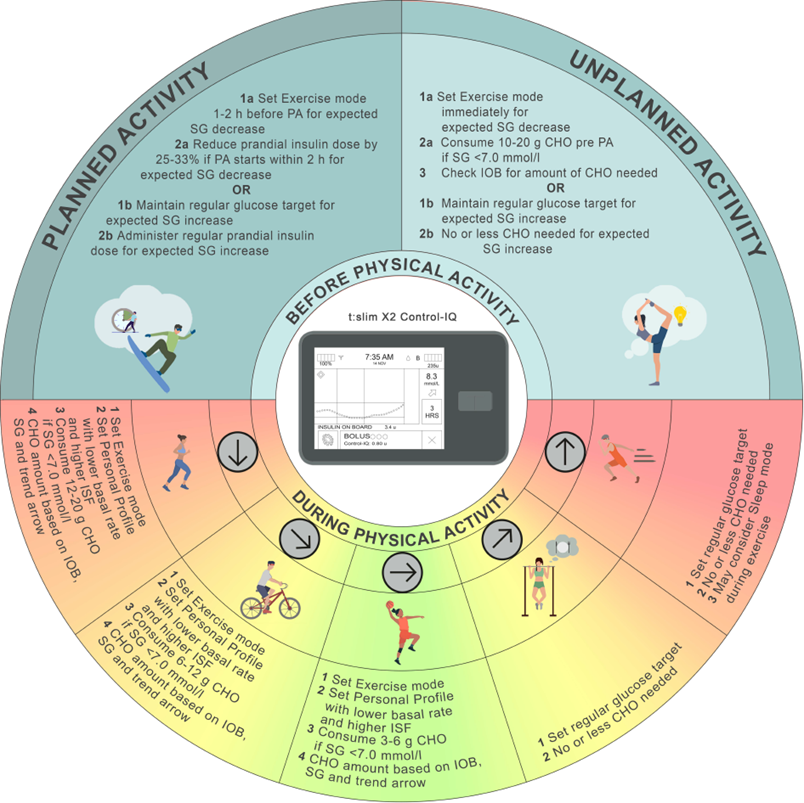
• Tandem t:slim X2 Control-IQ: Incorporates an “Exercise Mode” to manage glucose ranges during activity, complemented by predictive insulin adjustments.
- DBLG1 system: Incorporates a “Physical Activity” mode to manage glucose ranges during activity. Further, there is a ZEN mode that increases the target level.

Each system has unique features and limitations, making it essential to tailor exercise strategies to individual needs and device capabilities.
Practical Guidance for Different Types of Exercise
Physical activity can elicit varying glucose responses depending on the type, intensity, and duration of the activity. Aerobic exercise typically lowers glucose levels, while high-intensity or resistance training may increase them temporarily. Key recommendations include:
• Aerobic Activities: Start with a higher glucose target and consume small carbohydrate amounts to maintain levels within the target range.
• High-Intensity Exercise: Consider reducing insulin doses beforehand and monitor glucose closely to address spikes.
• Prolonged Activities: Additional planning is necessary, including carrying emergency supplies like fast-acting carbohydrates or glucagon to address both hypoglycaemia and hyperglycaemia risks.
Overcoming Challenges and Implementing Recommendations
While AID systems significantly improve glucose management during exercise, challenges remain. These include delays in glucose readings from continuous glucose monitoring (CGM) systems, the need for manual carbohydrate intake adjustments, and variability in individual glucose responses. To overcome these, individuals should:
Empowering Safer, More Enjoyable Exercise
1. Work closely with their healthcare team to understand their unique glucose trends.
2. Use CGM trend arrows and insights to guide real-time decision-making.
3. Regularly review and adjust exercise strategies based on personal experiences and new data.
Struggling with erratic glucose levels?
This often happens because AID systems adjust insulin levels every five minutes or so. As a result, you’ll never start exercising with the same insulin conditions, making your plans inconsistent and non-reproducible.
To overcome this, set a manual basal rate appropriate for your exercise and switch to open-loop mode two hours before starting. This will stabilise insulin conditions, allowing you to use trial and error to determine how many carbs you need to supplement. This plan will be much more reproducible!
Don’t forget to switch back to closed-loop mode afterward to enjoy steady overnight control!
Final Thoughts
Contributing to this consensus statement has been a deeply rewarding experience, and I am confident that the insights shared will help individuals with type 1 diabetes lead active, fulfilling lives. By implementing these practical tools, anyone can exercise safely, improve their health, and enjoy the many benefits of an active lifestyle. For a more detailed exploration of these strategies, I encourage readers to access the full document and consult their healthcare providers for personalised guidance.
If you want to know when a new section of blog is added, click here.
Cheers
John (T1D since 2008)
Dad to Grace and Jude who this blog is written for.
