

In this part, we describe The Ominous Octet and how each one is impacted by having T1D.
Prefer a Podcast? Listen to Episode 14.

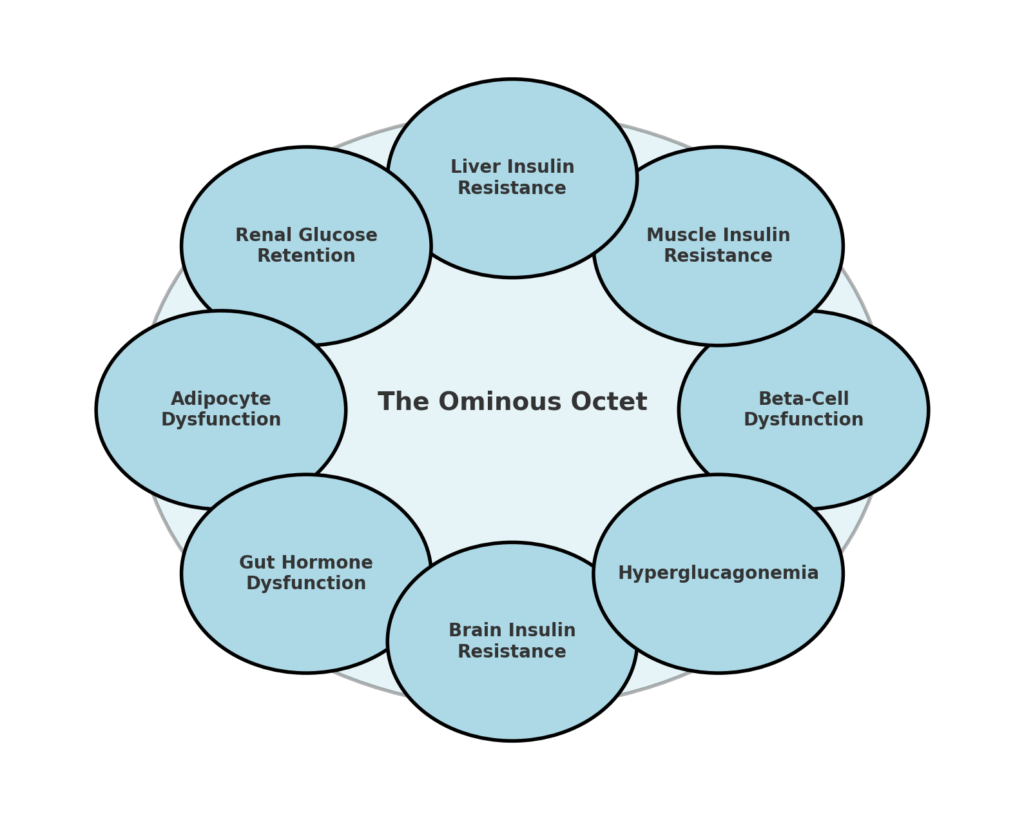
1. Beta-Cell Dysfunction
Even in people with long-standing type 1 diabetes, studies have shown that some beta-cell function may persist for years, particularly in those diagnosed later in life. Just like me. I was diagnosed at 27 and, nearly 20 years later, still have a C-peptide level of 100-150 pmol/L. I fully recognise that this gives me an “easier” experience compared to those with no measurable C-peptide. This means:
- Some insulin may still be produced, even if only in tiny amounts.
- Insulin from Beta cells helps regulate glucagon by directly reducing output by the alpha cell, which is often overactive in T1D.
- Glucose toxicity (high blood sugar) damages beta cells further, leading to even more dysfunction.
If insulin resistance is present, any remaining beta-cell function is even more impaired, making it harder to regulate glucose. Since the insulin released from beta cells suppresses glucagon from the alpha cells, their dysfunction means glucagon levels stay too high, driving excess liver glucose production, especially at night. This means hyperglycemia worsens, and insulin requirements increase as the lack of insulin in the pancreas struggles to suppress glucagon.

2. Muscle Insulin Resistance
Muscle tissue is the largest site for glucose disposal for people living with T1D, taking up about 75% of glucose after meals. If muscle insulin resistance develops, glucose stays in the bloodstream instead of being stored.
The main driver of muscle insulin resistance is fat accumulation inside muscle cells. When too much fat (in the form of diacylglycerols and ceramides) builds up, it blocks insulin signaling, making it harder for glucose to enter muscle cells.
This is why eating a high-fat meal can cause delayed glucose spikes hours later. The excess fat prevents muscles from taking up (via GLUT4 transporters) glucose efficiently. It’s worth showing the diagram again.

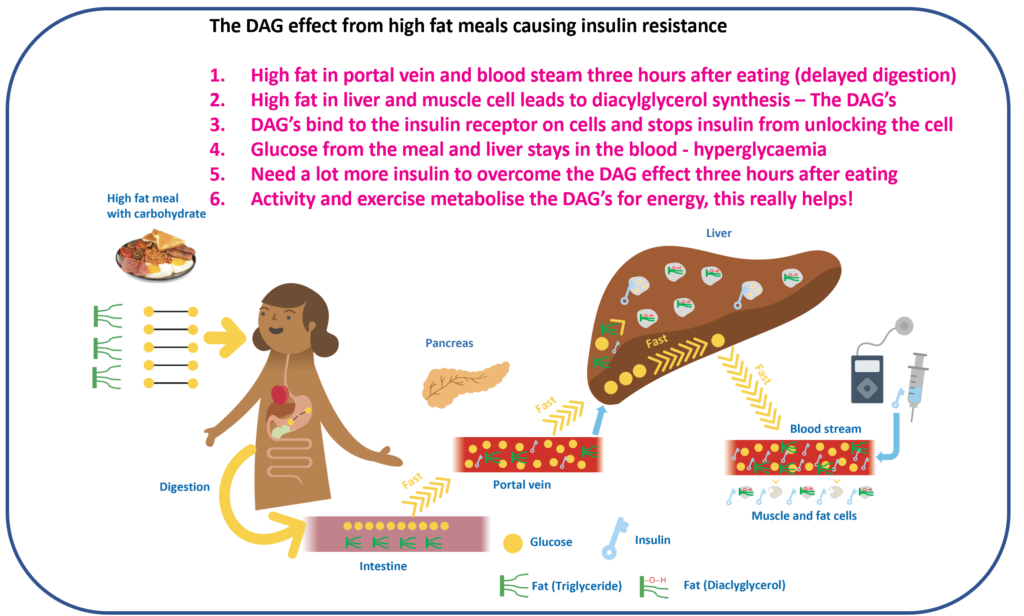
Since muscles aren’t taking up glucose properly, more insulin is needed to compensate. This raises overall insulin levels, leading to:
- More fat storage in muscle worsens insulin resistance further.
- Increased reliance on glucose from the liver, worsening glucose swings.
- Difficulty achieving stable blood glucose despite adjusting insulin doses.
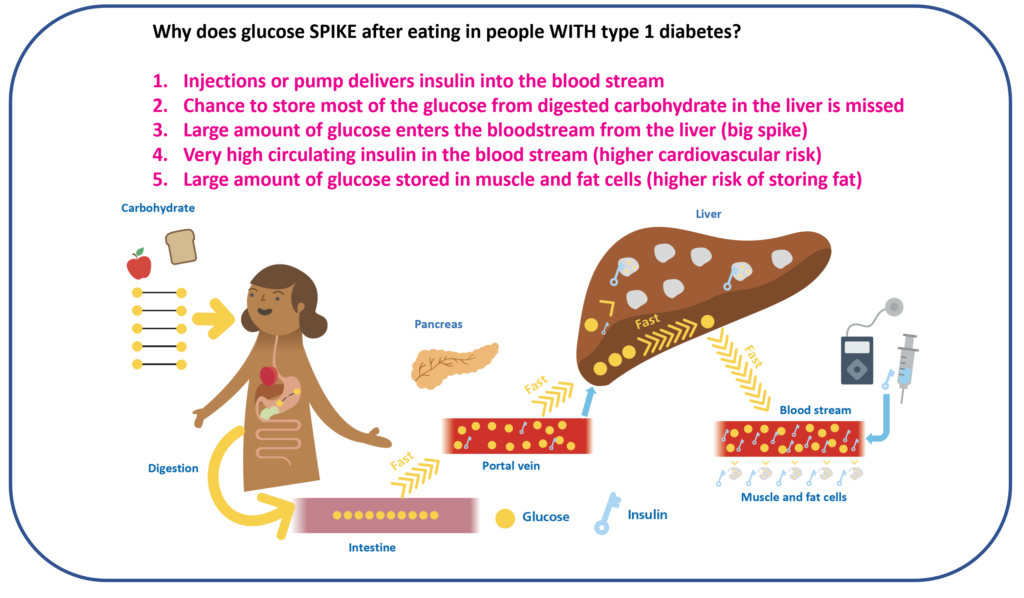
3. Liver Insulin Resistance
The liver is supposed to release glucose when fasting and stop releasing it when eating. The liver normally gets first access to insulin via the portal vein. However, in type 1 diabetes, insulin is injected under the skin, meaning the liver never gets a strong insulin signal.

Because of this:
- The liver continues to release glucose even after meals.
- Insulin resistance further impairs the liver’s ability to shut off glucose production.
- Glucagon levels stay too high, keeping the liver glucose production (glycogenolysis and gluconeogenesis) in overdrive!
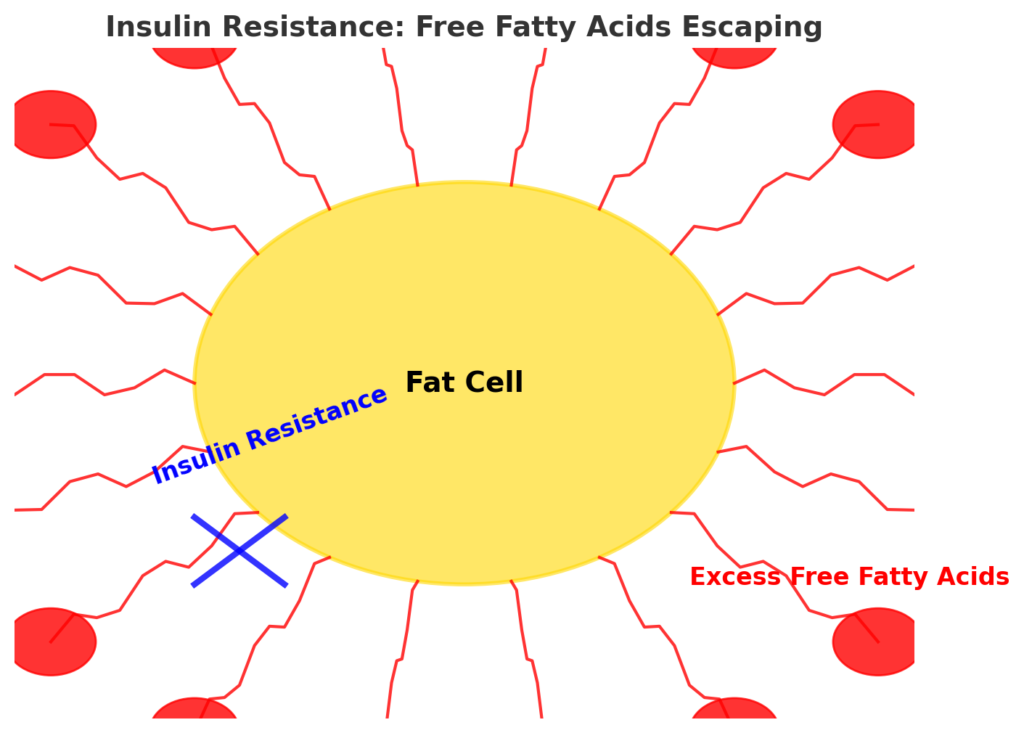
4. Fat Cell Dysfunction
Fat cells play a crucial role in glucose and lipid metabolism. Their main job is to store fatty acids and release them only when the body needs energy. Typically three to five hours after eating.
However, in insulin resistance, fat cells start releasing excessive free fatty acids (FFAs) continuously, instead of only when needed. This excess FFA release makes it harder for insulin to work effectively, contributing to metabolic dysfunction.
When this happens:
- Fat cells become resistant to insulin’s ability to keep fat stored (its anti-lipolytic effect), leading to the excessive release of free fatty acids. In theory, this could be beneficial since fat can be used for energy. However, in an insulin-resistant state, there is already an excess of available energy, making these extra free fatty acids problematic.
- High levels of FFAs block insulin signaling in muscle and liver cells, reducing glucose uptake.
- Excess FFAs increase glucose production in the liver, worsening hyperglycemia.

This means that people with higher insulin resistance often experience:
- Difficulty in losing weight, since excess FFAs continue circulating causing insulin resistance.
- More glucose variability, as FFAs drive liver glucose production.
- Higher insulin requirements, due to excess FFA uptake into the muscle and liver cells and the consequent DAG effect discussed above.
5. Kidney Dysfunction
The kidneys filter around 180 grams of glucose daily, deciding whether to reabsorb or excrete it in urine. If the glucose level goes above 10.0 mmol/L (180 mg/dL) the kidneys dump glucose in the urine. The SGLT2 transporter is responsible for reabsorbing 90% of the glucose filtered by the kidneys.

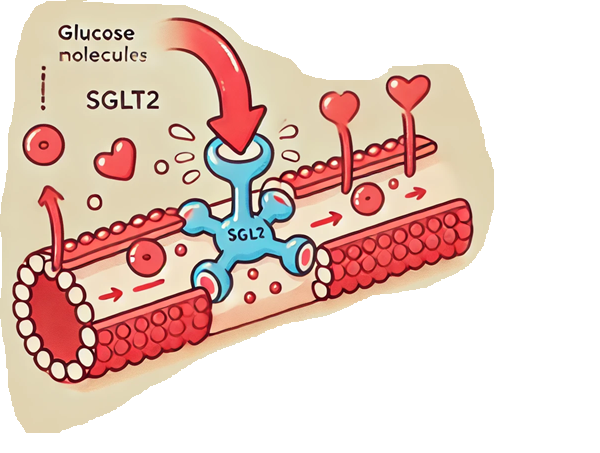
When insulin resistance is present, the kidneys overcompensate by upregulating SGLT2, meaning even more glucose is retained, making hyperglycemia worse. This creates a vicious cycle:
- Higher glucose levels increase SGLT2 activity, causing more glucose reabsorption.
- More glucose stays in circulation, leading to higher insulin needs.
- Higher insulin levels further increase insulin resistance, worsening the problem.
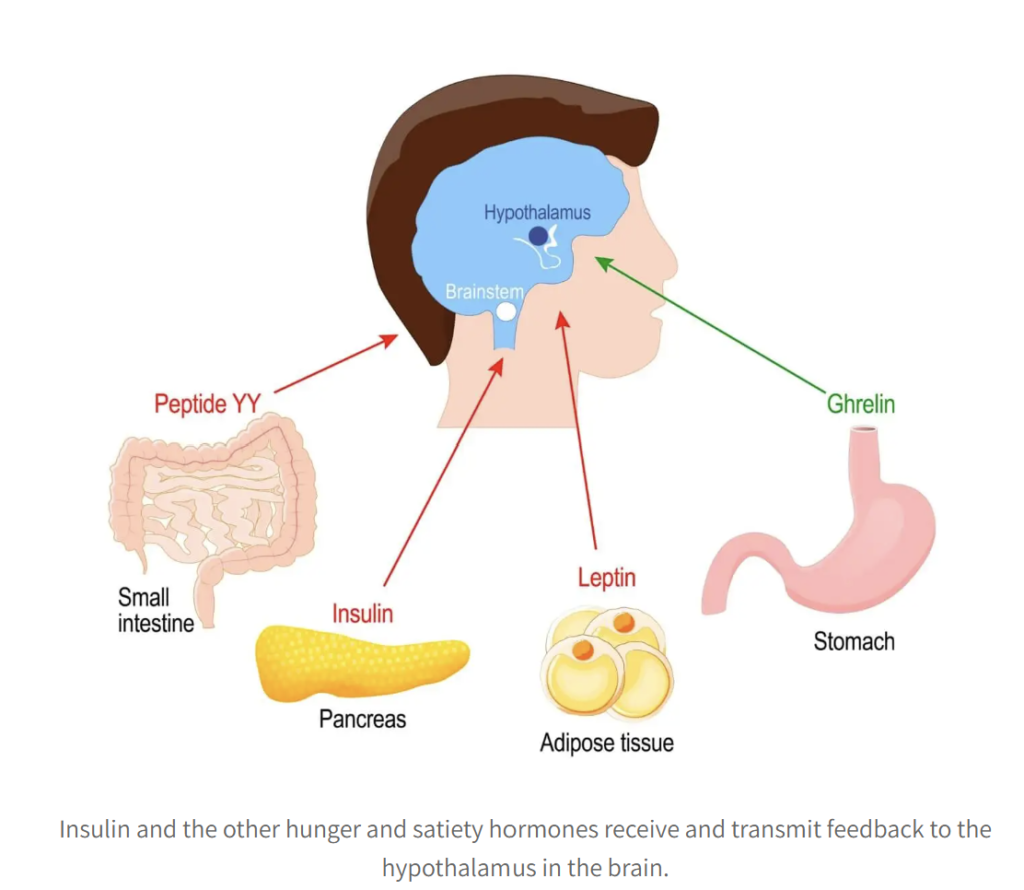
6. Brain Insulin Resistance
The hypothalamus in the brain is responsible for regulating hunger, metabolism, and energy balance. Insulin plays a key role in this process by signaling satiety; in other words, it tells your brain when you’ve had enough to eat. In insulin resistance, the brain stops responding properly to insulin, leading to (as depicted in the fantastic graphic):
- Increased hunger and food cravings.
- Greater difficulty with weight management.
- Higher insulin needs due to increased caloric intake.

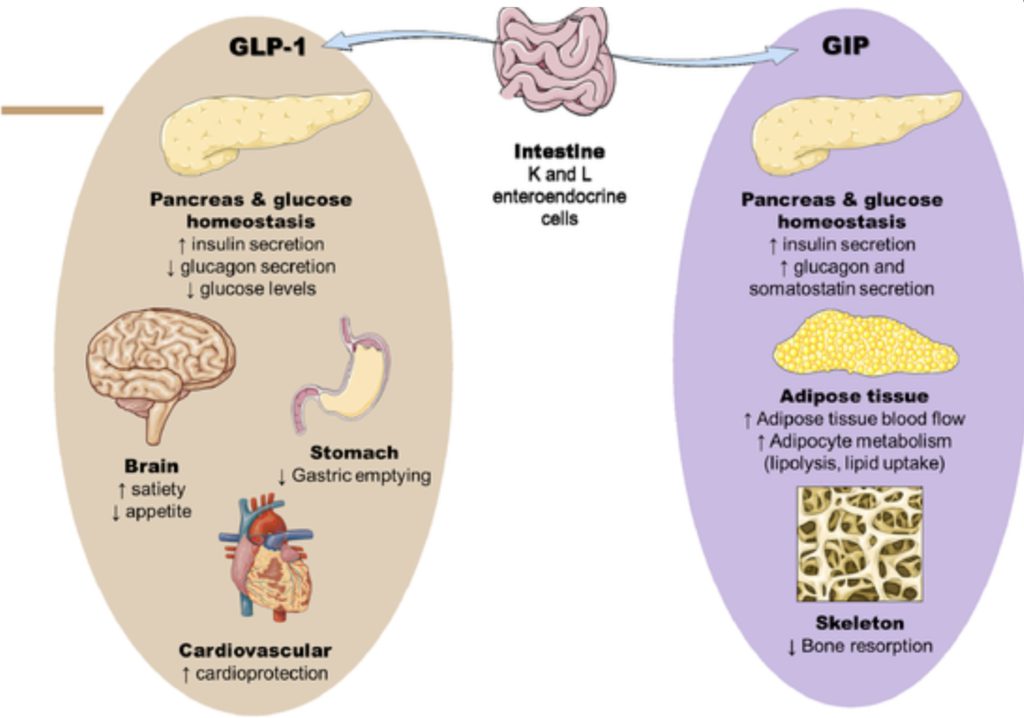
7. Gut Hormone Dysfunction
After eating, K and L cells in the gut release GLP-1 and GIP, which play several important roles:
- Stimulate insulin release from whatever Beta cells still function
- Suppress glucagon production
- Signal the brain that we are full
- Slow down the stomach’s emptying process
However, in insulin resistance, the body becomes resistant to the effects of GLP-1 and GIP. This leads to a cascade of negative effects, as you can imagine from this wonderful graphic.

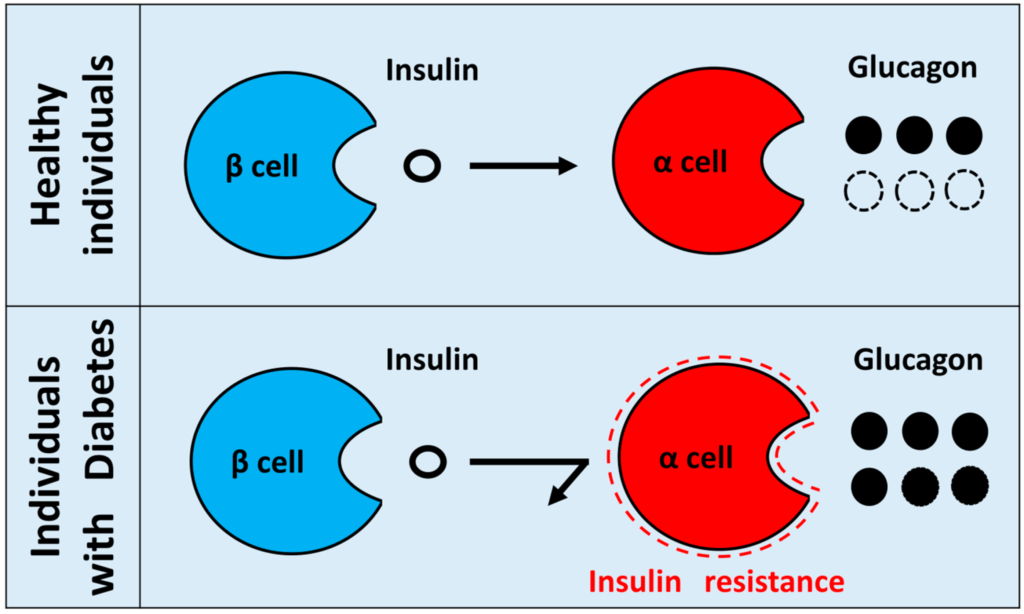
8. Hyperglucagonemia
Glucagon is the opposite of insulin, it tells the liver to release more glucose when needed. In type 1 diabetes, glucagon levels are often too high, leading to excess glucose output from the liver, especially overnight. As you know by now, insulin resistance and hyperglucagonemia go hand in hand!
It’s time to shift gears to how to overcome insulin resistance with T1D.
A reminder of the pyramid.
The pyramid format helps illustrate how different solutions work together, considering three key factors: effectiveness, accessibility, and side effect profiles.
- Clear boxes represent lifestyle interventions.
- Dark boxes represent pharmacological options.

If insulin resistance has eight different causes, can one strategy alone be enough? Unlikely.
You’ll likely need a combination of approaches, depending on where you’re starting from.
Part 3, dives into the seven solutions for insulin resistance.
