

Prefer a Podcast series?
Yes, listen to the CGM 3-Part Series
A quick recap from Understanding Risk Before Performance.
The only CGM Systems tested with a study design meeting basic criteria are:
- Accu-Chek SmartGuide
- Dexcom G6 and One
- Dexcom G7 and One+
- FreeStyle Libre 2 and 3 Plus
- Medtronic Guardian 4
- Medtronic Simplera
Ideally, CGM accuracy should be assessed against capillary glucose rather than venous glucose.
Capillary glucose represents the highest glucose levels that micro-vessels, such as those in the eyes, kidneys, feet, sexual organs, and nerves, are exposed to, making it the key driver of long-term complications.
In contrast, venous glucose tends to underestimate peak glucose exposure, which can lead to a misleadingly lower assessment of risk.
Remember how the Medtronic Simplera underreports post-meal glucose exposure because it aligns closely with venous glucose values rather than capillary.
In contrast, the Dexcom G7 and FreeStyle Libre 3 track much more closely to capillary glucose, which reflects accurately what the human body is exposed to (the study).

However, data comparing CGMs directly against capillary glucose is not consistently available for all systems. Given this limitation, I have initially summarised the accuracy of all the CGMs based on their performance against venous glucose, ranking them into two categories. Capillary comparisons, including the Accu-Chek SmartGuide, come after.
Top Band: CGM systems meeting the 15/15, 20/20, and 40/40 iCGM Performance Standards. These systems meet the highest accuracy standards, ensuring reliable performance in hypoglycemia (<3.9 mmol/L or <70mg/dL) target range (3.9-10.0 mmol/L or 70-180 mg/dL), and hyperglycemia (>10.0 mmol/L or 180 mg/dL)
- Dexcom G6 (Dexcom One is identical except for reduced functionality)
- Dexcom G7 and (Dexcom One+ is identical except for reduced functionality)
- FreeStyle Libre 2 and 3 Plus
Second Band: Approved CGMs (Non-iCGM). These CGMs do not meet iCGM criteria when assessed against venous glucose, but they are still accurate enough for treatment decisions.
- Medtronic Guardian 4
- Medtronic Simplera
But the Real Question Is…
How accurate are the leading CGM systems against capillary glucose?
That’s what matters because capillary glucose better reflects the risk of complications. If CGMs align with venous glucose, they may not provide the most meaningful insight for long-term health compared to CGMs aligned with capillary glucose levels.
Fortunately, the current generations have been tested against capillary glucose, so let’s take a look at them
- Accu-Chek SmartGuide
- Freestyle Libre 3 (Freestyle Libre 2 has the same sensor technology and algorithm)
- Dexcom G7 (Dexcom One+ has the same sensor technology)
- Medtronic Simplera
Before we take a look, here is an important note about the testing methodology:
- Freestyle Libre 3, Dexcom G7, and Medtronic Simplera were tested independently using the Dynamic Glucose Region (DGR) Challenge. The most rigorous approach evaluates performance under rapid glucose fluctuations, making it a more robust assessment of accuracy, but it will give the appearance of lower accuracy.
- Accu-Chek SmartGuide Study, although it did use meal and insulin challenges, the DGR Challenge was not used. While it provides valuable data, it has not been tested under the same conditions as the others, biasing it towards higher accuracy when compared to the others tested under DGR conditions. This is no different from all the CGM systems that achieved iCGM approval with a similar study design, they did not use a DGR challenge either.
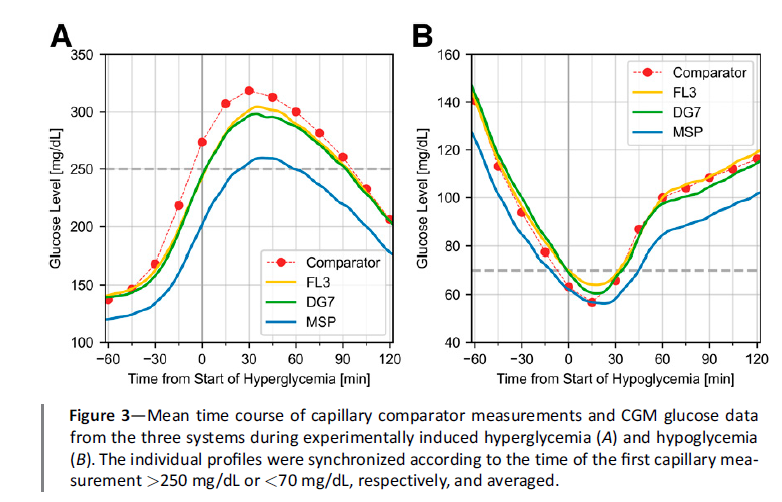
This graph illustrates a DGR test (red line), which evaluates rapid glucose rises after a meal without insulin, followed by a sharp drop after a high insulin dose during the same study visit.
In contrast, when the meal (blue line) and insulin (green line) challenges are conducted on separate visits, glucose fluctuations occur more gradually, and the CGM is not pushed to its limits.


Using a CGM that has been evaluated using a DGR challenge is like using a car that’s been tested the way glucose sometimes behaves, like a rollercoaster! For example:
- Food without insulin followed by several rage boluses in quick succession (guilty on more than one occasion!)
- Undertaking exercise within 90 minutes of eating (high amount of insulin on board, my nemesis!)
- Very late bolus for food when using an AID System (I have seen many times in clinic, but I don’t use one, so I have not had the personal experience)

Performance Metrics
There are many accuracy metrics, each with its limitations. Mean Average Relative Difference (MARD), the most commonly used metric, provides an overall average error but does not account for the risks associated with extremely high or low glucose levels.
A useful way to understand this is by asking:
“Would you cross a river if its average depth were 4 feet, even if you couldn’t swim?”
If your answer is yes, you may not fully grasp risk.
The extremes are where the most critical decisions happen!
Agreement Rates Indicate Risk
Agreement rates indicate the percentage of readings that fall within an acceptable range, such as 20/20 and 40/40.

Let’s start with the 20/20 metric, which gives a clear clinical benchmark for what counts as an “accurate” or “no risk” CGM reading. It works like this:
- If your CGM reports a value below 5.5 mmol/L (100 mg/dL), it’s considered accurate if the matched blood glucose (from a lab test or a high-quality fingerstick) is within ±1.1 mmol/L (or ±20 mg/dL).
- For instance, a CGM value of 4.5 mmol/L (80 mg/dL) would be considered on target if the actual glucose falls between 3.4 mmol/L (60 mg/dL) and 5.6 mmol/L (100 mg/dL).
- If your CGM shows a value at or above 5.5 mmol/L (100 mg/dL), then the reference glucose needs to fall within ±20% of the CGM reading.
- So a CGM reading of 10.0 mmol/L (180 mg/dL) would count as accurate if the true value lies between 8.0 mmol/L (144 mg/dL) and 12.0 mmol/L (216 mg/dL).
The more readings landing within this 20/20 range, the more dependable the CGM is, especially when safely dosing insulin based on sensor data.
The 40/40 metric offers a wider lens. It’s less about perfection and more about identifying how often CGM readings stray far enough to risk mistreatment, like giving a correction dose when none is needed or missing a hypo.
Here’s how it breaks down:
- For CGM readings under 5.5 mmol/L, the paired blood glucose must fall within ±2.2 mmol/L (or ±40 mg/dL).
- So, a CGM value of 4.5 mmol/L (80 mg/dL) would need a reference between 2.3 mmol/L (20 mg/dL) and 6.7 mmol/L (120 mg/dL) to make the cut.
- For readings 5.5 mmol/L (100 mg/dL) or higher, the acceptable range is ±40%.
- That means a CGM showing 10.0 mmol/L (180 mg/dL) needs a reference between 6.0 (108 mg/dL) and 14.0 mmol/L (252 mg/dL) to be deemed within bounds.
If a CGM often misses even the broader 40/40 window, that’s a red flag, these readings are very likely to cause dosing mistakes.
Now let’s see how the CGM systems stack up using the DSN Form UK Chart (published with permission)

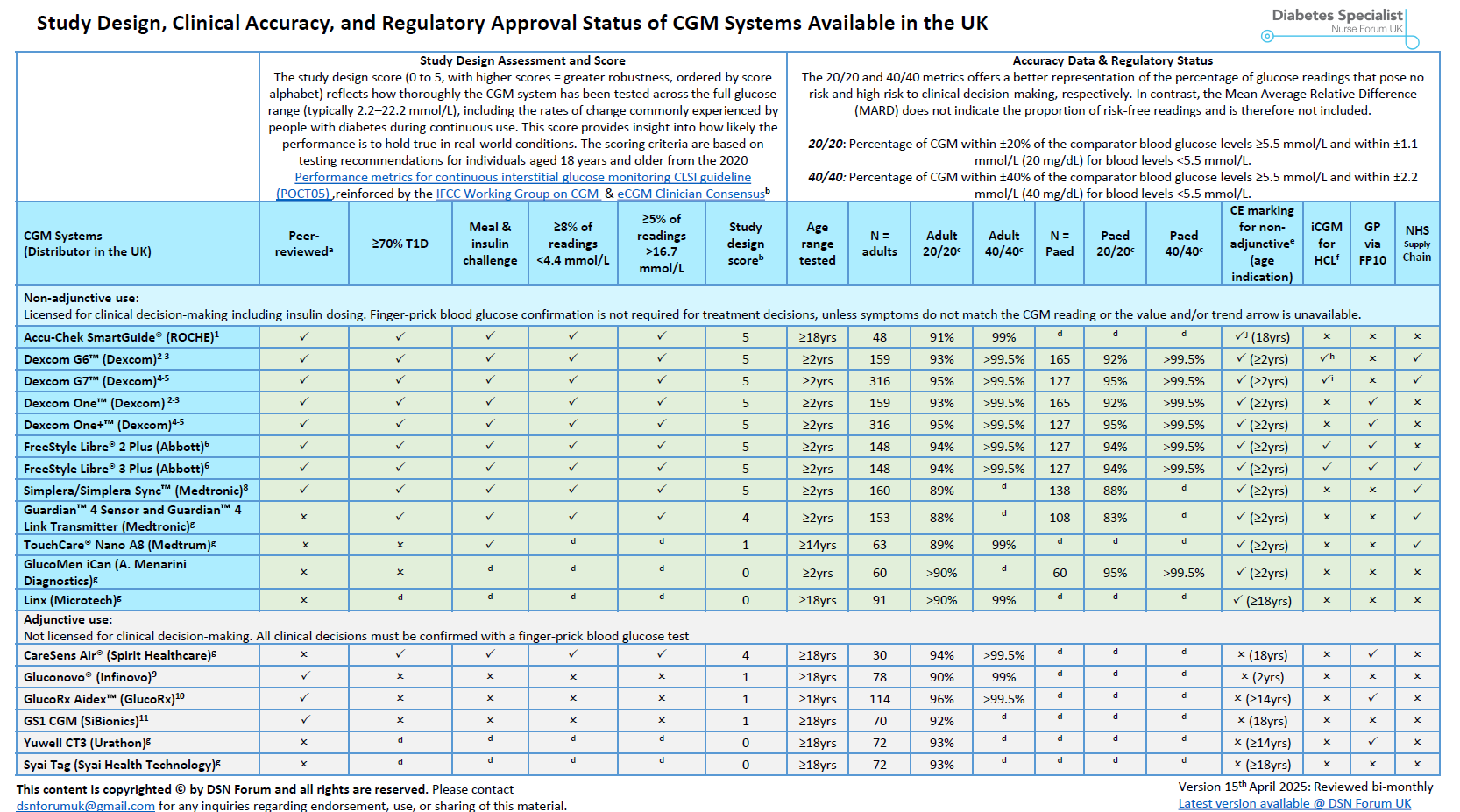
Comparing CGM Systems: A Note of Caution
You’ll often see tables like the one above reporting how various CGM systems perform on the 20/20 and 40/40 metrics. While these are useful for identifying systems that meet minimum safety standards, they’re not direct head-to-head comparisons. The studies behind these numbers differ widely, including different populations, different protocols, and different reference standards.
In my view, if a CGM has been tested under robust conditions (study design score of 4 or more), then achieving around 90% of readings within the 20/20 accuracy range indicates a high level of no-risk insulin decisions.
If 99% or more of readings fall within the 40/40 range, fewer than 1% of readings will result in a high-risk insulin dosing decision.
Together, these thresholds provide strong reassurance that the CGM system can confidently guide insulin decisions with minimal risk.
But you decide on what you think is an acceptable risk.
When a CGM system meets the iCGM performance standards (which uses venous glucose as the comparator) it is considered highly accurate. iCGM approval provides ultimate reassurance.
However, when a DGR test (described above) is used with capillary glucose as the comparator, the criteria become overly strict and virtually impossible to meet. Even top-performing CGMs like the Dexcom G7 and Freestyle Libre 3 fail to meet these standards.
This chart shows (orange and red) that even the most accurate CGMs we have fail to meet iCGM standards when tested robustly with a DGR test.

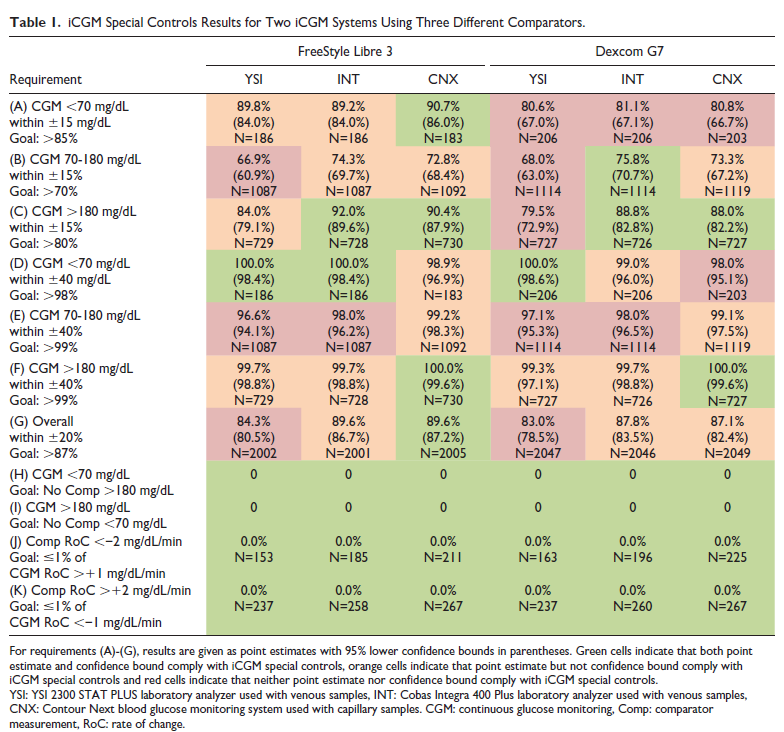
This does not mean the market-leading sensors have suddenly become less accurate overnight! Instead, it highlights that when a rigorous study protocol (DGR test) is followed using capillary glucose as the comparison, meeting the iCGM Performance Standards becomes virtually impossible.
Therefore, once CGM testing is standardized by the IFCC team, updated performance criteria will need to be developed to reflect these new standards.
So, is it time for DGR performance standards?
I hope I have made a strong case, as I believe so.
We need performance metrics that test candidate CGM systems in the five critical DGR Regions: BG low, Alert Low, Neutral, Alert High, and BG High.

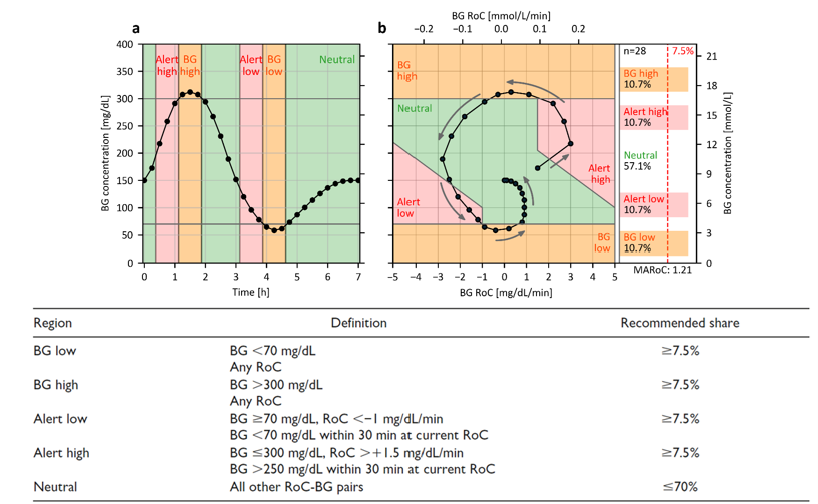
Why Five Regions?
This approach gives us a perspective on sensor accuracy when glucose levels are dropping toward hypoglycemia or rising rapidly to high levels. Therefore, the reported accuracy of sensors will reflect what we, as users, experience from time to time. This will help us understand when sensors are most reliable and when we need to be more vigilant.
Hint:
We must be especially mindful during rapid glucose changes, especially drops caused by exercise. This has been highlighted by Professor Othmar Moser and the wide range of experts who authored the CGM and AID international guidelines for exercise and T1D. It’s always wise to listen to a consensus when compiled by experts in the field!
However, the DGR metrics and standards are not ready yet.
Any other performance metric?
Last up, a measure that has multiple zones, and visually allows us to assess risk and compare performance?
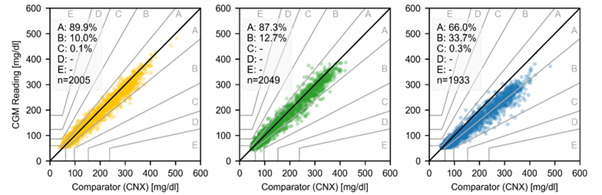
The DTS Error Grid
The Diabetes Technology Society (DTS) Error Grid is a tool designed to evaluate the clinical accuracy of blood glucose monitoring systems by assessing the potential risks associated with measurement errors. It compares the glucose readings from a device to comparator values and categorises the differences based on their potential impact on patient care.
The horizontal axis (x-axis) represents the true blood glucose values (in our case, capillary glucose). The vertical axis (y-axis) shows the glucose values measured by the device being evaluated (in our case, the CGM System values).
Zones: The graph is divided into different zones, each indicating a level of risk associated with the discrepancy between the CGM and comparator (capillary in our case) values:
- Zone A: Differences here are clinically insignificant, meaning the device’s readings are accurate enough for safe and effective treatment decisions.
- Zone B: Represents minor errors that would lead to benign or no treatment changes.
- Zone C: Indicates discrepancies that could lead to overcorrection or unnecessary treatment adjustments.
- Zone D: Errors here might cause a failure to detect and treat hypo- or hyperglycemia.
- Zone E: This signifies errors that could result in dangerous treatment decisions, such as administering insulin when it’s not needed, potentially leading to severe hypoglycemia.
Using the DTS Error Grid, we can compare the Freestyle Libre 3 (yellow), Dexcom G7 (green), and Medtronic Simplera (blue), using the data from the three-sensor study that used capillary as the comparator and performed a DGR Challenge.

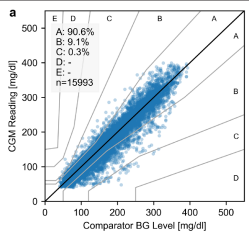
Also, the Accu-Chek SmartGuide Study used an older Consensus Error Grid with less robust meal and insulin challenges, but it’s still very informative and shows good accuracy.

What do the results mean?
The following systems have approximately 90% of their readings carrying no clinical risk, while the remaining 10% pose only a slight risk, with virtually no readings carrying high risk:
- Dexcom G7 (Dexcom One+ uses the same sensor technology, algorithm, and hardware as the G7.)
- Freestyle Libre 3 (Freestyle Libre 2 shares the same sensor technology and algorithm, so its accuracy is expected to be almost identical, as only the hardware is different.)
- Accu-Chek SmartGuide
In contrast, the Medtronic Simplera underreports capillary glucose levels significantly, with only 66% in Zone A (no risk), which has important clinical implications:
- Hypoglycaemia Management – There is almost no risk of missing a true low glucose level (hypoglycaemia), but the system is likely to incorrectly indicate hypoglycaemia when the person’s capillary glucose is in a safe range. This may be very helpful for those with serious hypo issues, but can lead to unnecessary treatments for low blood sugar when it’s not needed.
- Hyperglycaemia Management – The Simplera also underestimates high capillary glucose levels, which presents issues for individuals using Automated Insulin Delivery (AID) systems or those manually managing insulin with pens or pumps:
- AID users may miss important insulin corrections if their sensor glucose readings appear within range while their actual capillary glucose is higher. However, the SmartGuard algorithm in the 780G is particularly aggressive, providing approximately 5% more time in range compared to the t:slim X2 with Control-IQ. This increased time in range compensates for the underreporting of capillary glucose, ensuring that HbA1c levels remain equivalent between the systems. However, this equivalence is only achieved due to the 5-7% higher time in range.
- On the other hand, people using insulin pens or non-automated pumps may not adjust their insulin dosing if their sensor glucose appears in range, even when their actual capillary glucose is higher. As a result, achieving a 70% time-in-range with the Simplera sensor may not offer the same level of protection as a 70% time-in-range with a Dexcom, FreeStyle Libre, or Accu-Chek SmartGuide system, despite users putting in the same effort.
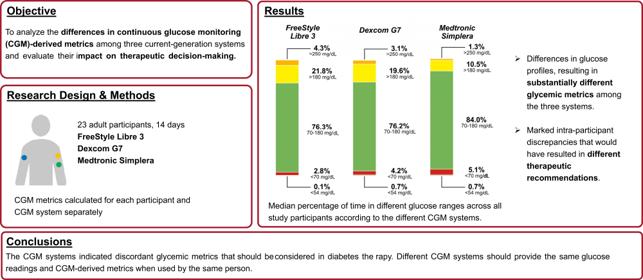
- Remember this?
The Medtronic Simplera tends to overestimate time in range (3.9–10.0 mmol/L or 70–180 mg/dL) by around 8% and time in tight range (3.9-7.8 mmol/L) by 13%! This isn’t a sensor fault, it’s because it aligns closely with venous glucose. Capillary glucose reflects the highs that matter day to day. So while Simplera is an accurate representation of venous glucose, it’s likely underestimating capillary time above range (>10.0 mmol/L or 180 mg/dL) by 10%! See the study for details.

Medtronic has partnered with another CGM manufacturer to develop future sensors. Combining a sensor that aligns with capillary glucose with the 780G algorithm could be a knockout combination!
Takeaway
If you are comfortable with venous glucose comparisons, an iCGM-approved and FDA-Cleared CGM should be your first choice.
However, for the most accurate reflection of capillary glucose levels, what matters most for day-to-day management, CGMs like the Dexcom G6/G7/One/One+, Freestyle Libre 2 Plus, Freestyle Libre 3 Plus, and Accu-Chek SmartGuide are ideal choices.
Now that you have a clearer understanding of accuracy, the next section explores all the bells and whistles, such as…
- Factory Calibration vs Manual Calibration (choose a blood glucose meter that aligns with your CGM System)
- Optional Calibration
- Alarms
- AI-powered systems
- Sensor wear duration
- Followers
- Hardware
- Integration with automated insulin delivery (AID) systems
- Age restrictions
2 responses to “Assessing CGM Accuracy Performance”
-
Thank you for your amazing work, so interesting and so clear to a non-medical audience! I wanted to mention another important factor with CGMs now that we are in the era of widespread AID system use – connectivity. Many of us have recently had to switch to the Libre2+ for cost reasons. It is CE marked to work with the Omnipod, and they seem to have obtained this approval on the basis of equivalence with the Dexcom G6, but in fact the connectivity is not at all the same. Many of us experience signal loss issues (I’ve seen two people report just this week that this landed them in hospital with DKA). For me that has been only an inconvenience, but I was alarmed to be informed by Insulet that I should only use my pod on the same arm as a sensor, no other sites are reliable. So no real site rotation. I can put them above and below a sensor, but I worry about the longer term impact of this. Please could you look into this for us? Your patients may be facing similar issues.
🙏🏻
-
Hi Emma, I hear what you are saying. I will look to include this in the upcoming CGM Series. Thanks for the kind words! X
-


Thank you for your amazing work, so interesting and so clear to a non-medical audience! I wanted to mention another important factor with CGMs now that we are in the era of widespread AID system use – connectivity. Many of us have recently had to switch to the Libre2+ for cost reasons. It is CE marked to work with the Omnipod, and they seem to have obtained this approval on the basis of equivalence with the Dexcom G6, but in fact the connectivity is not at all the same. Many of us experience signal loss issues (I’ve seen two people report just this week that this landed them in hospital with DKA). For me that has been only an inconvenience, but I was alarmed to be informed by Insulet that I should only use my pod on the same arm as a sensor, no other sites are reliable. So no real site rotation. I can put them above and below a sensor, but I worry about the longer term impact of this. Please could you look into this for us? Your patients may be facing similar issues.
🙏🏻
Hi Emma, I hear what you are saying. I will look to include this in the upcoming CGM Series. Thanks for the kind words! X