Foundations, Part 3
Basal Insulin
Basal insulin is background insulin, covering the glucose your liver releases all day and night, independently of food. Understanding basal is the first step in making sense of everything else.
What is basal insulin?
Basal insulin covers the glucose your liver releases continuously. It works independently of food and can be delivered in two ways: long-acting injections, which provide a relatively flat insulin profile, or pump basal, which allows delivery to vary hour by hour.
When basal insulin is close to right, glucose overnight tends to stay roughly flat when there is no food or bolus insulin in the system. When basal is mismatched, glucose may drift up or down in the background, making everything else harder to interpret.
This is why basal insulin appears early in the Foundations sequence. If basal is off, bolus insulin can feel unpredictable, corrections can feel random, and diabetes management can start to feel personal when it isn’t.
The mechanism
Your liver continuously releases glucose into the bloodstream. That output is not flat, it changes across the day and night in response to hormones, sleep, stress, illness, exercise, alcohol, and earlier food intake.
Basal insulin’s role is to move this liver-derived glucose into cells for energy. It is not designed to cover meals, and it cannot respond quickly to rapid glucose changes.
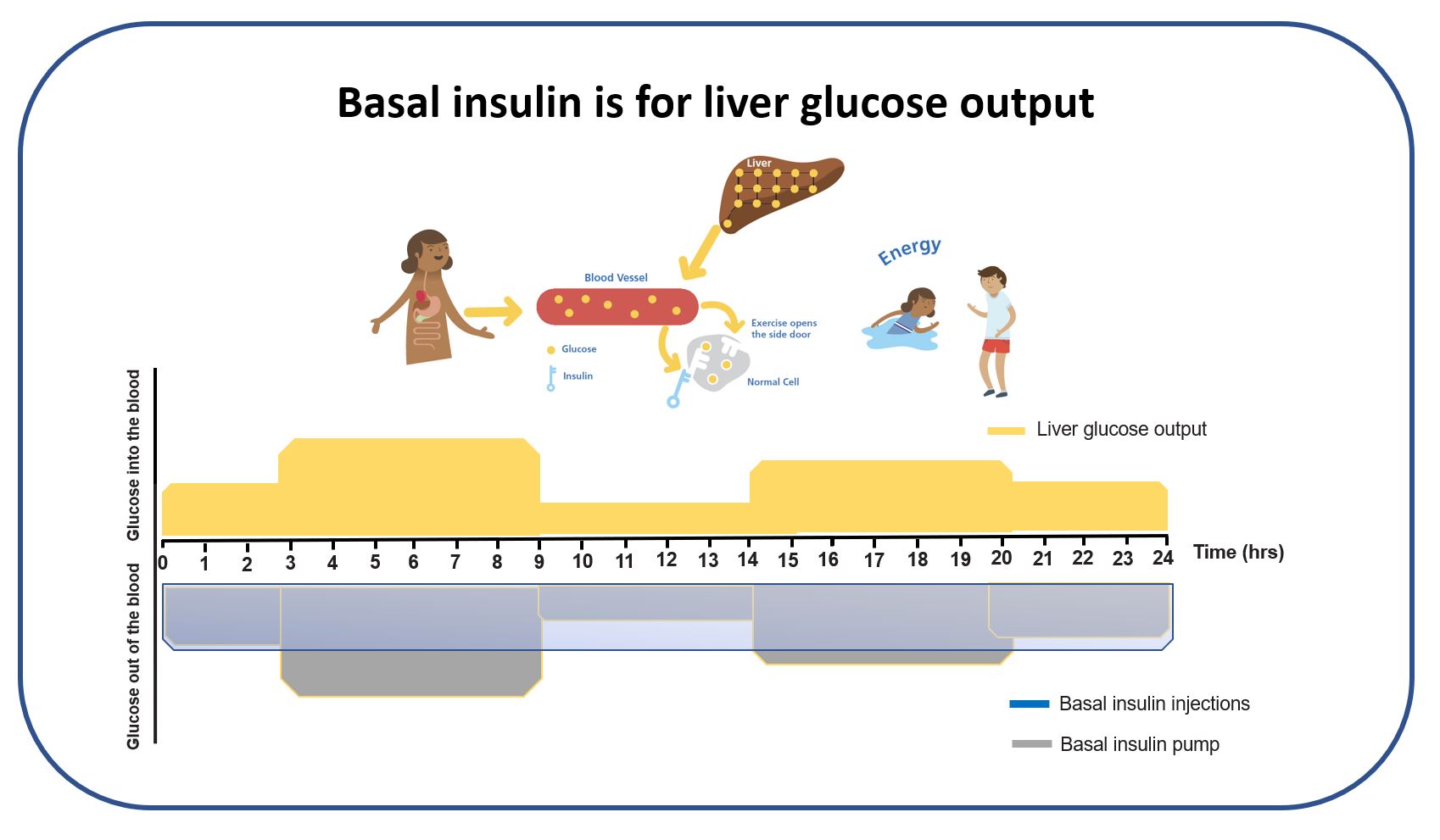
The graphic above illustrates the core basal challenge: liver glucose output rises and falls across the day, while insulin delivery, particularly with injections, is often relatively fixed.
Basal by injection (long-acting insulin)
Long-acting basal insulin is designed to work steadily over many hours. Examples include Lantus, Levemir, and degludec (Tresiba). The aim is to provide a stable background insulin level.
The limitation is that liver glucose output is not stable. As a result, glucose may tend to rise at some times of day and fall at others, even when the total daily basal dose is reasonable. This mismatch is one of the most common reasons people notice unexplained overnight drift or daytime dips.
This also helps explain why people who retain some endogenous insulin production often find overnight stability easier: even small amounts of internal insulin can buffer basal mismatch.
Basal by pump (fast-acting insulin)
With insulin pumps, basal is delivered using fast-acting insulin in tiny amounts throughout the day and night. The defining feature is flexibility: pump basal can be adjusted hour by hour to better match the variation in liver glucose output.
Fast-acting insulins used in pumps include NovoRapid, Humalog, Apidra, Fiasp, and Lyumjev. In practice, pump users often use multiple time blocks across 24 hours. The goal is not perfection, but reducing mismatch.
Illustrative example: a pump basal profile may be set higher overnight and lower during parts of the day, while keeping the total daily basal similar. This reflects physiology rather than fighting it.
Pump therapy is not suitable or desirable for everyone. Injections can work extremely well. Understanding why mismatch happens helps shift the explanation away from behaviour and back onto biology.
How to assess whether basal is set well
Basal insulin is easiest to assess overnight, when food, bolus insulin, and activity are largely absent. This exposes the background insulin signal more clearly.
- Relatively stable overnight glucose suggests basal is close to right.
- Consistent overnight rises tend to suggest basal may be insufficient.
- Consistent overnight drops tend to suggest basal may be excessive.
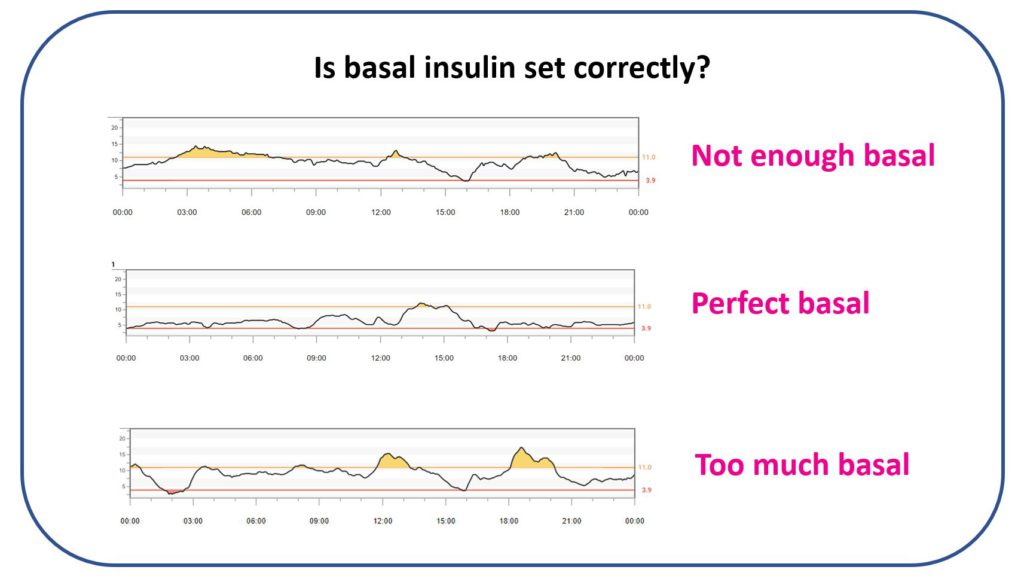
The graphic above shows glucose remaining broadly stable overnight, this is what “close enough” basal often looks like in practice.
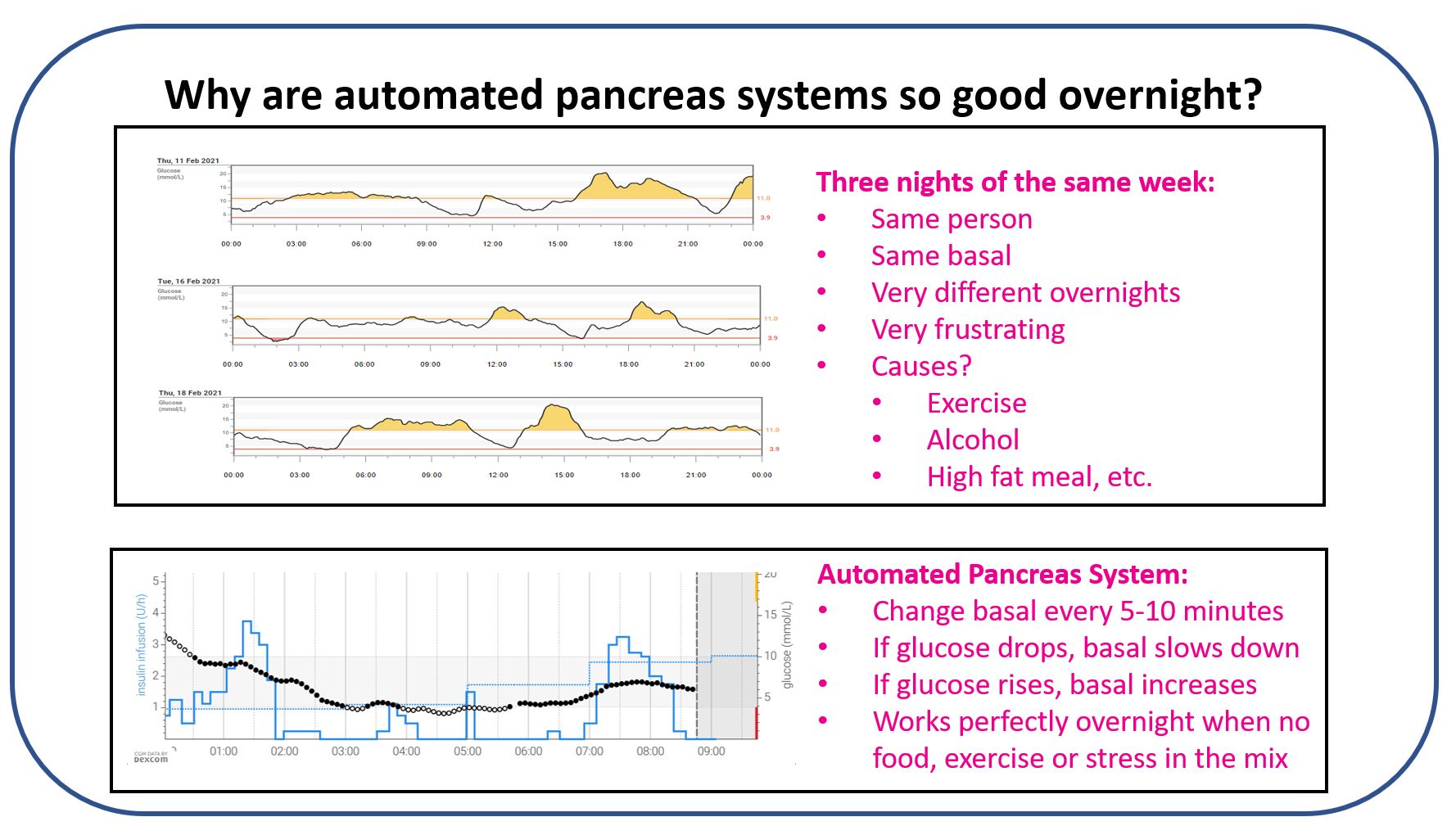
Liver glucose output varies night to night depending on the day’s inputs. Single nights are not reliable signals; repeated patterns across multiple nights matter much more.
- Liver output is often higher after very high-fat evening meals.
- Liver output is often lower on exercise days.
- Liver output can be minimal after heavy alcohol intake.
This variability is worth exploring with CGM data over time. A CGM with alarms is particularly valuable overnight for this reason.
Why AID systems tend to perform well overnight
Automated insulin delivery (AID) systems adjust basal insulin in response to CGM trends, increasing or decreasing delivery as glucose changes.
Overnight, when glucose moves slowly and there is no food, bolus insulin, exercise, or stress in play, AID systems consistently outperform fixed basal delivery. This is not because they are clever, but because basal needs are not static.
Insulin is a slow mover of glucose. Basal changes work overnight where the timescale is hours; during the day, faster tools tend to be needed for meaningful effect. Foundations Part 11 covers this in full.
What this means in practice
- Overnight CGM traces are the best window into whether basal is set well, look for repeated patterns, not single nights.
- Basal mismatch is a biological issue, not a personal failing. Understanding the mechanism helps reframe frustration.
- Pump basal allows hour-by-hour adjustment; injection basal does not, but both can work well when matched thoughtfully.
- AID systems tend to improve overnight results because they respond to the variability in liver output that fixed delivery cannot anticipate.
- Daytime glucose management requires faster tools, this is where the next pages in Foundations come in.
This content is for educational exploration only. It describes average responses and general principles. It is not medical advice and cannot replace individual clinical guidance from your diabetes care team.
Part 3 of 12
Basal Insulin
Read more on GNL
Insulin module, Part 2 of 2
Read Part 2: Bolus insulin
This page covers basal insulin (Part 1). Bolus insulin is the meal-time and correction partner; together they form the Foundations J2 insulin module.
Continue to Bolus Insulin (Part 2)