The Glucose Never Lies®
GNL Grace
Learn type 1 diabetes, the way that fits you. One curriculum of thirty modules, shaped around the learner in front of it, from newly diagnosed to clinician.
How it works
How Grace teaches
There is one curriculum, thirty modules, climbing from the safe basics to appraising the evidence. Grace adapts that same material to you: the depth, the framing, the worked examples, all shaped around where you are starting and how you learn. A newly diagnosed person and a clinician can study the same module and meet it very differently. You earn each tier as you go.
The curriculum
The learning map
The full thirty, tier by tier. Live guides open now; the rest are being rebuilt to the same standard and will light up as they land. Whichever guide you open, Grace can take you through it at the right depth for you.
The essentials everyone with type 1 needs. The safe basics, taught plainly, with no insulin-dose changes asked of you.
How the systems actually work, and the dose-changing levers. The mechanisms behind the day-to-day.
Appraising the evidence. Where the numbers come from, how good they are, and where individual variation takes over.
Where this sits
How this maps to the national technology framework
There is a UK-wide, four-tier competence framework for diabetes technology (Richardson and colleagues, Diabetic Medicine, 2026; a national consensus statement, endorsed by Breakthrough T1D, the Diabetes Technology Network, Diabetes UK, the DSN Forum, the Royal College of Nursing and Trend Diabetes), operationalised through a self-assessment tool. These bodies endorse the national framework. They do not endorse Learn with Grace, and Learn with Grace is not affiliated with, accredited by, or approved by any of them. That framework is itself a self-assessment, and so is this, so mapping our tiers onto it is a fair, like-for-like comparison. Every tier here is earned at a graded gate, so where you sit is shown by the work, not self-declared.
The framework describes what you understand, not what you are licensed to do. We use the same domains to describe depth of understanding, never to confer clinical competence, scope of practice or permission to act. A strong grasp of the material does not make a non-clinician a clinician, and clinical decisions about real doses always sit with your care team, every time.
Recognise the device, manage the emergency, signpost to the specialist team.
Interpret CGM and pump data, work with the algorithm differences, manage intercurrent illness.
Algorithm internals, advanced interpretation, critical appraisal. We teach the why; hands-on device handling still needs the kit and patient contact.
Service development, publication, mentorship, policy. Shown by doing the work, not by a module set; the continuous, up-to-date surface that opens once all thirty are passed.
Each tier is reached the same way: ten modules, each ending in ten rotating questions where more than one answer is plausible, passed at nine of ten. Score low and the path goes deep; score mid and you get a targeted top-up; score high and you go straight to the run.
You leave with a Passport
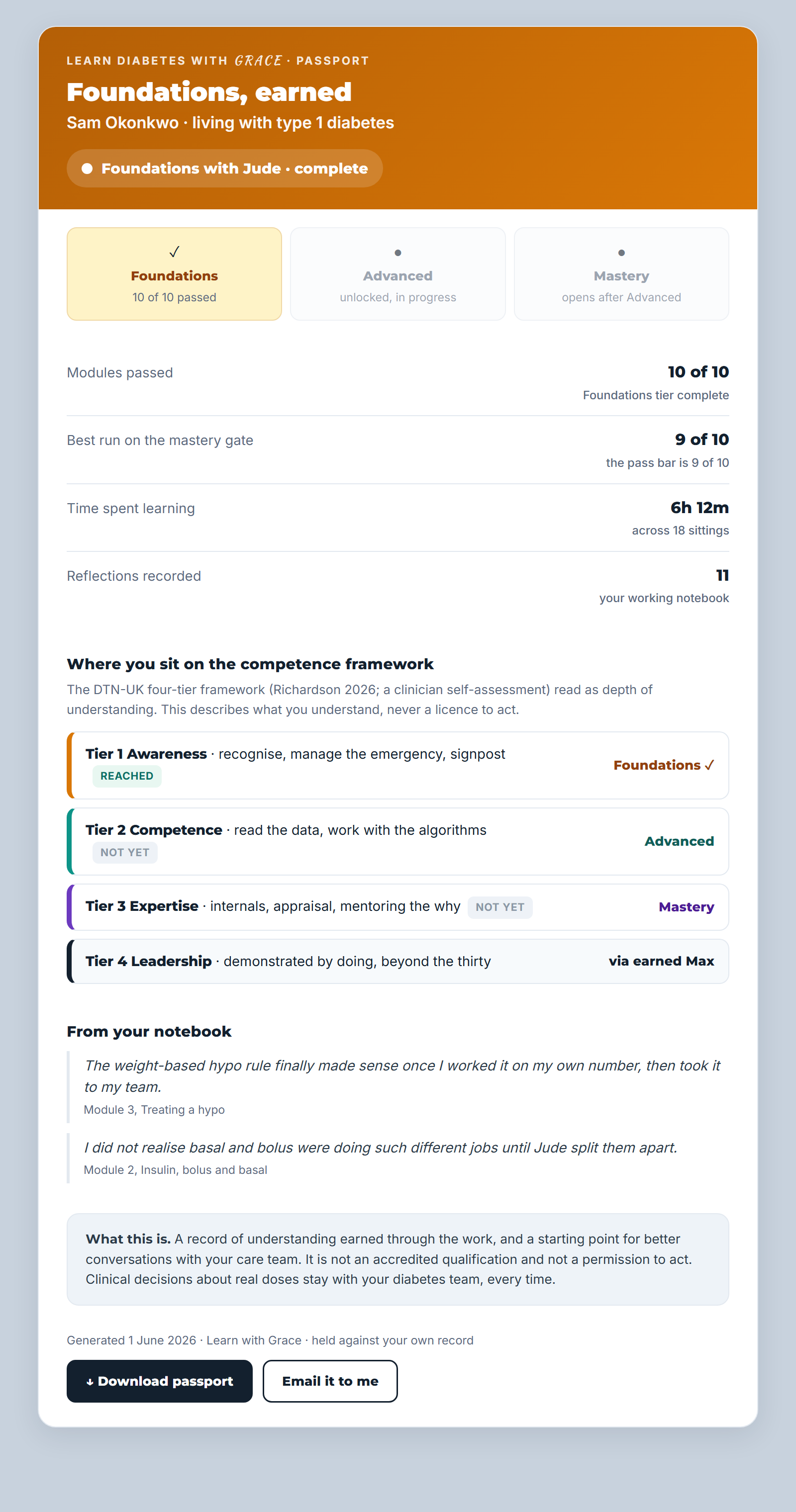
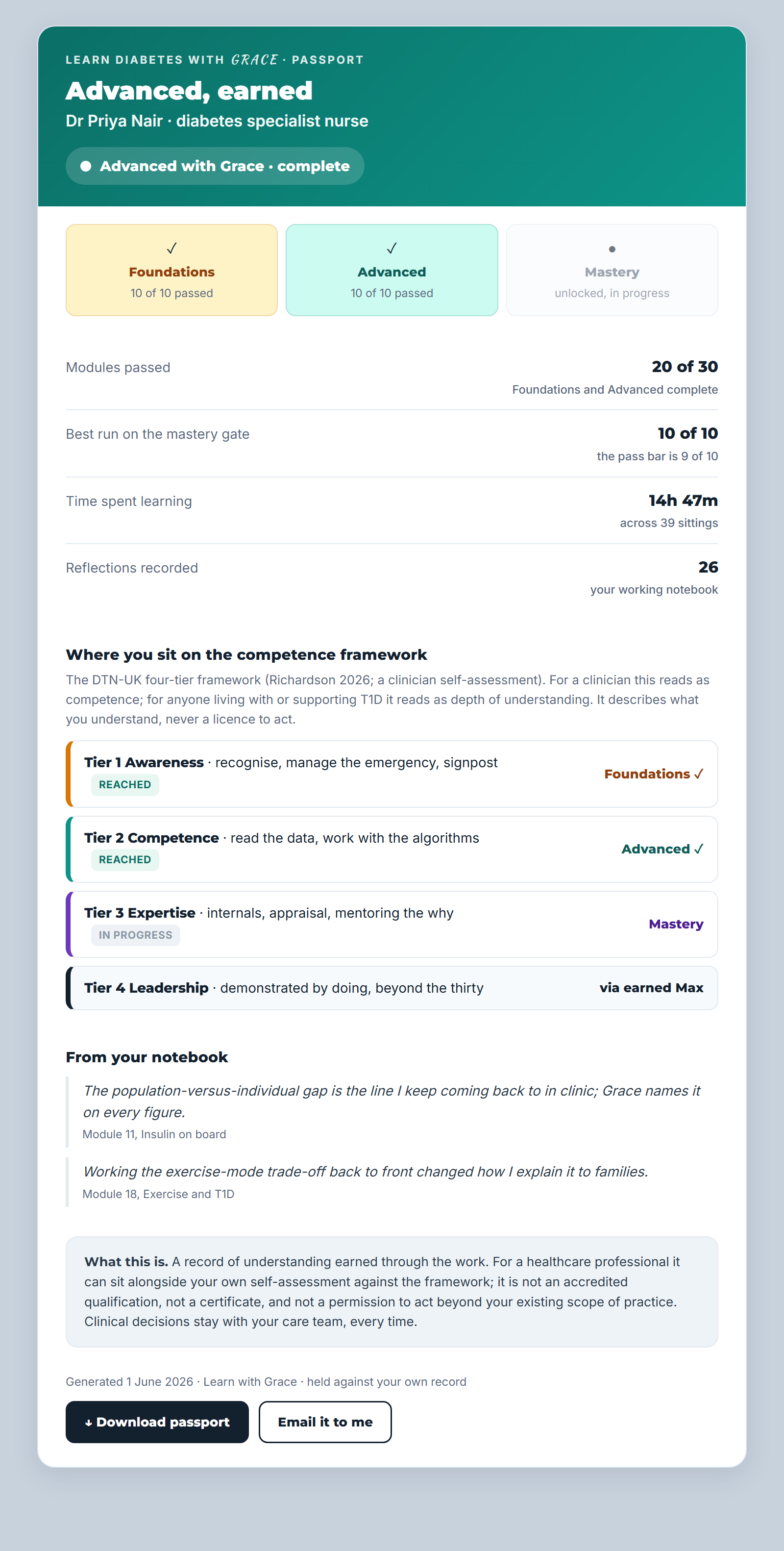
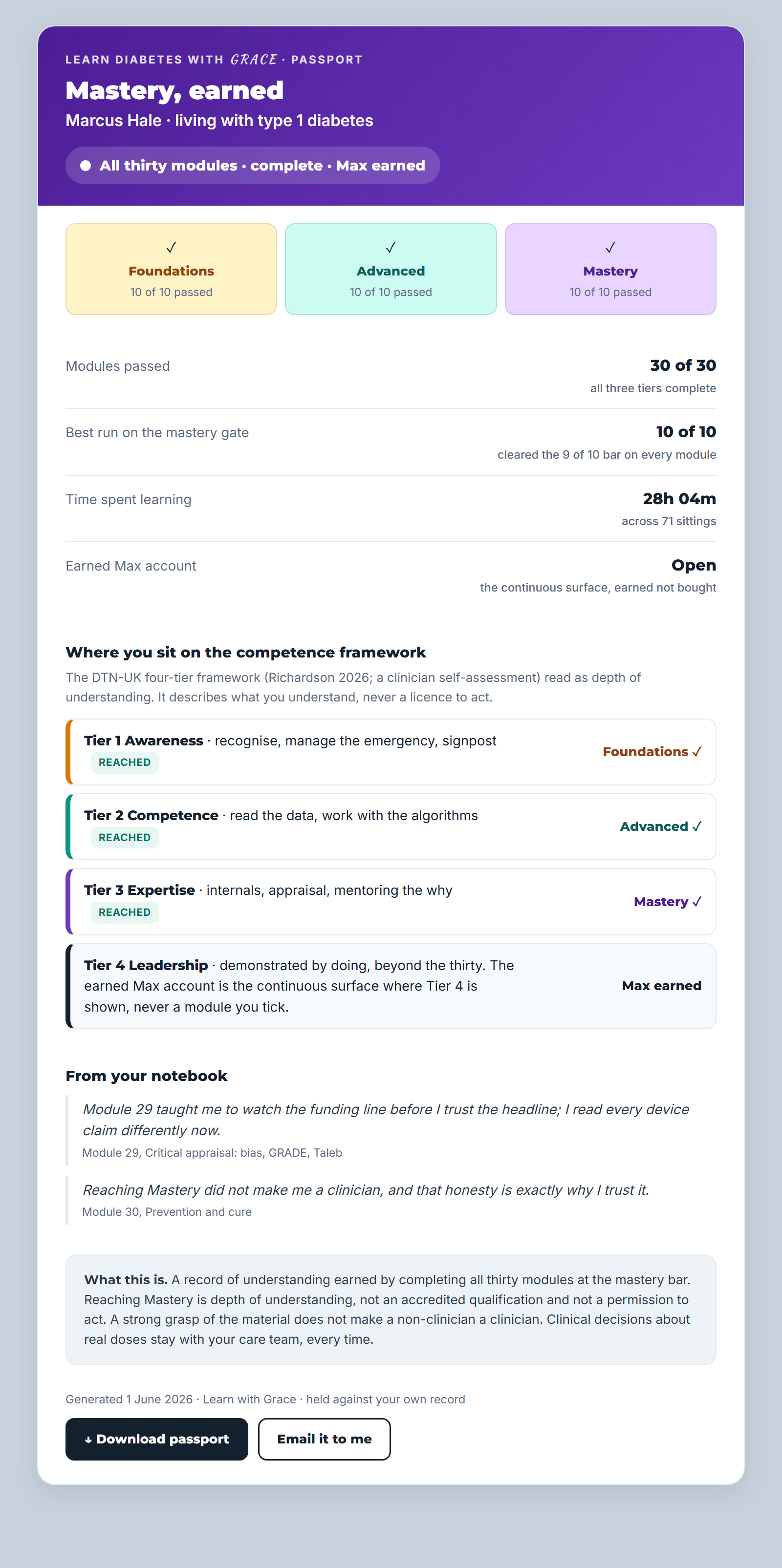
Every tier you pass is recorded in an exportable Learn with Grace Passport: the modules you completed, the time you put in, your reflections, and where you sit against the four-tier framework. It is yours to download or email; not a certificate, not a licence to act; proof of the work, in your hands.
See the full framework, tier by tier →
The Passport as it grows with you, Foundations through to Mastery and the earned Max account.
Educational tools
The eight Explorers
Eight deterministic educational tools, each grounded in the same evidence base as Grace. None of them outputs a personalised dose. Every result is a starting point for a conversation with your diabetes care team, not the end of one.
Live now
Start learning in the app
Grace is part of the GNL app, where access and the trial are handled. Open the app to start the curriculum, or read more about how Grace is built and kept safe.
Sponsor a free account for someone on the waiting list: support Grace on Buy Me a Coffee.
Grace is an educational advisor. She does not give personalised insulin doses. She does not tell you what to do with your glucose. Every numeric output is a population-average estimate at a given total daily dose; the figure that fits your day belongs to the care team who knows you.